
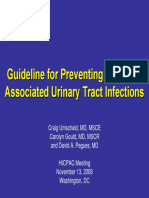
Trial Without Catheter TWOC Protocol 1991
Trial Without Catheter TWOC Protocol 1991
You might also like
- RAC Exam I Test Questions - Flash Cards Answer - KeyDocument101 pagesRAC Exam I Test Questions - Flash Cards Answer - KeyYesinta Diandra100% (4)
- Essentials For Nursing Practice 8th Edition Potter Test Bank DownloadDocument14 pagesEssentials For Nursing Practice 8th Edition Potter Test Bank DownloadJose Stepro100% (23)
- Consensus Guidelines On Point of Care Testing in Hospitals: I. BackgroundDocument4 pagesConsensus Guidelines On Point of Care Testing in Hospitals: I. BackgroundDocAxi Maximo Jr Axibal67% (3)
- Urinary Catheterisation and Catheter Care in Adults GuidelinesDocument37 pagesUrinary Catheterisation and Catheter Care in Adults GuidelinesAllend Reidene Viyar100% (1)
- Nurse Driven Protocols ArticleDocument7 pagesNurse Driven Protocols ArticlePaolo VegaNo ratings yet
- Groupd Ebp PresentationDocument38 pagesGroupd Ebp Presentationapi-384226081No ratings yet
- Bundles in Infection Prevention and SafetyDocument15 pagesBundles in Infection Prevention and SafetyInfectologia DiagnosticaNo ratings yet
- Catheter-Associated Urinary Tract Infection Care BundleDocument3 pagesCatheter-Associated Urinary Tract Infection Care BundleAnisaNo ratings yet
- Emergency Surgery FrameworkDocument36 pagesEmergency Surgery Frameworkhalosunyrtimr6No ratings yet
- Management of Patients With Long-Term Indwelling Urinary Catheters: A Review of GuidelinesDocument26 pagesManagement of Patients With Long-Term Indwelling Urinary Catheters: A Review of GuidelinesFaozan FikriNo ratings yet
- Appendix B. Urinary Catheterization - Sample Policy: AHRQ Safety Program For Reducing CAUTI in HospitalsDocument4 pagesAppendix B. Urinary Catheterization - Sample Policy: AHRQ Safety Program For Reducing CAUTI in HospitalsMhathea ArandidNo ratings yet
- TWOC Procedure GuidanceDocument6 pagesTWOC Procedure GuidanceKall VishNo ratings yet
- ISID InfectionGuide Chapter16Document15 pagesISID InfectionGuide Chapter16Nishtha Singh ChauhanNo ratings yet
- Uti Hicpac11 08Document40 pagesUti Hicpac11 08Koes Reenee EndroNo ratings yet
- Catheter-Associated Urinary Tract Infections and The Protocols For The Removal of Foley Catheters For Their PreventionDocument7 pagesCatheter-Associated Urinary Tract Infections and The Protocols For The Removal of Foley Catheters For Their PreventionCarlos I. RomeroNo ratings yet
- Admission and Discharge ProtocolDocument38 pagesAdmission and Discharge Protocolatinkut eteneshNo ratings yet
- Australia Isolation Rooms 2007Document48 pagesAustralia Isolation Rooms 2007jonathan_carretasNo ratings yet
- Essais Cliniques Decentralises VF enDocument15 pagesEssais Cliniques Decentralises VF enSchmoutNo ratings yet
- Eras Bps Final Nov2017 2Document24 pagesEras Bps Final Nov2017 2Wardah Fauziah El SofwanNo ratings yet
- Articulo en InglesDocument8 pagesArticulo en Inglesdante yonathan villegas lozanoNo ratings yet
- Catheter-Associated Urinary Tract InfectionsDocument20 pagesCatheter-Associated Urinary Tract Infectionsapi-315336673No ratings yet
- Guidelines For The Prevention of Catheterassociated Urinary Tract InfectionDocument54 pagesGuidelines For The Prevention of Catheterassociated Urinary Tract InfectioncateterdoblejotaNo ratings yet
