Download as pdf or txt
You might also like
- Appendicitis (Case Study)Document40 pagesAppendicitis (Case Study)Cherr Noll Sanchez100% (1)
- Nursing Research ReportDocument15 pagesNursing Research Reportapi-546467833No ratings yet
- Clinical Diagnosis and Management of Ocular Myasthenia GravisDocument11 pagesClinical Diagnosis and Management of Ocular Myasthenia GravisAinul NurrahmahNo ratings yet
- Dong KimberlyDocument7 pagesDong KimberlyalmaNo ratings yet
- 100255-Article Text-1482-2-10-20220311Document6 pages100255-Article Text-1482-2-10-20220311Fachry RahmanNo ratings yet
- Clinical CasesDocument49 pagesClinical Casesnorfitri hadeyNo ratings yet
- Medicine: Sumatriptan-Induced Angle-Closure GlaucomaDocument4 pagesMedicine: Sumatriptan-Induced Angle-Closure GlaucomanidaNo ratings yet
- A Rare Case of Terson Syndrome With Subarachnoid HemorrhageDocument12 pagesA Rare Case of Terson Syndrome With Subarachnoid HemorrhageNinaNo ratings yet
- Atypical Presentation of Optic Neuritis in Multiple Sclerosis - Dian ParamitasariDocument15 pagesAtypical Presentation of Optic Neuritis in Multiple Sclerosis - Dian ParamitasariGufront MustofaNo ratings yet
- Esferofauia Aislada y GlaucomaDocument3 pagesEsferofauia Aislada y GlaucomaManuel VasquezNo ratings yet
- Penatalaksanaan Glaukoma Sekunder Refrakter Pada Implantasi Lensa Intraokular Bilik Mata Depan - Pauline Meilisa SihiteDocument13 pagesPenatalaksanaan Glaukoma Sekunder Refrakter Pada Implantasi Lensa Intraokular Bilik Mata Depan - Pauline Meilisa SihiteZikra Herlius14No ratings yet
- Orbital Apex Syndrome Secondary To Herpes Zoster OphthalmicusDocument4 pagesOrbital Apex Syndrome Secondary To Herpes Zoster OphthalmicusYosiita KartinaaNo ratings yet
- Vogt Koyanagi Harada SyndromeDocument9 pagesVogt Koyanagi Harada SyndromeBianca PavelNo ratings yet
- Angle Recession GlaucomaDocument15 pagesAngle Recession GlaucomaDia Asri RusliNo ratings yet
- Downloadophthalmology Cases All Team PDF PDF Free - HTMLDocument23 pagesDownloadophthalmology Cases All Team PDF PDF Free - HTMLDương Yến TrânNo ratings yet
- Traumatic Hyphema: A Teaching Case Report: Priscilla Lenihan, OD Dorothy Hitchmoth, OD, FAAODocument9 pagesTraumatic Hyphema: A Teaching Case Report: Priscilla Lenihan, OD Dorothy Hitchmoth, OD, FAAOMarshaNo ratings yet
- Diagnosis Dan Tatalaksana Steroid Induced Glaucoma - Andivan Rahman PDFDocument11 pagesDiagnosis Dan Tatalaksana Steroid Induced Glaucoma - Andivan Rahman PDFMarini Yusufina LubisNo ratings yet
- Letters To The EditorDocument8 pagesLetters To The EditorGheavita Chandra DewiNo ratings yet
- Prospective Evaluation of Acupuncture As Treatment For GlaucomaDocument10 pagesProspective Evaluation of Acupuncture As Treatment For Glaucoma16.11Hz MusicNo ratings yet
- Penatalaksanaan Pasien Glaukoma Sudut Terbuka Dengan PemasanganintanmaulaDocument10 pagesPenatalaksanaan Pasien Glaukoma Sudut Terbuka Dengan PemasanganintanmaulaShela GranityaNo ratings yet
- The Chiropractic Care of An Infant Female With A Medical Diagnosis of Strabismus: A Case ReportDocument4 pagesThe Chiropractic Care of An Infant Female With A Medical Diagnosis of Strabismus: A Case ReportAndrea Parisio-FerraroNo ratings yet
