Download as pdf or txt
You might also like
- Verbal and Non Verbal Reasoning Learning PackDocument46 pagesVerbal and Non Verbal Reasoning Learning Packmirali74100% (6)
- Please Read The Instruction Carefully!: Green FillDocument19 pagesPlease Read The Instruction Carefully!: Green FillFrida YaniNo ratings yet
- Course Syllabus SHS General Physics 1 (Stem, MELC) SY 2021-2022Document14 pagesCourse Syllabus SHS General Physics 1 (Stem, MELC) SY 2021-2022Eushane Chiya SyNo ratings yet
- Health Care Waste Assessment ToolsDocument28 pagesHealth Care Waste Assessment ToolsMohammed NabeelNo ratings yet
- Optical Math Handout RJohnson PDFDocument5 pagesOptical Math Handout RJohnson PDFRitesh Upadhyay100% (1)
- Tutorial AllplanDocument105 pagesTutorial AllplanDeac NorbertNo ratings yet
- Face-Central Incisor Form Matching in Selected South Asian PopulationDocument5 pagesFace-Central Incisor Form Matching in Selected South Asian PopulationMonwarul AzizNo ratings yet
- Comparison Between Skeletal, and Facial Measurements of Vertical Dimension in Edentulous PatientsDocument4 pagesComparison Between Skeletal, and Facial Measurements of Vertical Dimension in Edentulous Patientspaula catanaNo ratings yet
- 1 s2.0 S1748681519304012 MainDocument8 pages1 s2.0 S1748681519304012 MainegyNo ratings yet
- Perceptions of Orthodontists, Laypersons, and Patients Regarding Buccal Corridors and Facial TypesDocument11 pagesPerceptions of Orthodontists, Laypersons, and Patients Regarding Buccal Corridors and Facial TypesMohammed ijasNo ratings yet
- Journal of Cranio-Maxillo-Facial SurgeryDocument7 pagesJournal of Cranio-Maxillo-Facial SurgeryMarta FloresNo ratings yet
- 3D-CT Evaluation of Facial Asymmetry in Patients With Maxillofacial DeformitiesDocument9 pages3D-CT Evaluation of Facial Asymmetry in Patients With Maxillofacial DeformitiesR KNo ratings yet
- 2011 Effect of Extraction of First Four Premolars On Smile AestheticsDocument5 pages2011 Effect of Extraction of First Four Premolars On Smile AestheticsRabia MekamchaNo ratings yet
- Assimetria Mandibular 3DDocument8 pagesAssimetria Mandibular 3DJúnior MarotoNo ratings yet
- Journal Homepage: - : IntroductionDocument9 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- Mandibular Dental Arch Dimensions in A Sample of Iraqi Children at The Mixed Dentition StageDocument4 pagesMandibular Dental Arch Dimensions in A Sample of Iraqi Children at The Mixed Dentition StageDileep PankajNo ratings yet
- Angle Vol. 78, No. 3, 387 - 395Document9 pagesAngle Vol. 78, No. 3, 387 - 395André MéndezNo ratings yet
- The Relationship Between Dentofacial Morphology and Smile Characteristics in Lateral and Oblique ViewsDocument8 pagesThe Relationship Between Dentofacial Morphology and Smile Characteristics in Lateral and Oblique ViewsIvy MedNo ratings yet
- Am J Orthod Dentofacial Orthop. 2016 150 3 425-35Document11 pagesAm J Orthod Dentofacial Orthop. 2016 150 3 425-35jonvargasNo ratings yet
- Cephalometrics: An Overdue Evaluation: Cairo Dental Journal (24) Number (I), 11:17 January, 2008Document7 pagesCephalometrics: An Overdue Evaluation: Cairo Dental Journal (24) Number (I), 11:17 January, 2008drzana78No ratings yet
- 2007 KuenDocument7 pages2007 KuenKaro Polo KnoNo ratings yet