- C0063 Specialty Guide - Respiratory and Coronavirus - v1 - 26 MarchDocument4 pagesC0063 Specialty Guide - Respiratory and Coronavirus - v1 - 26 MarchKevo VillagranNo ratings yet
- Qi Group Project - e C y TDocument10 pagesQi Group Project - e C y Tapi-302732994No ratings yet
- Roles of Bone Marrow Transplant Unit Nurses IncludesDocument10 pagesRoles of Bone Marrow Transplant Unit Nurses IncludesGleden UmayamNo ratings yet
- Admissions and Discharge: GuidelinesDocument26 pagesAdmissions and Discharge: GuidelinesIshaan TalrejaNo ratings yet
- Decontamination of Equipment Environment Policy 4.1Document29 pagesDecontamination of Equipment Environment Policy 4.1Rex Lagunzad FloresNo ratings yet
- Cathfoleyre 4859 FaDocument2 pagesCathfoleyre 4859 FaNeil OsborneNo ratings yet
- ACI Urology Bladder IrrigationDocument20 pagesACI Urology Bladder IrrigationOlivia BawaedaNo ratings yet
- IHFG Part B Renal Dialysis UnitDocument18 pagesIHFG Part B Renal Dialysis Unitmorton1472No ratings yet
- Adult Nasogastric Tube Insertion Procedure & Management PolicyDocument0 pagesAdult Nasogastric Tube Insertion Procedure & Management PolicyRubelyn Joy LazarteNo ratings yet
- CVC PolicyDocument15 pagesCVC Policyseaturtles505No ratings yet
- APH Surgical Service ProtocolDocument31 pagesAPH Surgical Service Protocolsami ketema50% (2)
- University of Colorado NICHE Practice Survey SummaryDocument48 pagesUniversity of Colorado NICHE Practice Survey Summarybocah_britpopNo ratings yet
- Pre Op 2010Document37 pagesPre Op 2010Tawona DhlakamaNo ratings yet
- Catheter Care: RCN Guidance For Health Care ProfessionalsDocument82 pagesCatheter Care: RCN Guidance For Health Care ProfessionalsSudin KumarNo ratings yet
- 2016 Toronto ERAS - STOMA - BPS - FINAL - 2018Document25 pages2016 Toronto ERAS - STOMA - BPS - FINAL - 2018durdane palabiyik yilmazNo ratings yet
- Strategies To Prevent Catheter Associated Urinary Tract Infections in Acute Care Hospitals 2022 UpdateDocument23 pagesStrategies To Prevent Catheter Associated Urinary Tract Infections in Acute Care Hospitals 2022 UpdateMega ArfiyantiNo ratings yet
- Guidanceclinicaltrials Covid19 en 1Document22 pagesGuidanceclinicaltrials Covid19 en 1VeraNo ratings yet
- Guidelines For Syringe Driver Management in Palliative Care: Developed byDocument57 pagesGuidelines For Syringe Driver Management in Palliative Care: Developed byFirmanNo ratings yet
- SOP-10-008 Suction July 20 2010 PDFDocument23 pagesSOP-10-008 Suction July 20 2010 PDFSalsabilla KimikoNo ratings yet
- Sop Number Title of SOP Author Consultation With StakeholdersDocument23 pagesSop Number Title of SOP Author Consultation With StakeholdersMr. BamsNo ratings yet
- Oncology Haematology 24 Hour TriageDocument28 pagesOncology Haematology 24 Hour TriageZaher MachadoNo ratings yet
- Get ResourceDocument28 pagesGet ResourceWalaa ElleithyNo ratings yet
- Guidanceclinicaltrials Covid19 Pres en PDFDocument65 pagesGuidanceclinicaltrials Covid19 Pres en PDFMarcM77No ratings yet
- انترودكشن عمليDocument13 pagesانترودكشن عمليRana KhaledNo ratings yet
- Qsen Project Urinary Catheter ComplicationsDocument18 pagesQsen Project Urinary Catheter Complicationsapi-316643564No ratings yet
- CAUTI Bundle of Care PDFDocument3 pagesCAUTI Bundle of Care PDFArvie PavinoNo ratings yet
