Download as pdf or txt
You might also like
- Test Banks For Contemporary Clinical Immunology and SerologyDocument1 pageTest Banks For Contemporary Clinical Immunology and Serologyhamadadodo7No ratings yet
- Test Banks For Basic and Applied Concepts of Blood Banking and Transfusion PracticesDocument1 pageTest Banks For Basic and Applied Concepts of Blood Banking and Transfusion Practiceshamadadodo7No ratings yet
- Chapter 04 Test Bank: Carbohydrates: Fill in The Blank QuestionsDocument24 pagesChapter 04 Test Bank: Carbohydrates: Fill in The Blank Questionscynthiaaa s100% (1)
- DiabetesmellitusDocument24 pagesDiabetesmellitusSania SaeedNo ratings yet
- Glucose Indices 2022Document40 pagesGlucose Indices 2022mustafa.abdo23112001No ratings yet
- Diabetes MellitusDocument85 pagesDiabetes MellitusPriyanka Hr GowdaNo ratings yet
- Diabetes MellitusDocument38 pagesDiabetes MellitustantsaNo ratings yet
- Diabetes - Oral KnowledgeDocument19 pagesDiabetes - Oral KnowledgeKSeegurNo ratings yet
- Blood GlucoseDocument42 pagesBlood GlucoseShaira De La CruzNo ratings yet
- Diabetes MellitusDocument17 pagesDiabetes MellitusKeeping up with ania kokoNo ratings yet
- Diabetes Mellitus in PregnancyDocument53 pagesDiabetes Mellitus in PregnancydemiseadmassuNo ratings yet
- Diabetes Mellitus Final SibiDocument62 pagesDiabetes Mellitus Final SibiSibi JohnNo ratings yet
- Print Article - Glucose Tests - Glucose Test - Blood Sugar - Blood Glucose - Fasting Blood Glucose - Oral Glucose Tolerance Test - OGTT - GTT - Urine Glucose - Lab Tests OnlineDocument9 pagesPrint Article - Glucose Tests - Glucose Test - Blood Sugar - Blood Glucose - Fasting Blood Glucose - Oral Glucose Tolerance Test - OGTT - GTT - Urine Glucose - Lab Tests OnlineHinaRaviNo ratings yet
- The Test: How Is It Used?Document5 pagesThe Test: How Is It Used?julia_jayronwaldoNo ratings yet
- Diabetes Mellitus: Salient Features of Type 1 Am D Type 2 DMDocument20 pagesDiabetes Mellitus: Salient Features of Type 1 Am D Type 2 DMPriyanka Karnik100% (1)
- Metabolic Disorders Diabetes HandoutDocument21 pagesMetabolic Disorders Diabetes HandoutEdelen GaleNo ratings yet
- GTT & HbA1cDocument35 pagesGTT & HbA1cHimani JheetayNo ratings yet
- 01 - CLS 382 - 443 - DMDocument19 pages01 - CLS 382 - 443 - DMamalNo ratings yet
- Presentation On: Kgmu College of NursingDocument42 pagesPresentation On: Kgmu College of NursingSweety YadavNo ratings yet
- Pre Gestational ConditionsDocument17 pagesPre Gestational Conditionslarissedeleon100% (2)
- Diabetes in Pregnancy: DR Omar Abu-AzzamDocument36 pagesDiabetes in Pregnancy: DR Omar Abu-AzzamRoba Mohmed AlamroNo ratings yet
- Insulin Secretion and FunctionDocument8 pagesInsulin Secretion and FunctionWendy EscalanteNo ratings yet
- Diabetes Mellitus & Pregnancy by D.a.mehtaDocument31 pagesDiabetes Mellitus & Pregnancy by D.a.mehtadr.d.a.mehta11No ratings yet
