Download as pdf or txt
You might also like
- Small Animal Spinal Disorders Diagnosis and Surgery, 2nd Edition (Vetbooks - Ir)Document369 pagesSmall Animal Spinal Disorders Diagnosis and Surgery, 2nd Edition (Vetbooks - Ir)ghimboasaNo ratings yet
- Pediatric Surgery HandbookDocument75 pagesPediatric Surgery HandbookAlex Vătau100% (2)
- Principles of Patient PositioningDocument62 pagesPrinciples of Patient PositioningMelody JusticeNo ratings yet
- SotaiDocument11 pagesSotailavagancia0% (2)
- Pneumologie PDFDocument1,155 pagesPneumologie PDFMariana Dragoi100% (1)
- The FACIAL NERVE Current Trends in Diagnosis, Treatment, and RehabilitationDocument17 pagesThe FACIAL NERVE Current Trends in Diagnosis, Treatment, and RehabilitationkrazeedoctorNo ratings yet
- Clinical Reasoning: Rare Cause of Hemiparesis and Ataxia in A 36-Year-Old ManDocument8 pagesClinical Reasoning: Rare Cause of Hemiparesis and Ataxia in A 36-Year-Old MansamuelNo ratings yet
- Exercise-Associated Numbness and Tingling in The Legs: For Editorial Comment See Page 1509Document4 pagesExercise-Associated Numbness and Tingling in The Legs: For Editorial Comment See Page 1509herpthederpNo ratings yet
- Intrasphenoidal Encephalocele: An Incidental Finding in Emergency DepartmentDocument3 pagesIntrasphenoidal Encephalocele: An Incidental Finding in Emergency DepartmentRinda AndreanditaNo ratings yet
- Facial PalsyDocument12 pagesFacial PalsyIqbal HabibieNo ratings yet
- A 7-Year-Old Boy Dying of Acute Encephalopathy: Case History Autopsy FindingsDocument4 pagesA 7-Year-Old Boy Dying of Acute Encephalopathy: Case History Autopsy FindingswillygopeNo ratings yet
- Mab200501 10Document8 pagesMab200501 10Muhammad Ardyansyah PratamaNo ratings yet
- D Evaluation For Resective Epilepsy SurgeryDocument104 pagesD Evaluation For Resective Epilepsy SurgeryYusuf BrilliantNo ratings yet
- Neurology Clinical Cases PDFDocument219 pagesNeurology Clinical Cases PDFHandre PutraNo ratings yet
- Vocal Cord Palsy: An Uncommon Presenting Feature of Myasthenia GravisDocument4 pagesVocal Cord Palsy: An Uncommon Presenting Feature of Myasthenia GravisDivine Jane PurciaNo ratings yet
- J Yebeh 2019 106551Document6 pagesJ Yebeh 2019 106551Luisa Fernanda Lopez MoraNo ratings yet
- Facial Nerve Palsy: Dr. Saud AlromaihDocument74 pagesFacial Nerve Palsy: Dr. Saud AlromaihChandra ManapaNo ratings yet
- Bilateral Facial Nerve (Bell's) Palsy in A 24-Year-Old Woman: A Case ReportDocument3 pagesBilateral Facial Nerve (Bell's) Palsy in A 24-Year-Old Woman: A Case Reportokto namikaNo ratings yet
- Bilateral Facial Nerve (Bells) Palsy in A 24-Year-Old WomanDocument3 pagesBilateral Facial Nerve (Bells) Palsy in A 24-Year-Old WomanmimicamasoNo ratings yet
- Acu Accident LumbarDocument2 pagesAcu Accident Lumbarrswongym449No ratings yet
- Liu 2016Document2 pagesLiu 2016Anonymous l3X3jf0NPNo ratings yet
- TJN 44370 Images in Clinical Neurology Aggarwal (A)Document3 pagesTJN 44370 Images in Clinical Neurology Aggarwal (A)VisshwajeetNo ratings yet