- Waht-Inf-040 V2.1Document20 pagesWaht-Inf-040 V2.1Kheanry AlejandroNo ratings yet
- Selecting A Urinary Catheter and Drainage System: John RobinsonDocument6 pagesSelecting A Urinary Catheter and Drainage System: John RobinsonFrancisca BartschNo ratings yet
- Protocols For Day Care Anaesthesia: Ministry of Health MalaysiaDocument27 pagesProtocols For Day Care Anaesthesia: Ministry of Health MalaysiasitiNo ratings yet
- Advanced Infection Prevention and PDFDocument28 pagesAdvanced Infection Prevention and PDFWardah Fauziah El SofwanNo ratings yet
- Cauti Prevention - UpdatedDocument25 pagesCauti Prevention - Updatedapi-340518242No ratings yet
- IHOP - 9.13.25 - Time Out Universal Protocol For Invasive and Surgical ProceduresDocument3 pagesIHOP - 9.13.25 - Time Out Universal Protocol For Invasive and Surgical Proceduresmaxxer1985No ratings yet
- Cauti PreventionDocument25 pagesCauti Preventionapi-340511634No ratings yet
- Manual for Iv Therapy Procedures & Pain Management: Fourth EditionFrom EverandManual for Iv Therapy Procedures & Pain Management: Fourth EditionNo ratings yet
- TÉCNICAS DEL AUXILIAR DE ENFERMERÍA EN EL ÁREA DE QUIRÓFANOFrom EverandTÉCNICAS DEL AUXILIAR DE ENFERMERÍA EN EL ÁREA DE QUIRÓFANONo ratings yet
- Pustjens2020 Article GuidelinesForTheManagementOfMyDocument15 pagesPustjens2020 Article GuidelinesForTheManagementOfMyganangahimsaNo ratings yet
- Abstracts: Case Reports: Indonesian Journal of CardiologyDocument63 pagesAbstracts: Case Reports: Indonesian Journal of CardiologyganangahimsaNo ratings yet
- Differential Diagnosis of Cardiogenic Syncope and Seizure DisordersDocument6 pagesDifferential Diagnosis of Cardiogenic Syncope and Seizure DisordersganangahimsaNo ratings yet
- Comparative Safety of Sulfonylurea and Metformin Monotherapy On The Risk of Heart Failure: A Cohort StudyDocument29 pagesComparative Safety of Sulfonylurea and Metformin Monotherapy On The Risk of Heart Failure: A Cohort StudyganangahimsaNo ratings yet
- Triatmo Budiyuwono SPJP (K), FIHA, FAPSICDocument40 pagesTriatmo Budiyuwono SPJP (K), FIHA, FAPSICganangahimsaNo ratings yet
- Regulatory T Cell I AtheroschlerisisDocument13 pagesRegulatory T Cell I AtheroschlerisisganangahimsaNo ratings yet
- Willmott Et Al-2008-BJOG An International Journal of Obstetrics & GynaecologyDocument3 pagesWillmott Et Al-2008-BJOG An International Journal of Obstetrics & GynaecologyganangahimsaNo ratings yet
- Investigation of Wall Shear Stress Distribution in Stented Coronary Artery Bifurcation V. DehlaghiDocument1 pageInvestigation of Wall Shear Stress Distribution in Stented Coronary Artery Bifurcation V. DehlaghiganangahimsaNo ratings yet
- Door To NeedleDocument40 pagesDoor To NeedleganangahimsaNo ratings yet
- ISF Content ListDocument4 pagesISF Content ListganangahimsaNo ratings yet
- Sanitation Saftey Midterm 2021Document5 pagesSanitation Saftey Midterm 2021Jah BinksNo ratings yet
- Certificate Nih Stroke ScaleDocument1 pageCertificate Nih Stroke Scaleapi-354841289No ratings yet
- Meniere's DiseaseDocument2 pagesMeniere's DiseaseNoelyn BaluyanNo ratings yet
- Munich DoctorsDocument6 pagesMunich DoctorsHafiz Muhammad LuqmanNo ratings yet
- 2024 Medical Examination FormDocument3 pages2024 Medical Examination Formmaryiordache2011No ratings yet
