
Ni Hms 422918
Ni Hms 422918
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5825)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Way With Words Offline Assessment - Audio - Mixed - AccentsDocument2 pagesWay With Words Offline Assessment - Audio - Mixed - AccentsCeline InterinoNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Final ThesisDocument74 pagesFinal ThesisPeter Castillo79% (34)
- Stihl Ts500i Service Manual-StihlDocument118 pagesStihl Ts500i Service Manual-StihlCarl Carlson63% (8)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Engineering Mechanics NotesDocument100 pagesEngineering Mechanics NotesRagothsingh Ramadoss67% (3)
- Prayer Guide - Five Fold Ministry - 4Document12 pagesPrayer Guide - Five Fold Ministry - 4Joseph100% (1)
- FK 84 - 2015Document1 pageFK 84 - 2015Vishnu R PuthusseryNo ratings yet
- Simple Interest: 7 Important Shortcuts ExplainedDocument3 pagesSimple Interest: 7 Important Shortcuts ExplainedVishnu R PuthusseryNo ratings yet
- FK 16-15Document1 pageFK 16-15Vishnu R PuthusseryNo ratings yet
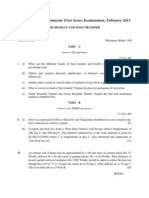
- s6 HMT Series 1 - 2013-FinalDocument2 pagess6 HMT Series 1 - 2013-FinalVishnu R PuthusseryNo ratings yet
- MTech Draft RegulationsDocument13 pagesMTech Draft RegulationsVishnu R PuthusseryNo ratings yet
- Civil Service NomineeDocument2 pagesCivil Service NomineeVishnu R PuthusseryNo ratings yet
- Mini Project PresentationDocument23 pagesMini Project PresentationVishnu R PuthusseryNo ratings yet
- Application Form (To Be Fully Typed in Capital Letters)Document2 pagesApplication Form (To Be Fully Typed in Capital Letters)Vishnu R PuthusseryNo ratings yet
- Thermal ModellingDocument28 pagesThermal ModellingVishnu R PuthusseryNo ratings yet
- Industrial Training Report 2011: at Mechanical Engineering Department HLL Lifecare Limited TrivandrumDocument3 pagesIndustrial Training Report 2011: at Mechanical Engineering Department HLL Lifecare Limited TrivandrumVishnu R PuthusseryNo ratings yet
- Drawing Basics - The Cube - The Drawing Blog - Artist DailyDocument4 pagesDrawing Basics - The Cube - The Drawing Blog - Artist DailyVishnu R PuthusseryNo ratings yet
- UAMDocument35 pagesUAMVishnu R PuthusseryNo ratings yet
- Paragraphs: A. B. C. D. E. FDocument4 pagesParagraphs: A. B. C. D. E. FAnh Cường ĐỗNo ratings yet
- Correlation DesignDocument43 pagesCorrelation DesignPuru TiwariNo ratings yet
- Ncert Solutions For Class 9 March 28 Science Chapter 5 The Fundamental Unit of LifeDocument8 pagesNcert Solutions For Class 9 March 28 Science Chapter 5 The Fundamental Unit of LifeEshaan BansalNo ratings yet
- Theoretical Foundations of Classroom Management in Special Education Module 2Document27 pagesTheoretical Foundations of Classroom Management in Special Education Module 2XERXA BILLONES100% (1)
- Reaction Paper KyleDocument4 pagesReaction Paper KyleRonaliza Durano SanchezNo ratings yet
- Bio Project Drug Resistance in BacteriaDocument18 pagesBio Project Drug Resistance in BacteriaAKASH ALAMNo ratings yet
- Creative Restaurant MenuDocument51 pagesCreative Restaurant MenuVicko PratamaNo ratings yet
- Definition Goals and Scope of Special and Inclusive EducationDocument8 pagesDefinition Goals and Scope of Special and Inclusive EducationBrenda Bravo100% (3)
- Earnings Statementimportant - Keep For Your Records: E-MailDocument1 pageEarnings Statementimportant - Keep For Your Records: E-MailJuanNo ratings yet
