Download as pdf or txt
You might also like
- Ari Whitten The Ultimate Guide To Red Light TherapyDocument41 pagesAri Whitten The Ultimate Guide To Red Light TherapyJulianne Bsc94% (36)
- Vitamin D and CancerDocument221 pagesVitamin D and CancerAna Ferreira50% (2)
- 1173 FullDocument6 pages1173 FullLeo TongNo ratings yet
- Prospective Study of UV Exposure and Cancer Incidence Among Swedish WomenDocument10 pagesProspective Study of UV Exposure and Cancer Incidence Among Swedish WomenAlexander HunterNo ratings yet
- Journal 1Document9 pagesJournal 1Ambar pudjiantoNo ratings yet
- Krause Et Al 2006 - UV Radiation and Cancer PreventionDocument5 pagesKrause Et Al 2006 - UV Radiation and Cancer PreventionKasumi PhantomhiveNo ratings yet
- A 0240105Document5 pagesA 0240105International Organization of Scientific Research (IOSR)No ratings yet
- Photobiomodulation Compressed PDFDocument27 pagesPhotobiomodulation Compressed PDFluanadumitruNo ratings yet
- BMJ 2013 346:F2360 (: Free Full-Text BMJ Article PDF Pubmed® AbstractDocument3 pagesBMJ 2013 346:F2360 (: Free Full-Text BMJ Article PDF Pubmed® AbstractintrascribdNo ratings yet
- Cancer in Working-Age Is Not Associated With Childhood AdversitiesDocument6 pagesCancer in Working-Age Is Not Associated With Childhood AdversitiesBadger6No ratings yet
- 42universitystudents PDFDocument7 pages42universitystudents PDFEl MarcelokoNo ratings yet
- Preventive Medicine: ArticleinfoDocument5 pagesPreventive Medicine: ArticleinfoEl MarcelokoNo ratings yet
- Epidemiology - Exercises. Gaetano MarroneDocument4 pagesEpidemiology - Exercises. Gaetano Marronemillion assefaNo ratings yet
- LiteraturereviewDocument8 pagesLiteraturereviewapi-311113195No ratings yet
- Vitamin D Intake and Incidence of Multiple SclerosisDocument6 pagesVitamin D Intake and Incidence of Multiple SclerosisDianne Faye ManabatNo ratings yet
- Copia de Final 2019-2020 No Answers PDFDocument20 pagesCopia de Final 2019-2020 No Answers PDFadkfnlsºNo ratings yet
- Metabolic Syndrome and Breast Cancer in The Me-Can (Metabolic Syndrome and Cancer) ProjectDocument10 pagesMetabolic Syndrome and Breast Cancer in The Me-Can (Metabolic Syndrome and Cancer) ProjectPanji Agung KhrisnaNo ratings yet
- Early-Onset Basal Cell CarcinomaDocument11 pagesEarly-Onset Basal Cell CarcinomajxmackNo ratings yet
- Estrés y Cáncer de MamaDocument6 pagesEstrés y Cáncer de MamaIsa SalazarNo ratings yet
- Sex Differences in Cancer Risk and Survival: A Swedish Cohort StudyDocument11 pagesSex Differences in Cancer Risk and Survival: A Swedish Cohort Studyfiora.ladesvitaNo ratings yet
- Articulo - Gargaras para Infecciones Vias RespiratoriasDocument6 pagesArticulo - Gargaras para Infecciones Vias RespiratoriasRaulNo ratings yet
- Annotated BibliographyDocument12 pagesAnnotated Bibliographyapi-448765847No ratings yet
- Risk Factors For Dementia in The Ninth Decade of Life and Beyond: A Study of The Lothian Birth Cohort 1921Document10 pagesRisk Factors For Dementia in The Ninth Decade of Life and Beyond: A Study of The Lothian Birth Cohort 1921yeremias setyawanNo ratings yet
- 10 1002@msc 1498Document13 pages10 1002@msc 1498Ricardo PietrobonNo ratings yet