- Ace SetiawanDocument11 pagesAce SetiawanGlaucoma UnhasNo ratings yet
- Jurnal StrabismusDocument3 pagesJurnal StrabismusBonita AsyigahNo ratings yet
- Diagnosis BandingDocument10 pagesDiagnosis BandingIntan Rahmi NasyaNo ratings yet
- Cogan-Reese Syndrome - A Rare Case of Unilateral GlaucomaDocument8 pagesCogan-Reese Syndrome - A Rare Case of Unilateral GlaucomaDr. Abhishek OnkarNo ratings yet
- Lapkas Glaukoma Pemasangan Implan GDD Lapkas Glaukoma (AutoRecovered)Document14 pagesLapkas Glaukoma Pemasangan Implan GDD Lapkas Glaukoma (AutoRecovered)Vincent RoorohNo ratings yet
- 86 Normal Low Tension Glaucoma PDFDocument4 pages86 Normal Low Tension Glaucoma PDFSherZalattha KuchikiElfNo ratings yet
- Ocular Myasthenia Gravis in Children A Case Report - Muhammad Arief MunandarDocument10 pagesOcular Myasthenia Gravis in Children A Case Report - Muhammad Arief Munandarirvan rahmanNo ratings yet
- 1 PBDocument4 pages1 PBRian YupitaNo ratings yet
- Adverse Drug Reaction FormDocument2 pagesAdverse Drug Reaction FormAhmad SaeedNo ratings yet
- Bilatteral Acute Angle Closure GlaucomaDocument17 pagesBilatteral Acute Angle Closure GlaucomaAhmed_Algihady_2987No ratings yet
- Case Report Urretz Zavalia SyndromeDocument6 pagesCase Report Urretz Zavalia SyndromeAi HidayatNo ratings yet
- Case ReportDocument7 pagesCase ReportJeel GaralaNo ratings yet
- A Review of Optic NeuritisDocument5 pagesA Review of Optic NeuritissatrianiNo ratings yet
- Questions and Answer Group 3 "Glaucoma" Nama: Gustin Ibrahim Umamah Kelas: A S1 FARMASI 2017 NIM: 821417021Document13 pagesQuestions and Answer Group 3 "Glaucoma" Nama: Gustin Ibrahim Umamah Kelas: A S1 FARMASI 2017 NIM: 821417021Afni YunitaNo ratings yet
- Opth 8 1351Document5 pagesOpth 8 1351Muhammad Halil GibranNo ratings yet
- Tatalaksana Dan Prognosis Severe Visual Impairment Pada Miopia Patologi - Nikho Melga ShalimDocument14 pagesTatalaksana Dan Prognosis Severe Visual Impairment Pada Miopia Patologi - Nikho Melga ShalimOt PtkNo ratings yet
- PDF StrabismusDocument1 pagePDF StrabismusirawadiputraNo ratings yet
- Association Between Hypertriglyceridemia and Open Angle Glaucoma: A Case ReportDocument3 pagesAssociation Between Hypertriglyceridemia and Open Angle Glaucoma: A Case Reportsyntacs skNo ratings yet
- Case IIM Tama NewDocument11 pagesCase IIM Tama NewAryati PutriNo ratings yet
- Penatalaksanaan Pasien Dengan Sudut Tertutup Primer - DegianaDocument13 pagesPenatalaksanaan Pasien Dengan Sudut Tertutup Primer - Degianacindy sweeteniaNo ratings yet
- Topiramate Induced GlaucomaDocument38 pagesTopiramate Induced GlaucomaArnob ShahriarNo ratings yet
- Ni Hms 419332Document10 pagesNi Hms 419332Monica Lauretta Sembiring IINo ratings yet
- American Journal of Emergency Medicine: Dietrich Jehle Mary Claire Lark, Clay O'BrienDocument3 pagesAmerican Journal of Emergency Medicine: Dietrich Jehle Mary Claire Lark, Clay O'BrienGufront MustofaNo ratings yet