- Impact of Facial Bone Deformity On Nasal Shape: Plastic and Aesthetic ResearchDocument9 pagesImpact of Facial Bone Deformity On Nasal Shape: Plastic and Aesthetic ResearchJorge Andrés Fuentes ZambranoNo ratings yet
- AJODO Correa 2013Document9 pagesAJODO Correa 2013Samantha OrtizNo ratings yet
- 1 s2.0 S088954061730937X MainDocument6 pages1 s2.0 S088954061730937X MainmedicalcenterNo ratings yet
- Comparison of Different Midsagittal Plane Conf 2017 American Journal of OrthDocument10 pagesComparison of Different Midsagittal Plane Conf 2017 American Journal of Orthdruzair007No ratings yet
- Facial Flow Final PDFDocument6 pagesFacial Flow Final PDFsamir caceresNo ratings yet
- International Journal of Medical and Health ResearchDocument8 pagesInternational Journal of Medical and Health ResearchIonela MadalinaNo ratings yet
- Jopr 13204Document14 pagesJopr 13204phungNo ratings yet
- Dental JournalDocument4 pagesDental JournalanantomiNo ratings yet
- Zogheib2018 PDFDocument11 pagesZogheib2018 PDFqwertygalNo ratings yet
- Bolt On 1Document6 pagesBolt On 1Mau HernandezNo ratings yet
- Digital Smile Design For Computer Assisted Esthetic RehabilitationDocument10 pagesDigital Smile Design For Computer Assisted Esthetic RehabilitationRoberto PucNo ratings yet
- Digital Smile Design - Predictable Results (#741934) - 1117267Document6 pagesDigital Smile Design - Predictable Results (#741934) - 1117267yuumiNo ratings yet
- Jced 5 E231Document8 pagesJced 5 E231ruben dario meza bertelNo ratings yet
- Art 2 PDFDocument8 pagesArt 2 PDFMilena RamirezNo ratings yet
- Reliability of Clinical Crown Center To Predict Marginal Ridge LevelingDocument7 pagesReliability of Clinical Crown Center To Predict Marginal Ridge LevelingSérgio EstelitaNo ratings yet
- Eur J Orthod 2009 Wellens 503 15Document13 pagesEur J Orthod 2009 Wellens 503 15Serene BatraNo ratings yet
- The Denture Frame Analysis: An Additional Diagnostic ToolDocument9 pagesThe Denture Frame Analysis: An Additional Diagnostic ToolMirek SzNo ratings yet
- Arch FormDocument14 pagesArch FormRiad IskanderNo ratings yet
- Perception of The Esthetic Impact of Gingival Smile On Laypersons, Dental Professionals, and Dental StudentsDocument7 pagesPerception of The Esthetic Impact of Gingival Smile On Laypersons, Dental Professionals, and Dental StudentsCésar Mauricio VilchezNo ratings yet
- 13 de Praeter J, Dermaut L, Martens G, Et Al - Long-Term Stability of The Leveling of The Curve of SpeeDocument7 pages13 de Praeter J, Dermaut L, Martens G, Et Al - Long-Term Stability of The Leveling of The Curve of SpeeabhishekiNo ratings yet
- Two-Year Follow-Up of Multidisciplinary Treatment Using DigitalDocument5 pagesTwo-Year Follow-Up of Multidisciplinary Treatment Using DigitalADRIANNo ratings yet
- Comparison Between 2D Cephalometric and 3D Digital Model Superimpositions in Patients With Lateral Incisor Agenesis Treated by Canine SubstitutionDocument10 pagesComparison Between 2D Cephalometric and 3D Digital Model Superimpositions in Patients With Lateral Incisor Agenesis Treated by Canine Substitutionhasan.abomohamedNo ratings yet
- Henrikson J, Persson M, Thilander B. Long-Term Stability ofDocument12 pagesHenrikson J, Persson M, Thilander B. Long-Term Stability ofyerly ramirezNo ratings yet