- Module 3 G10 (Q4)Document4 pagesModule 3 G10 (Q4)Meco ChicaNo ratings yet
- TACA Times Sept/Oct 2010Document6 pagesTACA Times Sept/Oct 2010Bruce WileyNo ratings yet
- MCN Nclex #1Document10 pagesMCN Nclex #1Bethlnly Nasayao100% (1)
- Raman, 1998Document10 pagesRaman, 1998Luan CaetanoNo ratings yet
- PowerDocument10 pagesPowerThomas Kristianto Edhi WangkoroNo ratings yet
- I ™Document25 pagesI ™SAB78No ratings yet
- At Home Training Guide: Workout BuilderDocument22 pagesAt Home Training Guide: Workout BuilderAnonymous NO0urGNo ratings yet
- Work Program For RoadsDocument8 pagesWork Program For RoadsSupun KariyawasamNo ratings yet
- Report of One Day Inservice Education - Mamata DasDocument16 pagesReport of One Day Inservice Education - Mamata DasJay Paul100% (1)
- Parksmart One PagerDocument2 pagesParksmart One PagerAnubhav MishraNo ratings yet
- Grade 7 8.1 Bacteria Fungi and ProtistsDocument14 pagesGrade 7 8.1 Bacteria Fungi and ProtistsRafunzel Pe BandoquilloNo ratings yet
- Lesson Plan in Top of Stove Cooking Equipment and Baking EquipmentDocument16 pagesLesson Plan in Top of Stove Cooking Equipment and Baking EquipmentNiña Mae SabilloNo ratings yet
- Summary of DissertationDocument8 pagesSummary of Dissertationjean uwakijijweNo ratings yet
- ASSERTIONDocument43 pagesASSERTIONAprilene YanuariaNo ratings yet
- Glucose Health - New Herbs RangeDocument42 pagesGlucose Health - New Herbs RangeTapan ChowdhuryNo ratings yet
- General: Technical Data TAD1641GEDocument9 pagesGeneral: Technical Data TAD1641GEBill CastilloNo ratings yet
- Guidelines For Hard MaterialDocument30 pagesGuidelines For Hard MaterialMuhamad MuzakkirNo ratings yet
















































































Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5825)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Way With Words Offline Assessment - Audio - Mixed - AccentsDocument2 pagesWay With Words Offline Assessment - Audio - Mixed - AccentsCeline InterinoNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Final ThesisDocument74 pagesFinal ThesisPeter Castillo79% (34)
- Stihl Ts500i Service Manual-StihlDocument118 pagesStihl Ts500i Service Manual-StihlCarl Carlson63% (8)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Engineering Mechanics NotesDocument100 pagesEngineering Mechanics NotesRagothsingh Ramadoss67% (3)
- Prayer Guide - Five Fold Ministry - 4Document12 pagesPrayer Guide - Five Fold Ministry - 4Joseph100% (1)
- FK 84 - 2015Document1 pageFK 84 - 2015Vishnu R PuthusseryNo ratings yet
- Simple Interest: 7 Important Shortcuts ExplainedDocument3 pagesSimple Interest: 7 Important Shortcuts ExplainedVishnu R PuthusseryNo ratings yet
- FK 16-15Document1 pageFK 16-15Vishnu R PuthusseryNo ratings yet
- s6 HMT Series 1 - 2013-FinalDocument2 pagess6 HMT Series 1 - 2013-FinalVishnu R PuthusseryNo ratings yet
- MTech Draft RegulationsDocument13 pagesMTech Draft RegulationsVishnu R PuthusseryNo ratings yet
- Civil Service NomineeDocument2 pagesCivil Service NomineeVishnu R PuthusseryNo ratings yet
- Mini Project PresentationDocument23 pagesMini Project PresentationVishnu R PuthusseryNo ratings yet
- Application Form (To Be Fully Typed in Capital Letters)Document2 pagesApplication Form (To Be Fully Typed in Capital Letters)Vishnu R PuthusseryNo ratings yet
