Download as pdf or txt
You might also like
- Pancreatic Cancer - Case AnalysisDocument37 pagesPancreatic Cancer - Case AnalysisMavy CantonNo ratings yet
- How To Reverse Type 2 DiabetesDocument20 pagesHow To Reverse Type 2 Diabetesjrobinhill100% (1)
- E-Ahpba 2013 Congress Book Add-OnDocument30 pagesE-Ahpba 2013 Congress Book Add-OnSvet MedicineNo ratings yet
- Inflammatory Potential of Diet and Risk of Laryngeal Cancer in A Case-Control Study From ItalyDocument8 pagesInflammatory Potential of Diet and Risk of Laryngeal Cancer in A Case-Control Study From ItalyFrizka ApriliaNo ratings yet
- Alcohol Consumption and The Risk of Prostate Cancer A Dose-Response MetaAnalysisDocument17 pagesAlcohol Consumption and The Risk of Prostate Cancer A Dose-Response MetaAnalysisGabriela VazquezNo ratings yet
- Nutrients: Association Between Alcohol Consumption, Folate Intake, and Risk of Pancreatic Cancer: A Case-Control StudyDocument9 pagesNutrients: Association Between Alcohol Consumption, Folate Intake, and Risk of Pancreatic Cancer: A Case-Control StudysyifaNo ratings yet
- Am. J. Epidemiol. 2009 Heinen 1233 42Document10 pagesAm. J. Epidemiol. 2009 Heinen 1233 42FP ErsidaNo ratings yet
- Inflammatory Potential of Diet and Risk of Colorectal Cancer A Casecontrol Study From ItalyDocument7 pagesInflammatory Potential of Diet and Risk of Colorectal Cancer A Casecontrol Study From ItalyHenrique VidalNo ratings yet
- Alcohol Consumption and Risk of Colon Cancer: Evidence From The National Health and Nutrition Examination Survey I Epidemiologic Follow-Up StudyDocument10 pagesAlcohol Consumption and Risk of Colon Cancer: Evidence From The National Health and Nutrition Examination Survey I Epidemiologic Follow-Up StudyIra FerawatiNo ratings yet
- Dietary Flavonols Intake and Risk of Esophageal and Gastric Cancer: A Meta-Analysis of Epidemiological StudiesDocument12 pagesDietary Flavonols Intake and Risk of Esophageal and Gastric Cancer: A Meta-Analysis of Epidemiological StudiesJose correNo ratings yet
- Risk of Colon Cancer and Coffee, Tea, and Sugar-Sweetened Soft Drink Intake: Pooled Analysis of Prospective Cohort StudiesDocument13 pagesRisk of Colon Cancer and Coffee, Tea, and Sugar-Sweetened Soft Drink Intake: Pooled Analysis of Prospective Cohort StudiesDevi KharismawatiNo ratings yet
- Alkohol 2Document10 pagesAlkohol 2Yuvhendmindo ShahcogaNo ratings yet
- Journal of A Ffective Disorders: Review ArticleDocument8 pagesJournal of A Ffective Disorders: Review ArticleLorena ErnstNo ratings yet
- The New England Journal of MedicineDocument12 pagesThe New England Journal of MedicineElyzabeth BonnesNo ratings yet
- Gut&Liver 2019 Jan 114 Alcohol Consumption Can Reduce The Risk of Gallstone Disease - A Systematic Review With A Dose-Response Meta-Analysis of Case-Control and Cohort StudieseDocument18 pagesGut&Liver 2019 Jan 114 Alcohol Consumption Can Reduce The Risk of Gallstone Disease - A Systematic Review With A Dose-Response Meta-Analysis of Case-Control and Cohort StudieseByung ChaNo ratings yet
- Cancro-Y-JeandE-Giovannucci-Int-J-Cancer CaféDocument29 pagesCancro-Y-JeandE-Giovannucci-Int-J-Cancer CaféMonica SáezNo ratings yet
- Coffee and Cancer Umbrella ReviewDocument12 pagesCoffee and Cancer Umbrella ReviewNicolás MurilloNo ratings yet
- A Metaanalysis On Alcohol Consumption and Risk of EndometriosisDocument10 pagesA Metaanalysis On Alcohol Consumption and Risk of EndometriosiskiranNo ratings yet