- 中国的药品安全监管状况 Status Quo Of Drug Supervision In China: we express the world 1Document40 pages中国的药品安全监管状况 Status Quo Of Drug Supervision In China: we express the world 1车笠No ratings yet
- 2020 Status Report As of August 31, 2021Document192 pages2020 Status Report As of August 31, 2021Jasper Kenneth PeraltaNo ratings yet
- Malady List - Mms Wiki - Jim Humble - Genesis II Church - Mmswiki IsDocument8 pagesMalady List - Mms Wiki - Jim Humble - Genesis II Church - Mmswiki Isapi-301431920No ratings yet
- Redacted Complaint Beaudoin V Baker FinalDocument25 pagesRedacted Complaint Beaudoin V Baker FinalKyle BeckerNo ratings yet
- Rapid Response TeamDocument4 pagesRapid Response TeamMichael SilvaNo ratings yet
- Equipment For Basic Life Support and Advanced Life Support Ground AmbulancesDocument8 pagesEquipment For Basic Life Support and Advanced Life Support Ground AmbulancesCesar MosqueraNo ratings yet
- A Brief History of Pharmacy 2015Document261 pagesA Brief History of Pharmacy 2015Najeeb100% (1)
- HTN BrochureDocument2 pagesHTN Brochureapi-400548889No ratings yet
- Recomendaciones Terapéuticas Del VII Consenso Clínico de SIBEN para La Encefalopatía Hipóxico-Isquémica NeonatalDocument17 pagesRecomendaciones Terapéuticas Del VII Consenso Clínico de SIBEN para La Encefalopatía Hipóxico-Isquémica NeonatalCarol HNo ratings yet
- Eliquis InfographicDocument7 pagesEliquis InfographicMichael RadaNo ratings yet
- Faculty of Graduate Studies, Mahidol University List of Recipients of 2021 Mahidol Postgraduate Scholarships (First Semester)Document6 pagesFaculty of Graduate Studies, Mahidol University List of Recipients of 2021 Mahidol Postgraduate Scholarships (First Semester)yayu latifahNo ratings yet
- Prevalence of Teenage Pregnancy Among Pregnant Mothers Presenting at Hoima Regional Referral Hospital During The Covid-19 Pandemic (2020 To 2021)Document8 pagesPrevalence of Teenage Pregnancy Among Pregnant Mothers Presenting at Hoima Regional Referral Hospital During The Covid-19 Pandemic (2020 To 2021)KIU PUBLICATION AND EXTENSIONNo ratings yet
- Placenta PreviaDocument3 pagesPlacenta PreviaReyniel Pablo ElumbaNo ratings yet
- Natural Benefits - EnglishDocument124 pagesNatural Benefits - EnglishNaveen SinghNo ratings yet
- MIMS Doctor November 2016 RGDocument36 pagesMIMS Doctor November 2016 RGDarmawan HariyantoNo ratings yet
- Fall 2020 - Week 3 GMDocument9 pagesFall 2020 - Week 3 GMapi-235454491No ratings yet
- Informed Consent On DocumentationDocument3 pagesInformed Consent On DocumentationanurajoneNo ratings yet
- AHM 250 Chapter 1Document9 pagesAHM 250 Chapter 1Paromita MukhopadhyayNo ratings yet
- Assessment Diagnosis Inference Planning Intervention Rationale Outcomes Subjective DataDocument2 pagesAssessment Diagnosis Inference Planning Intervention Rationale Outcomes Subjective DataJoan GuisicNo ratings yet
- CHN Lab - Quiz IMCIDocument3 pagesCHN Lab - Quiz IMCIKristine KimNo ratings yet
- 2 Antepartum Haemorrhage: Hannah Yeeles and Swati JhaDocument14 pages2 Antepartum Haemorrhage: Hannah Yeeles and Swati JhadeweNo ratings yet
- A Novel Approach To Correct Retracted NipplesDocument1 pageA Novel Approach To Correct Retracted NipplesEres TriasaNo ratings yet
- Wiac - Info PDF 771 Advances in Dga Interpretation PRDocument77 pagesWiac - Info PDF 771 Advances in Dga Interpretation PRChemist Ahmed FoudaNo ratings yet


































































