- Neurosyphilis Masquerading As An Acute Adie's Tonic Pupil: Report of A CaseDocument6 pagesNeurosyphilis Masquerading As An Acute Adie's Tonic Pupil: Report of A CaseOlvaria MisfaNo ratings yet
- Catarta e HipoparatiroidismoDocument3 pagesCatarta e HipoparatiroidismoBernardo RomeroNo ratings yet
- Departemen Ilmu Kesehatan Mata Fakultas Kedokteran Universitas Padjadjaran Pusat Mata Nasional Rumah Sakit Mata Cicendo BandungDocument11 pagesDepartemen Ilmu Kesehatan Mata Fakultas Kedokteran Universitas Padjadjaran Pusat Mata Nasional Rumah Sakit Mata Cicendo BandungBambang RinandiNo ratings yet
- Tatalaksana Operatif Dan Pascaoperatif Pada Pasien Juvenile Open Angle Glaucoma JOAG - Andreas Lukita HalimDocument14 pagesTatalaksana Operatif Dan Pascaoperatif Pada Pasien Juvenile Open Angle Glaucoma JOAG - Andreas Lukita HalimINDRINo ratings yet
- EENT Weekly TestDocument8 pagesEENT Weekly Testrajivsingal248No ratings yet
- Mindanao Medical Foundation CollegeDocument4 pagesMindanao Medical Foundation Collegeleidysaves0821No ratings yet
- Laporan Kasus SACG Dan Katarak Kongenital Pada AniridiaDocument15 pagesLaporan Kasus SACG Dan Katarak Kongenital Pada AniridiaIntan EkarulitaNo ratings yet
- Asian Upper Eyelid Blepharoplasty Sebagai Tatalaksana Dermatokalasis - Adessa RachmaDocument11 pagesAsian Upper Eyelid Blepharoplasty Sebagai Tatalaksana Dermatokalasis - Adessa Rachmafadil ahmadi100% (1)
- Running Head: A Patient Who Has Glaucoma 1Document10 pagesRunning Head: A Patient Who Has Glaucoma 1Alonso LugoNo ratings yet
- Revisi Ke-3 Journal Glaucoma (Group 12)Document12 pagesRevisi Ke-3 Journal Glaucoma (Group 12)TaschiaNo ratings yet
- Diagnosis Dan Tatalaksana Pasien Dengan Insufisiensi Akomodasi - Sri Hudaya WidihasthaDocument13 pagesDiagnosis Dan Tatalaksana Pasien Dengan Insufisiensi Akomodasi - Sri Hudaya WidihasthamalaNo ratings yet
- Orbital Apex Syndrome With Encephalitis A Rare and Serious Complication of Herpes Zoster Opthalmicus - Ludwig Melino Tjokrovonco 2Document12 pagesOrbital Apex Syndrome With Encephalitis A Rare and Serious Complication of Herpes Zoster Opthalmicus - Ludwig Melino Tjokrovonco 2Handi KrisnaniNo ratings yet
- Grand Rounds Glaucoma NTGDocument37 pagesGrand Rounds Glaucoma NTGRon TongbaiNo ratings yet
- Soal TryoutDocument3 pagesSoal Tryouthanidya fazwatNo ratings yet
- A Case of Angle-Closure Glaucoma, Cataract, Nanophthalmos and Spherophakia in Oculo-Dento-Digital SyndromeDocument3 pagesA Case of Angle-Closure Glaucoma, Cataract, Nanophthalmos and Spherophakia in Oculo-Dento-Digital SyndromeSriana K. LaliyoNo ratings yet
- 100122-Article Text-1484-2-10-20220311Document11 pages100122-Article Text-1484-2-10-20220311muzakiNo ratings yet
- IJCRR Nov2020 Vol12 Issue22Document9 pagesIJCRR Nov2020 Vol12 Issue22Aravind KumarNo ratings yet
- ACT TherapyDocument7 pagesACT TherapyPrince AroraNo ratings yet
- Associated Persons: Bertram Welton Sippy Description: TreatmentDocument5 pagesAssociated Persons: Bertram Welton Sippy Description: Treatmentkill_noj_olarcNo ratings yet
- Shoma Morita - WikipediaDocument8 pagesShoma Morita - WikipediacamicrisNo ratings yet