- H Ypoglycemia: Divisi Endokrin-Metabolik Departemen Ilmu Penyakit Dalam FK USU/ RSUP H Adam Malik MedanDocument36 pagesH Ypoglycemia: Divisi Endokrin-Metabolik Departemen Ilmu Penyakit Dalam FK USU/ RSUP H Adam Malik MedanririsNo ratings yet
- Gestational Diabetes: By: Fatima ChoudaryDocument26 pagesGestational Diabetes: By: Fatima Choudaryari naNo ratings yet
- CP2 MidtermsDocument278 pagesCP2 MidtermsDiana WadwasinNo ratings yet
- GTT My PresentationDocument33 pagesGTT My PresentationSrikrishnaNo ratings yet
- DIABETES MELLITUS FinalDocument83 pagesDIABETES MELLITUS FinalYuvi Yuvaraj100% (1)
- Neonatal HypoglycemiaDocument5 pagesNeonatal Hypoglycemiadiana rossNo ratings yet
- زدوززDocument13 pagesزدوززAli AzizNo ratings yet
- Laboratory Diagnosis and Monitoring of Diabetes MellitusDocument65 pagesLaboratory Diagnosis and Monitoring of Diabetes MellitusSonia Afika AzizaNo ratings yet
- Glucose TestDocument12 pagesGlucose Testislam.o.walyNo ratings yet
- Diabetes Mellitus Type 1Document19 pagesDiabetes Mellitus Type 1QwertyNo ratings yet
- DIABETES BookDocument2 pagesDIABETES BookMaria Kimberly NazarenoNo ratings yet
- Neonatal HypoglycemiaDocument22 pagesNeonatal HypoglycemiaRashmi KATTINo ratings yet
- DiabetesDocument14 pagesDiabetesRashmi ThakurNo ratings yet
- DiabetesDocument99 pagesDiabetes489226fahimNo ratings yet
- Know Diabetes For No Diabetes: DR U.S Shilpi M.D, (Physician) BhelhospitalDocument37 pagesKnow Diabetes For No Diabetes: DR U.S Shilpi M.D, (Physician) BhelhospitalAnonymous ysrxggk21cNo ratings yet
- Diabetes MellitusDocument36 pagesDiabetes Mellitusayeshakhan1060774No ratings yet
- Diagnosis of Diabetes MellitusDocument23 pagesDiagnosis of Diabetes MellitusNkosinathi ShongweNo ratings yet
- Diabetes in PregnancyDocument88 pagesDiabetes in PregnancyKathleenZunigaNo ratings yet
- Blood Glucose Practical Handout For 2nd Year MBBSDocument10 pagesBlood Glucose Practical Handout For 2nd Year MBBSIMDCBiochemNo ratings yet
- DIABETISDocument52 pagesDIABETISNeeraja M SureshNo ratings yet
- Lecture 10Document9 pagesLecture 10Hawaid AhmadNo ratings yet
- CARBOHYDRATE METABOLISM AND DISORDERS (Herbal Med)Document44 pagesCARBOHYDRATE METABOLISM AND DISORDERS (Herbal Med)AhjNo ratings yet
- DM in PregDocument32 pagesDM in Pregbryanpei23No ratings yet
- Diabetes Mellitus: NCM 116 Metabolism & Endocrine BSN 3Document19 pagesDiabetes Mellitus: NCM 116 Metabolism & Endocrine BSN 3Karen Kate AblesNo ratings yet
- Diabetes and PregnancyDocument63 pagesDiabetes and PregnancyAyesha KhatunNo ratings yet
- Session 4 Phase 2Document65 pagesSession 4 Phase 2ayoub shams mohamedNo ratings yet
- Carbohydrates Metabolism and Diabetes MellitusDocument63 pagesCarbohydrates Metabolism and Diabetes Mellitusapi-19641337No ratings yet
- Diabetes Mellitus: Investagtion, Diagnosis & Management: DR - Vivek Reddy 1 M.D.SDocument36 pagesDiabetes Mellitus: Investagtion, Diagnosis & Management: DR - Vivek Reddy 1 M.D.SBHEEMREDDY VIVEKREDDY100% (1)
- Chapter 4 Carbohydrate DisorderDocument26 pagesChapter 4 Carbohydrate DisorderNida RidzuanNo ratings yet