- 43 FullDocument9 pages43 Fullnayeta levi syahdanaNo ratings yet
- 2021 - Coffee Consumption and AllCause, Cardiovascular, and Cancer Mortality in An Adult Mediterranean PopulationDocument13 pages2021 - Coffee Consumption and AllCause, Cardiovascular, and Cancer Mortality in An Adult Mediterranean Populationjimmyneutron1337No ratings yet
- Increased Risk of Microscopic Colitis With Use of Proton Pump Inhibitors and Non-Steroidal Anti-In Ammatory DrugsDocument11 pagesIncreased Risk of Microscopic Colitis With Use of Proton Pump Inhibitors and Non-Steroidal Anti-In Ammatory DrugsFabrizzio BardalesNo ratings yet
- AnisaDocument7 pagesAnisaBoedyNo ratings yet
- Regular Consumption of Dark Chocolate Is Associated With Low Serum Concentrations of C-Reactive Protein in A Healthy Italian PopulationDocument7 pagesRegular Consumption of Dark Chocolate Is Associated With Low Serum Concentrations of C-Reactive Protein in A Healthy Italian Populationgeraldi23No ratings yet
- ArticuloDocument9 pagesArticuloElyzabeth BonnesNo ratings yet
- Dietary Fibre and The Risk of Colorectal Cancer: A Case-Control StudyDocument6 pagesDietary Fibre and The Risk of Colorectal Cancer: A Case-Control StudyEmanuel BotezatNo ratings yet
- Out 4Document14 pagesOut 4Muhammad Ali Sidik SNo ratings yet
- Manejo de Articulo Cientifico PDFDocument9 pagesManejo de Articulo Cientifico PDFDANIELA ALEJANDRA PEDRAZA ARTEAGANo ratings yet
- Activity 5 - 6bias and ConfoundingDocument4 pagesActivity 5 - 6bias and ConfoundingkfentonNo ratings yet
- Lab 8 Allen - Perception of AlcoholDocument7 pagesLab 8 Allen - Perception of Alcoholapi-583318017No ratings yet
- Tutorial 5Document6 pagesTutorial 5Wijaya AndiNo ratings yet
- Diabetes e Risco de QuedaDocument7 pagesDiabetes e Risco de QuedaanamartaafranciscoNo ratings yet
- Print This OneDocument11 pagesPrint This Oneapi-596913754No ratings yet
- Quality of Life of Children With Type 1 Diabetes: A Systematic ReviewDocument12 pagesQuality of Life of Children With Type 1 Diabetes: A Systematic ReviewNila Sari ChandraNo ratings yet
- Migraine and Body Mass Index Categories: A Systematic Review and Meta-Analysis of Observational StudiesDocument14 pagesMigraine and Body Mass Index Categories: A Systematic Review and Meta-Analysis of Observational StudiesRetno ManggalihNo ratings yet
- Alimentos, Nutrientes e Risco de Câncer de Boca e FaringeDocument7 pagesAlimentos, Nutrientes e Risco de Câncer de Boca e FaringePela Minha SaúdeNo ratings yet
- Downloaded From Uva-Dare, The Institutional Repository of The University of Amsterdam (Uva)Document28 pagesDownloaded From Uva-Dare, The Institutional Repository of The University of Amsterdam (Uva)Indah Putri permatasariNo ratings yet
- JAMA 2003 Lieberman 2959 67Document9 pagesJAMA 2003 Lieberman 2959 67Jeff Aloys GunawanNo ratings yet
- Introduction of PharmacologyDocument11 pagesIntroduction of PharmacologyDarnalet OngNo ratings yet
- Ciggarette Smokin and Alcohol Consumption To Colorectal CancerDocument7 pagesCiggarette Smokin and Alcohol Consumption To Colorectal CancerPutri Atthariq IlmiNo ratings yet
- Alcohol As A Risk Factor For Type 2 Diabetes: A Systematic Review and Meta-AnalysisDocument10 pagesAlcohol As A Risk Factor For Type 2 Diabetes: A Systematic Review and Meta-AnalysisMimbel WimbelNo ratings yet