Download as pdf or txt
You might also like
- RAC Exam I Test Questions - Flash Cards Answer - KeyDocument101 pagesRAC Exam I Test Questions - Flash Cards Answer - KeyYesinta Diandra100% (4)
- Essentials For Nursing Practice 8th Edition Potter Test Bank DownloadDocument14 pagesEssentials For Nursing Practice 8th Edition Potter Test Bank DownloadJose Stepro100% (23)
- Consensus Guidelines On Point of Care Testing in Hospitals: I. BackgroundDocument4 pagesConsensus Guidelines On Point of Care Testing in Hospitals: I. BackgroundDocAxi Maximo Jr Axibal67% (3)
- Urinary Catheterisation and Catheter Care in Adults GuidelinesDocument37 pagesUrinary Catheterisation and Catheter Care in Adults GuidelinesAllend Reidene Viyar100% (1)
- Nurse Driven Protocols ArticleDocument7 pagesNurse Driven Protocols ArticlePaolo VegaNo ratings yet
- Groupd Ebp PresentationDocument38 pagesGroupd Ebp Presentationapi-384226081No ratings yet
- Bundles in Infection Prevention and SafetyDocument15 pagesBundles in Infection Prevention and SafetyInfectologia DiagnosticaNo ratings yet
- Catheter-Associated Urinary Tract Infection Care BundleDocument3 pagesCatheter-Associated Urinary Tract Infection Care BundleAnisaNo ratings yet
- Emergency Surgery FrameworkDocument36 pagesEmergency Surgery Frameworkhalosunyrtimr6No ratings yet
- Management of Patients With Long-Term Indwelling Urinary Catheters: A Review of GuidelinesDocument26 pagesManagement of Patients With Long-Term Indwelling Urinary Catheters: A Review of GuidelinesFaozan FikriNo ratings yet
- Appendix B. Urinary Catheterization - Sample Policy: AHRQ Safety Program For Reducing CAUTI in HospitalsDocument4 pagesAppendix B. Urinary Catheterization - Sample Policy: AHRQ Safety Program For Reducing CAUTI in HospitalsMhathea ArandidNo ratings yet
- TWOC Procedure GuidanceDocument6 pagesTWOC Procedure GuidanceKall VishNo ratings yet
- ISID InfectionGuide Chapter16Document15 pagesISID InfectionGuide Chapter16Nishtha Singh ChauhanNo ratings yet
- Uti Hicpac11 08Document40 pagesUti Hicpac11 08Koes Reenee EndroNo ratings yet
- Catheter-Associated Urinary Tract Infections and The Protocols For The Removal of Foley Catheters For Their PreventionDocument7 pagesCatheter-Associated Urinary Tract Infections and The Protocols For The Removal of Foley Catheters For Their PreventionCarlos I. RomeroNo ratings yet
- Admission and Discharge ProtocolDocument38 pagesAdmission and Discharge Protocolatinkut eteneshNo ratings yet
- Australia Isolation Rooms 2007Document48 pagesAustralia Isolation Rooms 2007jonathan_carretasNo ratings yet
- Essais Cliniques Decentralises VF enDocument15 pagesEssais Cliniques Decentralises VF enSchmoutNo ratings yet
- Eras Bps Final Nov2017 2Document24 pagesEras Bps Final Nov2017 2Wardah Fauziah El SofwanNo ratings yet
- Articulo en InglesDocument8 pagesArticulo en Inglesdante yonathan villegas lozanoNo ratings yet
- Catheter-Associated Urinary Tract InfectionsDocument20 pagesCatheter-Associated Urinary Tract Infectionsapi-315336673No ratings yet
- Guidelines For The Prevention of Catheterassociated Urinary Tract InfectionDocument54 pagesGuidelines For The Prevention of Catheterassociated Urinary Tract InfectioncateterdoblejotaNo ratings yet