- Adem LikeDocument4 pagesAdem LikeRodrigo AriasNo ratings yet
- Case Report: Vertigo As A Predominant Manifestation of NeurosarcoidosisDocument5 pagesCase Report: Vertigo As A Predominant Manifestation of NeurosarcoidosisDjumadi AkbarNo ratings yet
- Facial Nerve Disroders and OtalgiaDocument39 pagesFacial Nerve Disroders and Otalgiaياسر كوثر هانيNo ratings yet
- Epilepsy & Behavior Case Reports: 10.1016/j.ebcr.2017.07.003Document21 pagesEpilepsy & Behavior Case Reports: 10.1016/j.ebcr.2017.07.003Faras ArinalNo ratings yet
- Bell's Palsy With Ipsilateral Numbness: Short ReportDocument3 pagesBell's Palsy With Ipsilateral Numbness: Short ReportubayyumrNo ratings yet
- Part 1 CNS CasesDocument10 pagesPart 1 CNS CasesMicole NatividadNo ratings yet
- A Case Report of Hydrocephalus in A US Military RecruitDocument3 pagesA Case Report of Hydrocephalus in A US Military RecruitRomita PutriNo ratings yet
- Fah Ling 2016Document2 pagesFah Ling 2016Anonymous OjlR4HLNo ratings yet
- Als LymeDocument2 pagesAls LymeChristine Anne HellmundNo ratings yet
- Case Report: A Rare Case of Central Nervous System TuberculosisDocument6 pagesCase Report: A Rare Case of Central Nervous System TuberculosislittlecandiesNo ratings yet
- Casereport: Vishal Jain, MD, Anagha Deshmukh, MD, Stephen Gollomp, MDDocument4 pagesCasereport: Vishal Jain, MD, Anagha Deshmukh, MD, Stephen Gollomp, MDlionkingNo ratings yet
- Neurohistiocytosis: Two Cases of A Rare DiseaseDocument8 pagesNeurohistiocytosis: Two Cases of A Rare DiseaseIJAR JOURNALNo ratings yet
- Cerebellar Hemangioblastoma-A Rare EntityDocument10 pagesCerebellar Hemangioblastoma-A Rare EntityJay LeheriNo ratings yet
- Intracranial Cavernomatous Hemangiomas As A Cause of Childhood Temporal Lobe EpilepsyDocument2 pagesIntracranial Cavernomatous Hemangiomas As A Cause of Childhood Temporal Lobe EpilepsyPrateek Kumar PandaNo ratings yet
- Aca Infarction With Mers Due To Infective Arteritis of An Interhemispheric Subdural Empyema Complicating A Maxillary SinusitisDocument3 pagesAca Infarction With Mers Due To Infective Arteritis of An Interhemispheric Subdural Empyema Complicating A Maxillary SinusitisIJAR JOURNALNo ratings yet
- Acute Blindness in A Dog With Acinetobacter-Associated Postencephalitic HydrocephalusDocument5 pagesAcute Blindness in A Dog With Acinetobacter-Associated Postencephalitic Hydrocephaluslikxel1027No ratings yet
- Canine Choroid Plexus Tumor With Intracranial Dissemination Presenting As Multiple Cystic LesionsDocument5 pagesCanine Choroid Plexus Tumor With Intracranial Dissemination Presenting As Multiple Cystic LesionsMihai SavescuNo ratings yet
- Ramsay HuntDocument3 pagesRamsay HuntFebri AntoNo ratings yet
- Clinical Reasoning: A Young Man With Recurrent Paralysis, Revisable White Matter Lesions and Peripheral Neuropathy Word Count: 945Document13 pagesClinical Reasoning: A Young Man With Recurrent Paralysis, Revisable White Matter Lesions and Peripheral Neuropathy Word Count: 945aileenzhongNo ratings yet
- S.Sharma, Et Al - 2Document4 pagesS.Sharma, Et Al - 2Anonymous QPXAgjBwNo ratings yet