- Magnesium in Women's Health and Gynecology: Shawna Tonick, Ozgul Muneyyirci-DelaleDocument9 pagesMagnesium in Women's Health and Gynecology: Shawna Tonick, Ozgul Muneyyirci-DelaleyoggsssNo ratings yet
- Attitudinize Psychotherapy NewDocument30 pagesAttitudinize Psychotherapy NewLeenah ÃskareeNo ratings yet
- Lauren Humphrey ResumeDocument2 pagesLauren Humphrey Resumeapi-242376719No ratings yet
- Penggunaan Ekstrak Buah Adas Dalam Mengurangi Dismenore Pada Remaja Putri Hermayanti, Gita Kostania, Siti YulaikahDocument8 pagesPenggunaan Ekstrak Buah Adas Dalam Mengurangi Dismenore Pada Remaja Putri Hermayanti, Gita Kostania, Siti YulaikahAnas TasiaNo ratings yet
- Maternal and Child Healthe Nursing MCQ 6Document18 pagesMaternal and Child Healthe Nursing MCQ 6shanika100% (2)
- Spine Oncology, An Issue of Orthopedic Clinics PDFDocument168 pagesSpine Oncology, An Issue of Orthopedic Clinics PDFThanh Le DangNo ratings yet
- Morning Report Tension Type HeadacheDocument12 pagesMorning Report Tension Type HeadacheLintan FarzNo ratings yet
- Nutrition Repaired)Document10 pagesNutrition Repaired)Brylle MirandaNo ratings yet
- Kanner 2016Document11 pagesKanner 2016Izara Maité Mondragón MorenoNo ratings yet
- Presentation 307w Correct One MeatballsDocument24 pagesPresentation 307w Correct One Meatballsapi-347761303No ratings yet
- Lecture 1 Historical Aspects of Surgery (Core)Document27 pagesLecture 1 Historical Aspects of Surgery (Core)Charwinth KankaNo ratings yet
- Kpop Body Challenge Diet FinalDocument5 pagesKpop Body Challenge Diet FinalJaneNo ratings yet
- Mcfadden S System o 00 Mac FDocument144 pagesMcfadden S System o 00 Mac FcgonzjamNo ratings yet
- Livro - Acido LáticoDocument670 pagesLivro - Acido LáticoLuciana CoelhoNo ratings yet
- Behavior TheoryDocument6 pagesBehavior Theoryapi-401555861No ratings yet
- Pharmacology of Thyroid Hormones and Anti Thyroid Drugs For Second Year Medicine StudentsDocument48 pagesPharmacology of Thyroid Hormones and Anti Thyroid Drugs For Second Year Medicine StudentsAmanuel MaruNo ratings yet
- Chocolate: Chocolate Is A Raw or Processed Food Produced From The Seed of The TropicalDocument7 pagesChocolate: Chocolate Is A Raw or Processed Food Produced From The Seed of The TropicalNyimas Irina SilvaniNo ratings yet
- Traumatic Brain Injury A Case Report: SCORE:40/50Document10 pagesTraumatic Brain Injury A Case Report: SCORE:40/50Allan CastroNo ratings yet
- Atm 04 08 160Document9 pagesAtm 04 08 160manalNo ratings yet
- Mechanical Ventilation SeminarDocument82 pagesMechanical Ventilation Seminarrajan kumar91% (22)
- Clearing Clutter With EFT BonusDocument10 pagesClearing Clutter With EFT BonusKristen Hammer75% (4)
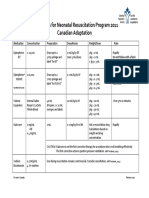
- Medications For Neonatal Resuscitation Program 2011 Canadian AdaptationDocument1 pageMedications For Neonatal Resuscitation Program 2011 Canadian AdaptationrubymayNo ratings yet
- The Vibration of Exceptional Health - Carol LookDocument5 pagesThe Vibration of Exceptional Health - Carol LookMichael CliftonNo ratings yet
- CipaDocument15 pagesCipaapi-247628136No ratings yet
- Yang Line Hani CD 10Document13 pagesYang Line Hani CD 10Janine NogueraNo ratings yet