- C0063 Specialty Guide - Respiratory and Coronavirus - v1 - 26 MarchDocument4 pagesC0063 Specialty Guide - Respiratory and Coronavirus - v1 - 26 MarchKevo VillagranNo ratings yet
- Qi Group Project - e C y TDocument10 pagesQi Group Project - e C y Tapi-302732994No ratings yet
- Roles of Bone Marrow Transplant Unit Nurses IncludesDocument10 pagesRoles of Bone Marrow Transplant Unit Nurses IncludesGleden UmayamNo ratings yet
- Admissions and Discharge: GuidelinesDocument26 pagesAdmissions and Discharge: GuidelinesIshaan TalrejaNo ratings yet
- Decontamination of Equipment Environment Policy 4.1Document29 pagesDecontamination of Equipment Environment Policy 4.1Rex Lagunzad FloresNo ratings yet
- Cathfoleyre 4859 FaDocument2 pagesCathfoleyre 4859 FaNeil OsborneNo ratings yet
- ACI Urology Bladder IrrigationDocument20 pagesACI Urology Bladder IrrigationOlivia BawaedaNo ratings yet
- IHFG Part B Renal Dialysis UnitDocument18 pagesIHFG Part B Renal Dialysis Unitmorton1472No ratings yet
- Adult Nasogastric Tube Insertion Procedure & Management PolicyDocument0 pagesAdult Nasogastric Tube Insertion Procedure & Management PolicyRubelyn Joy LazarteNo ratings yet
- CVC PolicyDocument15 pagesCVC Policyseaturtles505No ratings yet
- APH Surgical Service ProtocolDocument31 pagesAPH Surgical Service Protocolsami ketema50% (2)
- University of Colorado NICHE Practice Survey SummaryDocument48 pagesUniversity of Colorado NICHE Practice Survey Summarybocah_britpopNo ratings yet
- Pre Op 2010Document37 pagesPre Op 2010Tawona DhlakamaNo ratings yet
- Catheter Care: RCN Guidance For Health Care ProfessionalsDocument82 pagesCatheter Care: RCN Guidance For Health Care ProfessionalsSudin KumarNo ratings yet
- 2016 Toronto ERAS - STOMA - BPS - FINAL - 2018Document25 pages2016 Toronto ERAS - STOMA - BPS - FINAL - 2018durdane palabiyik yilmazNo ratings yet
- Strategies To Prevent Catheter Associated Urinary Tract Infections in Acute Care Hospitals 2022 UpdateDocument23 pagesStrategies To Prevent Catheter Associated Urinary Tract Infections in Acute Care Hospitals 2022 UpdateMega ArfiyantiNo ratings yet
- Guidanceclinicaltrials Covid19 en 1Document22 pagesGuidanceclinicaltrials Covid19 en 1VeraNo ratings yet
- Guidelines For Syringe Driver Management in Palliative Care: Developed byDocument57 pagesGuidelines For Syringe Driver Management in Palliative Care: Developed byFirmanNo ratings yet
- SOP-10-008 Suction July 20 2010 PDFDocument23 pagesSOP-10-008 Suction July 20 2010 PDFSalsabilla KimikoNo ratings yet
- Sop Number Title of SOP Author Consultation With StakeholdersDocument23 pagesSop Number Title of SOP Author Consultation With StakeholdersMr. BamsNo ratings yet
- Oncology Haematology 24 Hour TriageDocument28 pagesOncology Haematology 24 Hour TriageZaher MachadoNo ratings yet
- Get ResourceDocument28 pagesGet ResourceWalaa ElleithyNo ratings yet
- Guidanceclinicaltrials Covid19 Pres en PDFDocument65 pagesGuidanceclinicaltrials Covid19 Pres en PDFMarcM77No ratings yet
- انترودكشن عمليDocument13 pagesانترودكشن عمليRana KhaledNo ratings yet
- Qsen Project Urinary Catheter ComplicationsDocument18 pagesQsen Project Urinary Catheter Complicationsapi-316643564No ratings yet
- CAUTI Bundle of Care PDFDocument3 pagesCAUTI Bundle of Care PDFArvie PavinoNo ratings yet