- 22 October 19 Fcps 2Document36 pages22 October 19 Fcps 2Kahkashan HameedNo ratings yet
- TTH Journal 4 PDFDocument5 pagesTTH Journal 4 PDFRumah Kost Kontrakan AntapaniNo ratings yet
- Motor Cortex Stimulation For Neuropathic Facial Pain: Nikolai G. Rainov and Volkmar HeideckeDocument5 pagesMotor Cortex Stimulation For Neuropathic Facial Pain: Nikolai G. Rainov and Volkmar HeideckemoiNo ratings yet
- EN + EosinofiliaDocument3 pagesEN + EosinofiliaAna Flavia BaptistaNo ratings yet
- Bell's Palsy: Pathogenesis, Clinical Features, and Diagnosis in AdultsDocument16 pagesBell's Palsy: Pathogenesis, Clinical Features, and Diagnosis in AdultsAmada Angel VillanuevaNo ratings yet
- Neuro JournalDocument7 pagesNeuro JournalLannydchandraNo ratings yet
- Jurnal Reading Saraf ALGIDocument6 pagesJurnal Reading Saraf ALGIMuhammad Al GifariNo ratings yet
- AbcesoDocument2 pagesAbcesoRocio LedesmaNo ratings yet
- Ruptured Cerebral Aneurysms: PerspectiveDocument4 pagesRuptured Cerebral Aneurysms: PerspectiveDini Nanami100% (1)
- Neuroscience AssignmentDocument7 pagesNeuroscience AssignmentAubrey Unique EvangelistaNo ratings yet
- Constellatus StrokeDocument4 pagesConstellatus StrokeW Antonio Rivera MartínezNo ratings yet
- Neuroanatomical Considerations of Isolated Hearing Loss in Thalamic HemorrhageDocument3 pagesNeuroanatomical Considerations of Isolated Hearing Loss in Thalamic HemorrhageBella Cynthia BettabestariNo ratings yet
- 6M Case Report Postinfectious CerebellitisDocument14 pages6M Case Report Postinfectious CerebellitisGa B B OrlonganNo ratings yet
- Case Report: Coexistence of Ankylosing Spondylitis and Neurofibromatosis Type 1Document4 pagesCase Report: Coexistence of Ankylosing Spondylitis and Neurofibromatosis Type 1Lupita Mora LobacoNo ratings yet
- 278 977 1 SMDocument2 pages278 977 1 SMMohamed MukhrizNo ratings yet
- Steroid Pulse Therapy in Herpes Simplex Encephalitis: Neurosciences July 2013Document3 pagesSteroid Pulse Therapy in Herpes Simplex Encephalitis: Neurosciences July 2013Dwi KurniawanNo ratings yet
- Idiopathic Intracranial Hypertension (By Dr. Rakshay)Document51 pagesIdiopathic Intracranial Hypertension (By Dr. Rakshay)Rakshay KaulNo ratings yet
- Pineal TumorsDocument8 pagesPineal TumorsNguyen Tran CanhNo ratings yet
- Management of Bell's Palsy and Ramsay Hunt Syndrome - ClinicalKeyDocument33 pagesManagement of Bell's Palsy and Ramsay Hunt Syndrome - ClinicalKeyWaterfloNo ratings yet
- Clinical Neuroimmunology: Multiple Sclerosis and Related DisordersFrom EverandClinical Neuroimmunology: Multiple Sclerosis and Related DisordersNo ratings yet
- Neurovascular NeuropsychologyFrom EverandNeurovascular NeuropsychologyRonald M. LazarNo ratings yet
- Patient or Problem Intervention Comparison OutcomeDocument2 pagesPatient or Problem Intervention Comparison OutcomeafiwahyuNo ratings yet
- Emergencies in UrologyDocument112 pagesEmergencies in UrologyafiwahyuNo ratings yet
- Neurotransmitters & NeuromodulatorsDocument41 pagesNeurotransmitters & Neuromodulatorsafiwahyu100% (1)