- VM 2073 Review of Use of Evidence (Epidemiology) Years 1 And2Document61 pagesVM 2073 Review of Use of Evidence (Epidemiology) Years 1 And2KerolusMouradNo ratings yet
- Healing Whispers : Surviving Throat, Bone and Skin Cancer Despite all OddsFrom EverandHealing Whispers : Surviving Throat, Bone and Skin Cancer Despite all OddsNo ratings yet
- Striae Distensae - A Comprehensive Review and Evidence-Based Evaluation of Prophylaxis and TreatmentDocument54 pagesStriae Distensae - A Comprehensive Review and Evidence-Based Evaluation of Prophylaxis and TreatmentigorfragaNo ratings yet
- Nej MC 082208Document2 pagesNej MC 082208anggiNo ratings yet
- 10 1111@jdv 15494Document8 pages10 1111@jdv 15494ahmad saadNo ratings yet
- Research Letter: Risk of Depression Among Patients With Acne in The U.K.: A Population-Based Cohort StudyDocument2 pagesResearch Letter: Risk of Depression Among Patients With Acne in The U.K.: A Population-Based Cohort StudyadhastriNo ratings yet
- DanielDocument8 pagesDanielLora MyrickNo ratings yet
- Xu 2006Document9 pagesXu 2006Cristiane Leao dos SantosNo ratings yet
- 6 - Cancer Risk in 680 000 People Exposed To Computed Tomography Scans in Childhood or Adolescence - Data Linkage Study of 11 Million AustraliansDocument18 pages6 - Cancer Risk in 680 000 People Exposed To Computed Tomography Scans in Childhood or Adolescence - Data Linkage Study of 11 Million AustraliansEdis DjedovicNo ratings yet
- Cancer Risk Among Patients With Type 2 Diabetes Mellitus: A Population-Based Prospective Study in ChinaDocument7 pagesCancer Risk Among Patients With Type 2 Diabetes Mellitus: A Population-Based Prospective Study in ChinaAndreea KNo ratings yet
- Quality of Life of Children With Type 1 Diabetes: A Systematic ReviewDocument12 pagesQuality of Life of Children With Type 1 Diabetes: A Systematic ReviewNila Sari ChandraNo ratings yet
- Evidence On The Prevention of Cancer PDFDocument10 pagesEvidence On The Prevention of Cancer PDFMonicaNo ratings yet
- Sunlight & CancerDocument13 pagesSunlight & CancerMarcoSaliniNo ratings yet
- Abstracts 853 125: 4 OCTOBER 2005: BackgroundDocument1 pageAbstracts 853 125: 4 OCTOBER 2005: BackgroundkelbmutsNo ratings yet
- 2006, Vol.24, Issues 2, Women's DermatologyDocument145 pages2006, Vol.24, Issues 2, Women's DermatologyRizweta DestinNo ratings yet
- Cancer Entangled: Anticipation, Acceleration, and the Danish StateFrom EverandCancer Entangled: Anticipation, Acceleration, and the Danish StateRikke Sand AndersenNo ratings yet
- Support TD7 2024 StudentsDocument2 pagesSupport TD7 2024 StudentsMoira RazafimalalaNo ratings yet
- Examenes Radiologicos y Riesgo de Cancer en PacientesDocument27 pagesExamenes Radiologicos y Riesgo de Cancer en PacientesMaría Isabel Clara Aponte OrtizNo ratings yet
- CondylomaDocument4 pagesCondylomaOchabianconeriNo ratings yet
- Epidemiological StudiesDocument25 pagesEpidemiological StudiesDr Sumit KarNo ratings yet
- The 2003 Health Survey of Penyffordd Results of The Cank Questionnaire Survey Chris Busby PHD Helen Rowe BaDocument7 pagesThe 2003 Health Survey of Penyffordd Results of The Cank Questionnaire Survey Chris Busby PHD Helen Rowe BaAkmens Raimonds - RAYSTARNo ratings yet