- Waht-Inf-040 V2.1Document20 pagesWaht-Inf-040 V2.1Kheanry AlejandroNo ratings yet
- Selecting A Urinary Catheter and Drainage System: John RobinsonDocument6 pagesSelecting A Urinary Catheter and Drainage System: John RobinsonFrancisca BartschNo ratings yet
- Protocols For Day Care Anaesthesia: Ministry of Health MalaysiaDocument27 pagesProtocols For Day Care Anaesthesia: Ministry of Health MalaysiasitiNo ratings yet
- Advanced Infection Prevention and PDFDocument28 pagesAdvanced Infection Prevention and PDFWardah Fauziah El SofwanNo ratings yet
- Cauti Prevention - UpdatedDocument25 pagesCauti Prevention - Updatedapi-340518242No ratings yet
- IHOP - 9.13.25 - Time Out Universal Protocol For Invasive and Surgical ProceduresDocument3 pagesIHOP - 9.13.25 - Time Out Universal Protocol For Invasive and Surgical Proceduresmaxxer1985No ratings yet
- Cauti PreventionDocument25 pagesCauti Preventionapi-340511634No ratings yet
- Manual for Iv Therapy Procedures & Pain Management: Fourth EditionFrom EverandManual for Iv Therapy Procedures & Pain Management: Fourth EditionNo ratings yet
- TÉCNICAS DEL AUXILIAR DE ENFERMERÍA EN EL ÁREA DE QUIRÓFANOFrom EverandTÉCNICAS DEL AUXILIAR DE ENFERMERÍA EN EL ÁREA DE QUIRÓFANONo ratings yet
- Pustjens2020 Article GuidelinesForTheManagementOfMyDocument15 pagesPustjens2020 Article GuidelinesForTheManagementOfMyganangahimsaNo ratings yet
- Abstracts: Case Reports: Indonesian Journal of CardiologyDocument63 pagesAbstracts: Case Reports: Indonesian Journal of CardiologyganangahimsaNo ratings yet
- Differential Diagnosis of Cardiogenic Syncope and Seizure DisordersDocument6 pagesDifferential Diagnosis of Cardiogenic Syncope and Seizure DisordersganangahimsaNo ratings yet
- Comparative Safety of Sulfonylurea and Metformin Monotherapy On The Risk of Heart Failure: A Cohort StudyDocument29 pagesComparative Safety of Sulfonylurea and Metformin Monotherapy On The Risk of Heart Failure: A Cohort StudyganangahimsaNo ratings yet
- Triatmo Budiyuwono SPJP (K), FIHA, FAPSICDocument40 pagesTriatmo Budiyuwono SPJP (K), FIHA, FAPSICganangahimsaNo ratings yet
- Regulatory T Cell I AtheroschlerisisDocument13 pagesRegulatory T Cell I AtheroschlerisisganangahimsaNo ratings yet
- Willmott Et Al-2008-BJOG An International Journal of Obstetrics & GynaecologyDocument3 pagesWillmott Et Al-2008-BJOG An International Journal of Obstetrics & GynaecologyganangahimsaNo ratings yet
- Investigation of Wall Shear Stress Distribution in Stented Coronary Artery Bifurcation V. DehlaghiDocument1 pageInvestigation of Wall Shear Stress Distribution in Stented Coronary Artery Bifurcation V. DehlaghiganangahimsaNo ratings yet
- Door To NeedleDocument40 pagesDoor To NeedleganangahimsaNo ratings yet
- ISF Content ListDocument4 pagesISF Content ListganangahimsaNo ratings yet
- Sanitation Saftey Midterm 2021Document5 pagesSanitation Saftey Midterm 2021Jah BinksNo ratings yet
- Certificate Nih Stroke ScaleDocument1 pageCertificate Nih Stroke Scaleapi-354841289No ratings yet
- Meniere's DiseaseDocument2 pagesMeniere's DiseaseNoelyn BaluyanNo ratings yet
- Munich DoctorsDocument6 pagesMunich DoctorsHafiz Muhammad LuqmanNo ratings yet
- 2024 Medical Examination FormDocument3 pages2024 Medical Examination Formmaryiordache2011No ratings yet