- Comparison of Overjet Among 3 Arch Types in Normal OcclusionDocument8 pagesComparison of Overjet Among 3 Arch Types in Normal OcclusionAlexandra308No ratings yet
- Ort Stom PDFDocument100 pagesOrt Stom PDFaliolveroNo ratings yet
- Beta Angle in IraqiDocument6 pagesBeta Angle in Iraqisurendra334No ratings yet
- Cevidanes 2009 (Sobreposição Tomo)Document6 pagesCevidanes 2009 (Sobreposição Tomo)Tadeu MendesNo ratings yet
- Evaluation of The Golden Proportion in Facial Soft-Tissues of Class I and II Malocclusion PatientsDocument6 pagesEvaluation of The Golden Proportion in Facial Soft-Tissues of Class I and II Malocclusion PatientsIkhwan Zulmi DalimuntheNo ratings yet
- Do Different Vertical Positions of Maxillary Central Incisors Influence Smile Esthetics Perception?Document11 pagesDo Different Vertical Positions of Maxillary Central Incisors Influence Smile Esthetics Perception?cruvbkj hchjkNo ratings yet
- Nikolaidis Pitas - Facial Feature Extraction and Pose DeterminationDocument20 pagesNikolaidis Pitas - Facial Feature Extraction and Pose DeterminationVienNgocQuangNo ratings yet
- Correlation Between Maxillary Central Incisor Crown Morphology and Mandibular Dental Arch Form in Normal Occlusion SubjectsDocument5 pagesCorrelation Between Maxillary Central Incisor Crown Morphology and Mandibular Dental Arch Form in Normal Occlusion SubjectsJessi RecaldeNo ratings yet
- J Jcms 2015 12 012Document41 pagesJ Jcms 2015 12 012Gerardo Valenzuela GonzálezNo ratings yet
- Yang. AJODO 2015. Effect of Mesiodistal Angulation of The Maxillary Central Incisors On Esthetic Perceptions of The Smile Frontal ViewDocument9 pagesYang. AJODO 2015. Effect of Mesiodistal Angulation of The Maxillary Central Incisors On Esthetic Perceptions of The Smile Frontal Viewjustin4leNo ratings yet
- 2009 - Schabel - Subjective Vs Objective Evaluations of Smile EstheticsDocument8 pages2009 - Schabel - Subjective Vs Objective Evaluations of Smile EstheticsVictóriaEscóssiaNo ratings yet
- Tomography 10 00004Document10 pagesTomography 10 00004lekshmip9715No ratings yet
- Artigo Inglês 4Document4 pagesArtigo Inglês 4Ana LuizaNo ratings yet
- Ijd2020 8855681Document6 pagesIjd2020 8855681Jessi RecaldeNo ratings yet
- Method of Assessing Facial Change Induced by Orthodontic TreatmentDocument17 pagesMethod of Assessing Facial Change Induced by Orthodontic TreatmentKaruna ShresthaNo ratings yet
- Articulo 2 - Clase IIDocument10 pagesArticulo 2 - Clase IIMarcela Cano RicardoNo ratings yet
- Dynamic Smile Analysis in Young AdultsDocument9 pagesDynamic Smile Analysis in Young AdultsameodontoNo ratings yet
- Online Only Abstracts - YmodDocument5 pagesOnline Only Abstracts - YmodDr.Prakher SainiNo ratings yet
- Evaluation of Facial Hard and Soft Tissueusing CBCTDocument13 pagesEvaluation of Facial Hard and Soft Tissueusing CBCTSoe San KyawNo ratings yet
- Smile Analysis PDFDocument4 pagesSmile Analysis PDFtikaNo ratings yet
- The Prayer of A Traveler: Shaykh Salih Al-FawzanDocument4 pagesThe Prayer of A Traveler: Shaykh Salih Al-FawzanMohammed NabeelNo ratings yet
- Smu Mba Healthcare Management Project With Guideline Free Sample Download - Project HelplineDocument68 pagesSmu Mba Healthcare Management Project With Guideline Free Sample Download - Project HelplineMohammed Nabeel0% (1)
- MCQ in ProsthodonticsDocument5 pagesMCQ in ProsthodonticsMohammed NabeelNo ratings yet