- Alasan Ke ManusiaDocument12 pagesAlasan Ke ManusiaafiwahyuNo ratings yet
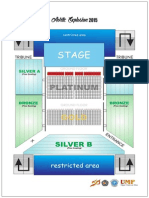
- Site PlanDocument1 pageSite PlanafiwahyuNo ratings yet
- Dental ImplantDocument36 pagesDental ImplantLeony Ricci100% (5)
- 11 01 06 Bambach BrochureDocument6 pages11 01 06 Bambach BrochureFred StoreyNo ratings yet
- Meridian /channel: Simplified Chinese Traditional Chinese PinyinDocument20 pagesMeridian /channel: Simplified Chinese Traditional Chinese Pinyinramesh2007-mptNo ratings yet
- NM Injection TherapyDocument2 pagesNM Injection TherapypranajiNo ratings yet
- Comet SCD 1 PDFDocument2 pagesComet SCD 1 PDFWilliamNo ratings yet
- Basic Suturing and Wound Management PrintableDocument14 pagesBasic Suturing and Wound Management Printablepakya hussinNo ratings yet
- Final Report On PediatricDocument17 pagesFinal Report On PediatricJoshua MillzNo ratings yet
- INSULINDocument6 pagesINSULINmilaNo ratings yet
- Jurnal Internasional Post Laparatomi 2014 PDFDocument8 pagesJurnal Internasional Post Laparatomi 2014 PDFDimas PramudyaNo ratings yet
- Ventricular Septal DefectDocument55 pagesVentricular Septal DefecthoneyworksNo ratings yet
- Coldex CapsuleDocument3 pagesColdex Capsulehk_scribdNo ratings yet
- 5.11 NC AG Letter To MissionDocument3 pages5.11 NC AG Letter To MissionMitchell BlackNo ratings yet
- Amblyopia Hunter PDFDocument12 pagesAmblyopia Hunter PDFWaqar AhmadNo ratings yet
- Continuous Positive Airway Pressure (CPAP)Document53 pagesContinuous Positive Airway Pressure (CPAP)indiamahesh100% (1)
- Neurofibromatosis Type 1Document9 pagesNeurofibromatosis Type 1Mitra SadrameliNo ratings yet
- AntacidsDocument16 pagesAntacidsVishal CoolestNo ratings yet
- A Study of The Incidence of Over Eruption and Occlusal Interferences in Unopposed Posterior TeethDocument8 pagesA Study of The Incidence of Over Eruption and Occlusal Interferences in Unopposed Posterior TeethimwinnerNo ratings yet
- Maria Encarnacion RESUMEDocument2 pagesMaria Encarnacion RESUMEarlyn encarnacionNo ratings yet
- Picot PaperDocument10 pagesPicot PaperFatoumata BayoNo ratings yet
- ChemotherapyDocument16 pagesChemotherapyCandida NickensNo ratings yet
- Drain CareDocument6 pagesDrain Carecharleston_mendozaNo ratings yet
- ACEMAC 2019 BrochureDocument5 pagesACEMAC 2019 BrochureAshley PrescottNo ratings yet
- Pusponegoro HD. Standar Pelayanan Medis Kesehatan Anak Edisi 1. Jakarta: Badan Penerbit IDAI, 2004. Hal 149-153Document2 pagesPusponegoro HD. Standar Pelayanan Medis Kesehatan Anak Edisi 1. Jakarta: Badan Penerbit IDAI, 2004. Hal 149-153Nurrahmadani RambeNo ratings yet
- Raphael Sevilla, PT, DPT: Student Physical TherapistDocument1 pageRaphael Sevilla, PT, DPT: Student Physical TherapistRaphael SevillaNo ratings yet
- Haitian English BookDocument85 pagesHaitian English BookjeanclaudiNo ratings yet
- Natural Vision Improvement - Short Exercises and RecommendationsDocument3 pagesNatural Vision Improvement - Short Exercises and RecommendationsElizabeta RadeskaNo ratings yet