- Chronic Periodontal Disease A Proxy For Increased Cancer RiskDocument7 pagesChronic Periodontal Disease A Proxy For Increased Cancer RiskRaiNo ratings yet
- Artikel Cancer PayudaraDocument6 pagesArtikel Cancer PayudaraAndi MarwansyahNo ratings yet
- New England Journal Medicine: The ofDocument9 pagesNew England Journal Medicine: The ofIsmail Eko SaputraNo ratings yet
- 85 PDFDocument3 pages85 PDFAdi PranataNo ratings yet
- Prevalence of Risk Factors For Breast Cancer in German Airline Cabin Crew: A Cross-Sectional StudyDocument5 pagesPrevalence of Risk Factors For Breast Cancer in German Airline Cabin Crew: A Cross-Sectional StudyYudi SupartaNo ratings yet
- Leisure Time Physical Activity and The Risk of Type 2 Diabetes in Men and Women From The General PopulationDocument8 pagesLeisure Time Physical Activity and The Risk of Type 2 Diabetes in Men and Women From The General PopulationMaría HurtadoNo ratings yet
- The Global Burden of Selected Occupational Disease and Injury Risks: Methodology andDocument21 pagesThe Global Burden of Selected Occupational Disease and Injury Risks: Methodology andconnectessamNo ratings yet
- Doi150043association of Skin Cancer and Indoor Tanning in Sexual Minority Men and WomenDocument9 pagesDoi150043association of Skin Cancer and Indoor Tanning in Sexual Minority Men and WomenKen KatzNo ratings yet
- Season of Interview and Self-Report of Summer Sun Protection BehaviorsDocument10 pagesSeason of Interview and Self-Report of Summer Sun Protection BehaviorsEl MarcelokoNo ratings yet
- Treating Facial Acne in Adolescents and Young Adults With Auriculoacupuncture and AuriculotherapyDocument16 pagesTreating Facial Acne in Adolescents and Young Adults With Auriculoacupuncture and AuriculotherapyPedro MaiaNo ratings yet
- Copy1 Chapter 1Document40 pagesCopy1 Chapter 1X And ZNo ratings yet
- Descriptive EpidemiologyDocument25 pagesDescriptive Epidemiologydocsaurabh777No ratings yet
- Ca CervikDocument7 pagesCa CervikHendra SusantoNo ratings yet
- Dental X Rays and The Risk of Thyroid Cancer A Case Control StudyDocument8 pagesDental X Rays and The Risk of Thyroid Cancer A Case Control StudyEm EryNo ratings yet
- Prospective Study Cohort Study: Assis - Prof.Dr Diaa Marzouk Community MedicineDocument30 pagesProspective Study Cohort Study: Assis - Prof.Dr Diaa Marzouk Community MedicineMona SamiNo ratings yet
- Advance Epi & Direct Acyclic GraphDocument14 pagesAdvance Epi & Direct Acyclic GraphPurnima VermaNo ratings yet
- USER MANUAL Psoriasis Vitiligo LampDocument50 pagesUSER MANUAL Psoriasis Vitiligo Lamplixo_mail50% (6)
- (Sinecatechins: Key ReferencesDocument14 pages(Sinecatechins: Key ReferencesFerdy Arif FadhilahNo ratings yet
- Dcbecf 33Document7 pagesDcbecf 33Nida Dwi ArifaNo ratings yet
- Skin Physiology: Lecturer:Dr Herman Mulijadi MS, SPKPDocument59 pagesSkin Physiology: Lecturer:Dr Herman Mulijadi MS, SPKPJosephine SNo ratings yet
- Ban Xuất Huyết BatemanDocument7 pagesBan Xuất Huyết BatemanhoangNo ratings yet
- Prediksi Soal Utbk Bahasa Inggris 2022Document4 pagesPrediksi Soal Utbk Bahasa Inggris 2022Aulia Azhar0% (1)