- Developmental Disorders of Oral Cavity PDFDocument121 pagesDevelopmental Disorders of Oral Cavity PDFMohammed Nabeel100% (1)
- Gingival Crevice FluidDocument3 pagesGingival Crevice FluidMohammed NabeelNo ratings yet
- Glycobiology 2014 Etulain 1252 9Document8 pagesGlycobiology 2014 Etulain 1252 9Mohammed NabeelNo ratings yet
- Occlusal SplintDocument4 pagesOcclusal SplintMohammed NabeelNo ratings yet
- Principles of Occlusion in Complete DentureDocument72 pagesPrinciples of Occlusion in Complete DentureMohammed NabeelNo ratings yet
- Finance in A Nutshell Javier Estrada FT Prentice Hall, 2005: Answer Key To Challenge SectionsDocument63 pagesFinance in A Nutshell Javier Estrada FT Prentice Hall, 2005: Answer Key To Challenge Sectionssanucwa6932No ratings yet
- Delays VerilogDocument18 pagesDelays VerilogAkhilesh SinghNo ratings yet
- Ass 1Document4 pagesAss 1Shashwat AgrawalNo ratings yet
- Shear Force and Bending Moment DiagramDocument11 pagesShear Force and Bending Moment DiagramfreonxzNo ratings yet
- LA7837Document9 pagesLA7837Julio Hernandez MateoNo ratings yet
- E7 2014-2-Pen-Jit Sin-ADocument4 pagesE7 2014-2-Pen-Jit Sin-APeng Peng KekNo ratings yet
- Prediction of Wall Thickness Distribution in Simple Thermoforming MouldDocument8 pagesPrediction of Wall Thickness Distribution in Simple Thermoforming MouldFrancisco Ribeiro FernandesNo ratings yet
- Abaqus TutorialDocument11 pagesAbaqus TutorialXaockaNo ratings yet
- Laplace Table PDFDocument2 pagesLaplace Table PDFDeve UsterNo ratings yet
- Melegin Angoluan-Correlaing VariablesDocument6 pagesMelegin Angoluan-Correlaing VariablesMelegin RatonNo ratings yet
- Science Notebook Analyzing Data Scientific Notation and Dimensional Analysis Student EditableDocument4 pagesScience Notebook Analyzing Data Scientific Notation and Dimensional Analysis Student EditableMaisam Al AaliNo ratings yet
- Portion&Blueprint-class (Xi & Xii)Document13 pagesPortion&Blueprint-class (Xi & Xii)THANIGAINATHAN.G.D 10A3No ratings yet
- Teorema de SteinerDocument4 pagesTeorema de Steinerluis quitianNo ratings yet
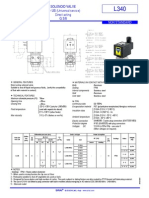
- Electrovalva Sirai L340v08GDocument2 pagesElectrovalva Sirai L340v08Ggig90No ratings yet
- Some Generalized Order-Disorder TransformationsDocument4 pagesSome Generalized Order-Disorder TransformationsBoris Atenas NuñezNo ratings yet
- Summative Test in Gen Math 1Document9 pagesSummative Test in Gen Math 1Park NimfaNo ratings yet
- Prime & Composite NumbersDocument39 pagesPrime & Composite NumbersShane TeruelNo ratings yet
- Mass Transfer: Assoc. Prof. Dr. Emel AKYOLDocument18 pagesMass Transfer: Assoc. Prof. Dr. Emel AKYOLesra göçen100% (1)
- Local Grid RefinementDocument10 pagesLocal Grid RefinementWallace StationNo ratings yet
- EEE 353 - Lecture-1Document30 pagesEEE 353 - Lecture-1rontojoyNo ratings yet
- 1 SMDocument11 pages1 SMNuPhia MagdalenaNo ratings yet
- 11aDocument44 pages11agegegegNo ratings yet
- Assembly Language TestDocument3 pagesAssembly Language TestLeo100% (2)
- BS - Reinforced Masonry Design GuideDocument76 pagesBS - Reinforced Masonry Design Guidescgengineer100% (7)
- Chapter 5 Analysing Investment Risk and Its ApplicationDocument14 pagesChapter 5 Analysing Investment Risk and Its ApplicationMaisarah YaziddNo ratings yet