- Dietary Patterns and Colorectal Cancer: Systematic Review and Meta-AnalysisDocument10 pagesDietary Patterns and Colorectal Cancer: Systematic Review and Meta-AnalysisDidi Nurhadi IllianNo ratings yet
- Nurullia R - G4a017075 - CmeDocument12 pagesNurullia R - G4a017075 - CmeNurullia RahmawatiNo ratings yet
- Zhou 2013fgDocument9 pagesZhou 2013fgMuhammad Wim AdhitamaNo ratings yet
- Diet Soft Drink Consumption Is Associated With The Metabolic Syndrome: A Two Sample ComparisonDocument18 pagesDiet Soft Drink Consumption Is Associated With The Metabolic Syndrome: A Two Sample ComparisonPK MilkyNo ratings yet
- Alcohol Consumption Patients Adenomatous Polyps: in With ColorectalDocument4 pagesAlcohol Consumption Patients Adenomatous Polyps: in With ColorectalJae Yong LeeNo ratings yet
- Chan 2009Document12 pagesChan 2009veaceslav coscodanNo ratings yet
- Chang2010 11Document12 pagesChang2010 11Jose Angel AbadíaNo ratings yet
- Original Article: Fried Foods, Olive Oil and Colorectal CancerDocument4 pagesOriginal Article: Fried Foods, Olive Oil and Colorectal CancerFrancisco BetancourtNo ratings yet
- Abstract JURNAL SKRIPSI 2Document11 pagesAbstract JURNAL SKRIPSI 2Ade RatnasariNo ratings yet
- The Relation of Moderate Alcohol Consumption To Hyperuricemia in A Rural General PopulationDocument11 pagesThe Relation of Moderate Alcohol Consumption To Hyperuricemia in A Rural General PopulationsyifaNo ratings yet
- Bmj.c4229.Full Httpis - Gdca8wlvDocument8 pagesBmj.c4229.Full Httpis - Gdca8wlvrianiputriNo ratings yet
- NutritionsDocument9 pagesNutritionsPutra EkaNo ratings yet
- Am J Clin Nutr 2010 Vrieling 471 90Document21 pagesAm J Clin Nutr 2010 Vrieling 471 90SunardiasihNo ratings yet
- Ohkuma, 2015. META ANÁLISE - ANC E ABESIDADEDocument8 pagesOhkuma, 2015. META ANÁLISE - ANC E ABESIDADEMaria MachadoNo ratings yet
- Epidemiology ReviewDocument10 pagesEpidemiology ReviewSaurabhNo ratings yet
- Risk Factors For Noncommunicable Chronic Diseases in Women in China: Surveillance EffortsDocument11 pagesRisk Factors For Noncommunicable Chronic Diseases in Women in China: Surveillance Effortssamson jinaduNo ratings yet
- Caffeine and Kidney DiseasesDocument7 pagesCaffeine and Kidney DiseasesOlomoniyi PreciousNo ratings yet
- General Review 5Document9 pagesGeneral Review 5Abdulphatah Mohamed IbrahimNo ratings yet
- Esteves 2012Document15 pagesEsteves 2012Nawaf RuwailiNo ratings yet
- FMLRDocument7 pagesFMLRapi-550114496No ratings yet
- BMJ 2014-Tsilidis - Type 2 Diabetes and Cancer-Umbrella Review of Meta-Analyses of Observational StudiesDocument11 pagesBMJ 2014-Tsilidis - Type 2 Diabetes and Cancer-Umbrella Review of Meta-Analyses of Observational StudiesPatrick Leonard G. CoNo ratings yet
- Optimizing Advanced Therapies in Ulcerative Colitis: Is Your Practice Up to Date? A Focus on Clinical Evidence and Guideline RecommendationsFrom EverandOptimizing Advanced Therapies in Ulcerative Colitis: Is Your Practice Up to Date? A Focus on Clinical Evidence and Guideline RecommendationsNo ratings yet
- Daftar PustakaDocument16 pagesDaftar PustakaAfif Al FatihNo ratings yet
- What Is Research: DefinitionDocument4 pagesWhat Is Research: DefinitionAfif Al FatihNo ratings yet
- Yeaaaah 23456789Document1 pageYeaaaah 23456789Afif Al FatihNo ratings yet
- YeaaaahDocument1 pageYeaaaahAfif Al FatihNo ratings yet
- Clinical EndocrinologyDocument52 pagesClinical EndocrinologyAfif Al FatihNo ratings yet
- Activities and IntentsDocument47 pagesActivities and IntentsAfif Al FatihNo ratings yet