- ACTIVITY SHEETS IN SCIENCE 4 Week 7Document3 pagesACTIVITY SHEETS IN SCIENCE 4 Week 7Princes100% (3)
- Oleh Ilham Syifaur Pembimbing Dr. Rahmad Syuhada, Sp. MDocument20 pagesOleh Ilham Syifaur Pembimbing Dr. Rahmad Syuhada, Sp. MMeta MedianaNo ratings yet
- Vitamin D Deficiency Causes and Treatment Vol1Document105 pagesVitamin D Deficiency Causes and Treatment Vol1Poongkodi KNo ratings yet
- 10 Best Ways To Increase Dopamine Levels NaturallyDocument9 pages10 Best Ways To Increase Dopamine Levels Naturallysmit_ghoseNo ratings yet
- SungazingDocument8 pagesSungazingPaul SavvyNo ratings yet
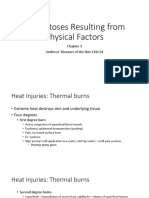
- Andrews - Chapter 3 - Dermatosis Resulting From Physical FactorsDocument71 pagesAndrews - Chapter 3 - Dermatosis Resulting From Physical FactorsAngeli Ramos-EstrellaNo ratings yet
- The Clinical Importance of Vitamin D (Cholecalciferol) : A Paradigm Shift With Implications For All Healthcare ProvidersDocument82 pagesThe Clinical Importance of Vitamin D (Cholecalciferol) : A Paradigm Shift With Implications For All Healthcare Providersdevin mahendikaNo ratings yet
- Results and DiscussionDocument2 pagesResults and Discussionjyoruta198No ratings yet
- How To Read and Really Use An Item Analysis: Nurse EducatorDocument6 pagesHow To Read and Really Use An Item Analysis: Nurse EducatorTuấn Anh VũNo ratings yet
- Complementary FeedingDocument29 pagesComplementary FeedingRebecca BrandonNo ratings yet
- Natty Lifter's Guide To Supplementation - Build Quality Gainz W - Out SteroidsDocument9 pagesNatty Lifter's Guide To Supplementation - Build Quality Gainz W - Out SteroidsMouhNo ratings yet
- Ccupational and Environmental OptometryDocument20 pagesCcupational and Environmental OptometryRachana KafleNo ratings yet
- Chapter 2 Overcoming MS Handbook - SamplerDocument20 pagesChapter 2 Overcoming MS Handbook - SamplerAllen & UnwinNo ratings yet
- Beach Safety Workbook777 PDFDocument64 pagesBeach Safety Workbook777 PDFanna petersonNo ratings yet
- Sunlight & CancerDocument13 pagesSunlight & CancerMarcoSaliniNo ratings yet
- Advances in Malignant Melanoma - Clinical and Research PerspectivesDocument264 pagesAdvances in Malignant Melanoma - Clinical and Research PerspectivesInternational Medical PublisherNo ratings yet
- Market Analysis of Everyuth Derma Care RangeDocument58 pagesMarket Analysis of Everyuth Derma Care RangeHarsha SilanNo ratings yet
- Journal of Photochemistry and Photobiology B: BiologyDocument6 pagesJournal of Photochemistry and Photobiology B: BiologygerardosloveNo ratings yet
- Whitening Injection Informed ConsentDocument3 pagesWhitening Injection Informed ConsentCalix Jr Rambuyon0% (1)
- Anatomoclinical Confrontation Between Melanoma, Solar Lentigo and Seborrheic Keratosis: A Case ReportDocument4 pagesAnatomoclinical Confrontation Between Melanoma, Solar Lentigo and Seborrheic Keratosis: A Case ReportIJAR JOURNALNo ratings yet
- Mike Adams - The Healing Power of Sunlight Vitamin DDocument26 pagesMike Adams - The Healing Power of Sunlight Vitamin DJOSEPHNo ratings yet
- Vitamin D TGDocument25 pagesVitamin D TGKole NeljeNo ratings yet