- Gestational Diabetes PowerpointDocument26 pagesGestational Diabetes Powerpointteritohaha100% (2)
- Diabetes MellitusDocument22 pagesDiabetes MellitusAnburaj JamesNo ratings yet
- Glucose PDFDocument36 pagesGlucose PDFHerzl Hali V. HermosaNo ratings yet
- Oral Glucose Tolerance TestDocument29 pagesOral Glucose Tolerance TestAhmedmmhNo ratings yet
- New Hypoglycmemia 1Document61 pagesNew Hypoglycmemia 1Suravi DuttaNo ratings yet
- Pathophysiology of DiabetesDocument88 pagesPathophysiology of DiabetesCahya SetiyaNo ratings yet
- Gestational Diabetes Mellitus 173278680Document22 pagesGestational Diabetes Mellitus 173278680njnaasuramyaNo ratings yet
- Nursing Care of Patients With Diabetes MellitusDocument43 pagesNursing Care of Patients With Diabetes MellitusRashida RuwaNo ratings yet
- Diabetes Mellitus: Regulation of Blood GlucoseDocument65 pagesDiabetes Mellitus: Regulation of Blood GlucoseReggae BautistaNo ratings yet
- Ginni Rani NewDocument41 pagesGinni Rani NewEkta RajputNo ratings yet
- Distillation and DeionizerDocument26 pagesDistillation and Deionizerhamadadodo7No ratings yet
- Use of Water BathDocument1 pageUse of Water Bathhamadadodo7No ratings yet
- Chloride Test in WaterDocument4 pagesChloride Test in Waterhamadadodo7No ratings yet
- Centrifuge: (January 2009)Document11 pagesCentrifuge: (January 2009)hamadadodo7No ratings yet
- Care and Maintenance of AutoclaveDocument1 pageCare and Maintenance of Autoclavehamadadodo7No ratings yet
- Boro Cili CateDocument9 pagesBoro Cili Catehamadadodo7No ratings yet
- 18 - Flow Cytometry and Introduction To Molecular PathologyDocument11 pages18 - Flow Cytometry and Introduction To Molecular Pathologyhamadadodo7No ratings yet
- Test Banks For Textbook of Diagnostic MicrobiologyDocument1 pageTest Banks For Textbook of Diagnostic Microbiologyhamadadodo70% (1)
- Test Banks For Clinical Hematology and Fundamentals of HemostasisDocument1 pageTest Banks For Clinical Hematology and Fundamentals of Hemostasishamadadodo7No ratings yet
- 22 - ImmunohematologyDocument6 pages22 - Immunohematologyhamadadodo7No ratings yet
- 08 - Gastrointestinal and Exocrine Pancreatic FunctionDocument7 pages08 - Gastrointestinal and Exocrine Pancreatic Functionhamadadodo7No ratings yet
- 21 - Thyroid Function TestsDocument2 pages21 - Thyroid Function Testshamadadodo7No ratings yet
- 02 - Examination of Blood and Bone Marrow HematologyDocument3 pages02 - Examination of Blood and Bone Marrow Hematologyhamadadodo7No ratings yet
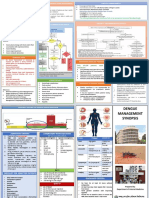
- Dengue Management Synopsis BSMMUDocument2 pagesDengue Management Synopsis BSMMURakibk65No ratings yet
- Buotan Si June Buotan Jud Si JuneDocument13 pagesBuotan Si June Buotan Jud Si JuneMajestic RavenNo ratings yet
- Acute Toxic-Metabolic Encephalopathy in Adults - UpToDateDocument19 pagesAcute Toxic-Metabolic Encephalopathy in Adults - UpToDateBruno FernandesNo ratings yet