- PyelonephritisDocument9 pagesPyelonephritisAfif Al FatihNo ratings yet
- Immunodeficiency: Principles of ImmunologyDocument16 pagesImmunodeficiency: Principles of ImmunologyAfif Al FatihNo ratings yet
- Absen Cwek PaiDocument2 pagesAbsen Cwek PaiAfif Al FatihNo ratings yet
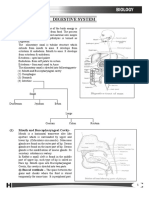
- Digestive System AnaDocument8 pagesDigestive System AnaTADERA TEFFANIE NICOLE O. BSN 1-YA-9No ratings yet
- NCMB 316Document46 pagesNCMB 316andreatrojilloNo ratings yet
- Diabetes MellitusDocument31 pagesDiabetes MellitusElenaCondratscribdNo ratings yet
- Healthy Low-Fat Diets For Dogs With Special Dietary NeedsDocument5 pagesHealthy Low-Fat Diets For Dogs With Special Dietary NeedsNicholay AtanassovNo ratings yet
- GIT - Dr. Allam 2021 PDFDocument47 pagesGIT - Dr. Allam 2021 PDFMohammedNo ratings yet
- Trans Chapter 16Document5 pagesTrans Chapter 16رجمه ديوانNo ratings yet
- Literature Review On Broiler ChickenDocument7 pagesLiterature Review On Broiler Chickenafdtalblw100% (1)
- Herbs For PancreasDocument3 pagesHerbs For PancreasStefanie LevinaWolfNo ratings yet
- Koncpt GB PantDocument96 pagesKoncpt GB Pantoddie333No ratings yet
- RPN Post Review TestDocument69 pagesRPN Post Review Testfairwoods94% (17)
- AP Biology 018 - Positive and Negative Feedback Loops Video Review SheetDocument2 pagesAP Biology 018 - Positive and Negative Feedback Loops Video Review SheetKaelyn BrushettNo ratings yet
- (Artigo) (Anatomia) Gastroduodenal Artery - Single Key For Many Locks Desai (2019)Document11 pages(Artigo) (Anatomia) Gastroduodenal Artery - Single Key For Many Locks Desai (2019)Beatriz BelottiNo ratings yet
- Gastrointestinal Physiology: By: Zewdu JimaDocument77 pagesGastrointestinal Physiology: By: Zewdu JimaZewdu Jima100% (1)
- Endocrine SystemDocument32 pagesEndocrine Systemlee bon hukNo ratings yet
- 2 - Control & CoordinationDocument11 pages2 - Control & CoordinationSANCHIT BAWEJANo ratings yet
- Egregious Eleven of Type 2 Diabetes Mellitus - My Endo ConsultDocument20 pagesEgregious Eleven of Type 2 Diabetes Mellitus - My Endo Consultakbar011512No ratings yet
- Case History: Year 8 SemesterDocument26 pagesCase History: Year 8 SemesterNarmada PemathilakaNo ratings yet
- Antidiabetic Effect of Cephalandra Indica Q in Diabetic RatsDocument11 pagesAntidiabetic Effect of Cephalandra Indica Q in Diabetic Ratsdrkapilkohli3514No ratings yet
- Diabetes Melitus 2 DkaDocument104 pagesDiabetes Melitus 2 DkaLaiza Fatima LacsonNo ratings yet
- Prophesy Again Pastor Andrew Henriques WWW - Prophesyagain.com ...Document2 pagesProphesy Again Pastor Andrew Henriques WWW - Prophesyagain.com ...rohan777No ratings yet
- Outline: Relative Measurements of Alimentary TractsDocument9 pagesOutline: Relative Measurements of Alimentary TractsProfessor GhoulNo ratings yet
- Tle 9 10 Housekeeping Q4 Week 5 6Document13 pagesTle 9 10 Housekeeping Q4 Week 5 6Ellen Maskariño100% (2)
- What Is Type 2 DiabetesDocument10 pagesWhat Is Type 2 DiabetesCyron Elden T. BodegasNo ratings yet
- CSEC Biology - AssimilationDocument1 pageCSEC Biology - AssimilationRaveena SinghNo ratings yet
- Mammalian System-01 (Digestive System)Document35 pagesMammalian System-01 (Digestive System)Saumya99No ratings yet
- Digestive SystemDocument64 pagesDigestive SystemAyro Business CenterNo ratings yet
- Lecture 28 - Pathology of DiabetesDocument34 pagesLecture 28 - Pathology of Diabetesapi-3703352100% (4)