- 中国的药品安全监管状况 Status Quo Of Drug Supervision In China: we express the world 1Document40 pages中国的药品安全监管状况 Status Quo Of Drug Supervision In China: we express the world 1车笠No ratings yet
- 2020 Status Report As of August 31, 2021Document192 pages2020 Status Report As of August 31, 2021Jasper Kenneth PeraltaNo ratings yet
- Malady List - Mms Wiki - Jim Humble - Genesis II Church - Mmswiki IsDocument8 pagesMalady List - Mms Wiki - Jim Humble - Genesis II Church - Mmswiki Isapi-301431920No ratings yet
- Redacted Complaint Beaudoin V Baker FinalDocument25 pagesRedacted Complaint Beaudoin V Baker FinalKyle BeckerNo ratings yet
- Rapid Response TeamDocument4 pagesRapid Response TeamMichael SilvaNo ratings yet
- Equipment For Basic Life Support and Advanced Life Support Ground AmbulancesDocument8 pagesEquipment For Basic Life Support and Advanced Life Support Ground AmbulancesCesar MosqueraNo ratings yet
- A Brief History of Pharmacy 2015Document261 pagesA Brief History of Pharmacy 2015Najeeb100% (1)
- HTN BrochureDocument2 pagesHTN Brochureapi-400548889No ratings yet
- Recomendaciones Terapéuticas Del VII Consenso Clínico de SIBEN para La Encefalopatía Hipóxico-Isquémica NeonatalDocument17 pagesRecomendaciones Terapéuticas Del VII Consenso Clínico de SIBEN para La Encefalopatía Hipóxico-Isquémica NeonatalCarol HNo ratings yet
- Eliquis InfographicDocument7 pagesEliquis InfographicMichael RadaNo ratings yet
- Faculty of Graduate Studies, Mahidol University List of Recipients of 2021 Mahidol Postgraduate Scholarships (First Semester)Document6 pagesFaculty of Graduate Studies, Mahidol University List of Recipients of 2021 Mahidol Postgraduate Scholarships (First Semester)yayu latifahNo ratings yet
- Prevalence of Teenage Pregnancy Among Pregnant Mothers Presenting at Hoima Regional Referral Hospital During The Covid-19 Pandemic (2020 To 2021)Document8 pagesPrevalence of Teenage Pregnancy Among Pregnant Mothers Presenting at Hoima Regional Referral Hospital During The Covid-19 Pandemic (2020 To 2021)KIU PUBLICATION AND EXTENSIONNo ratings yet
- Placenta PreviaDocument3 pagesPlacenta PreviaReyniel Pablo ElumbaNo ratings yet
- Natural Benefits - EnglishDocument124 pagesNatural Benefits - EnglishNaveen SinghNo ratings yet
- MIMS Doctor November 2016 RGDocument36 pagesMIMS Doctor November 2016 RGDarmawan HariyantoNo ratings yet
- Fall 2020 - Week 3 GMDocument9 pagesFall 2020 - Week 3 GMapi-235454491No ratings yet
- Informed Consent On DocumentationDocument3 pagesInformed Consent On DocumentationanurajoneNo ratings yet
- AHM 250 Chapter 1Document9 pagesAHM 250 Chapter 1Paromita MukhopadhyayNo ratings yet
- Assessment Diagnosis Inference Planning Intervention Rationale Outcomes Subjective DataDocument2 pagesAssessment Diagnosis Inference Planning Intervention Rationale Outcomes Subjective DataJoan GuisicNo ratings yet
- CHN Lab - Quiz IMCIDocument3 pagesCHN Lab - Quiz IMCIKristine KimNo ratings yet
- 2 Antepartum Haemorrhage: Hannah Yeeles and Swati JhaDocument14 pages2 Antepartum Haemorrhage: Hannah Yeeles and Swati JhadeweNo ratings yet
- A Novel Approach To Correct Retracted NipplesDocument1 pageA Novel Approach To Correct Retracted NipplesEres TriasaNo ratings yet
- Wiac - Info PDF 771 Advances in Dga Interpretation PRDocument77 pagesWiac - Info PDF 771 Advances in Dga Interpretation PRChemist Ahmed FoudaNo ratings yet