- Thermal ModellingDocument28 pagesThermal ModellingVishnu R PuthusseryNo ratings yet
- Industrial Training Report 2011: at Mechanical Engineering Department HLL Lifecare Limited TrivandrumDocument3 pagesIndustrial Training Report 2011: at Mechanical Engineering Department HLL Lifecare Limited TrivandrumVishnu R PuthusseryNo ratings yet
- Drawing Basics - The Cube - The Drawing Blog - Artist DailyDocument4 pagesDrawing Basics - The Cube - The Drawing Blog - Artist DailyVishnu R PuthusseryNo ratings yet
- UAMDocument35 pagesUAMVishnu R PuthusseryNo ratings yet
- Paragraphs: A. B. C. D. E. FDocument4 pagesParagraphs: A. B. C. D. E. FAnh Cường ĐỗNo ratings yet
- Correlation DesignDocument43 pagesCorrelation DesignPuru TiwariNo ratings yet
- Ncert Solutions For Class 9 March 28 Science Chapter 5 The Fundamental Unit of LifeDocument8 pagesNcert Solutions For Class 9 March 28 Science Chapter 5 The Fundamental Unit of LifeEshaan BansalNo ratings yet
- Theoretical Foundations of Classroom Management in Special Education Module 2Document27 pagesTheoretical Foundations of Classroom Management in Special Education Module 2XERXA BILLONES100% (1)
- Reaction Paper KyleDocument4 pagesReaction Paper KyleRonaliza Durano SanchezNo ratings yet
- Bio Project Drug Resistance in BacteriaDocument18 pagesBio Project Drug Resistance in BacteriaAKASH ALAMNo ratings yet
- Creative Restaurant MenuDocument51 pagesCreative Restaurant MenuVicko PratamaNo ratings yet
- Definition Goals and Scope of Special and Inclusive EducationDocument8 pagesDefinition Goals and Scope of Special and Inclusive EducationBrenda Bravo100% (3)
- Earnings Statementimportant - Keep For Your Records: E-MailDocument1 pageEarnings Statementimportant - Keep For Your Records: E-MailJuanNo ratings yet
- Module 3 G10 (Q4)Document4 pagesModule 3 G10 (Q4)Meco ChicaNo ratings yet
- TACA Times Sept/Oct 2010Document6 pagesTACA Times Sept/Oct 2010Bruce WileyNo ratings yet
- MCN Nclex #1Document10 pagesMCN Nclex #1Bethlnly Nasayao100% (1)
- Raman, 1998Document10 pagesRaman, 1998Luan CaetanoNo ratings yet
- PowerDocument10 pagesPowerThomas Kristianto Edhi WangkoroNo ratings yet
- I ™Document25 pagesI ™SAB78No ratings yet
- At Home Training Guide: Workout BuilderDocument22 pagesAt Home Training Guide: Workout BuilderAnonymous NO0urGNo ratings yet
- Work Program For RoadsDocument8 pagesWork Program For RoadsSupun KariyawasamNo ratings yet
- Report of One Day Inservice Education - Mamata DasDocument16 pagesReport of One Day Inservice Education - Mamata DasJay Paul100% (1)
- Parksmart One PagerDocument2 pagesParksmart One PagerAnubhav MishraNo ratings yet
- Grade 7 8.1 Bacteria Fungi and ProtistsDocument14 pagesGrade 7 8.1 Bacteria Fungi and ProtistsRafunzel Pe BandoquilloNo ratings yet
- Lesson Plan in Top of Stove Cooking Equipment and Baking EquipmentDocument16 pagesLesson Plan in Top of Stove Cooking Equipment and Baking EquipmentNiña Mae SabilloNo ratings yet
- Summary of DissertationDocument8 pagesSummary of Dissertationjean uwakijijweNo ratings yet
- ASSERTIONDocument43 pagesASSERTIONAprilene YanuariaNo ratings yet
- Glucose Health - New Herbs RangeDocument42 pagesGlucose Health - New Herbs RangeTapan ChowdhuryNo ratings yet
- General: Technical Data TAD1641GEDocument9 pagesGeneral: Technical Data TAD1641GEBill CastilloNo ratings yet
- Guidelines For Hard MaterialDocument30 pagesGuidelines For Hard MaterialMuhamad MuzakkirNo ratings yet