- Levemir Flex PenDocument2 pagesLevemir Flex PenDika FrantikoNo ratings yet
- Literature Review Type 2 DiabetesDocument4 pagesLiterature Review Type 2 Diabetesafmaadalrefplh100% (1)
- Type 1 Diabetes: Basis of Causes and Away of PreventionDocument11 pagesType 1 Diabetes: Basis of Causes and Away of PreventionOpenaccess Research paperNo ratings yet
- Insulin Adjustment Workbook CompleteDocument53 pagesInsulin Adjustment Workbook CompleteDiabestes-stuff100% (1)
- A Comprehensive: Health Analysis ReportDocument37 pagesA Comprehensive: Health Analysis ReportSandeep KumarNo ratings yet
- Care of A Child With Diabetes Mellitus: Guidelines For ParentsDocument12 pagesCare of A Child With Diabetes Mellitus: Guidelines For ParentsNivedita MishraNo ratings yet
- Blood Glucose MonitoringDocument4 pagesBlood Glucose MonitoringAman ChaudharyNo ratings yet
- Diabetes PPT FianlDocument31 pagesDiabetes PPT FianlUqba Mishal100% (1)
- Carbohydrates Take Longer To Break Down, and Provide A Longer Lasting EnergyDocument2 pagesCarbohydrates Take Longer To Break Down, and Provide A Longer Lasting EnergyAlvenia Meilina EdnisariNo ratings yet
- Unit 4: Medical EmergenciesDocument44 pagesUnit 4: Medical EmergenciesMR々๛ AKMツNo ratings yet
- Case Studies - Type 1 DiabetesDocument4 pagesCase Studies - Type 1 Diabeteszenagit1234560% (2)
- Approach To Hypoglycemia in Infants and Children - UpToDateDocument31 pagesApproach To Hypoglycemia in Infants and Children - UpToDateyohanes gabriel dwirianto w.aNo ratings yet
- Complete Remission in Newly Diagnosed Type 1 Diabetes Mellitus PatientDocument3 pagesComplete Remission in Newly Diagnosed Type 1 Diabetes Mellitus PatientAdvanced Research Publications100% (1)
- Gudoy, Charies Jamille 12-WeierstrassDocument4 pagesGudoy, Charies Jamille 12-WeierstrasschaNo ratings yet
- NCLEX Guide CompilationDocument63 pagesNCLEX Guide CompilationVal Solidum100% (2)
- Humalog Drug StudyDocument3 pagesHumalog Drug StudyKristinelou Marie ReynaNo ratings yet
- Test Sas 16, 17 & 18 Nur 151 Cooa A4: Questions 1 To 10Document2 pagesTest Sas 16, 17 & 18 Nur 151 Cooa A4: Questions 1 To 10Sistine Rose LabajoNo ratings yet
- Manual On Surgery Part BDocument6 pagesManual On Surgery Part BSojiNo ratings yet
- CC Intensive Rationale PDFDocument6 pagesCC Intensive Rationale PDFAnne MorenoNo ratings yet
- Mounjaro UspiDocument19 pagesMounjaro UspiayaznptiNo ratings yet
- Volten VR4 JurnalDocument7 pagesVolten VR4 JurnalAndi Ahsan NurNo ratings yet
- Eating Well With Diabetes When You Have A Poor AppetiteDocument28 pagesEating Well With Diabetes When You Have A Poor AppetiteRitika SinghalNo ratings yet
- Hyperglycemia Algorithm 2Document1 pageHyperglycemia Algorithm 2damondouglasNo ratings yet
- Insulin ApidraDocument2 pagesInsulin ApidraDivine Grace Arreglo AbingNo ratings yet
- PDF Hosted at The Radboud Repository of The Radboud UniversityDocument19 pagesPDF Hosted at The Radboud Repository of The Radboud UniversityAhmed RabieNo ratings yet