
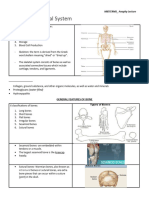
The Musculoskeletal System
The Musculoskeletal System
You might also like
- Addiction Treatment: A Strengths PerspectiveDocument2 pagesAddiction Treatment: A Strengths PerspectiveKatherine van Wormer50% (4)
- Anaphy C7 Oral Rec.Document3 pagesAnaphy C7 Oral Rec.Katrina ParbaNo ratings yet
- Musculoskeltal SystemDocument18 pagesMusculoskeltal Systemhy7tnNo ratings yet
- Formation: Blood Calcium Level - Calcium HydroxyapatiteDocument13 pagesFormation: Blood Calcium Level - Calcium HydroxyapatiteClarissa IsuriñaNo ratings yet
- Lec 1516 Bone Tissue and Skeletal SystemDocument28 pagesLec 1516 Bone Tissue and Skeletal SystemonegaonnweNo ratings yet
- Functional Anatomy and Physiology 1Document6 pagesFunctional Anatomy and Physiology 1AtiqahNo ratings yet
- Kalsifikasi, Deposisi Dan Resorpsi TulangDocument40 pagesKalsifikasi, Deposisi Dan Resorpsi TulangrifkaNo ratings yet
- Calcium Homeostasis and Osteoporosis - McMaster Pathophysiology ReviewDocument8 pagesCalcium Homeostasis and Osteoporosis - McMaster Pathophysiology ReviewEzayu AzeraNo ratings yet
- Bone and Mineral Metabolism in Health and DiseaseDocument14 pagesBone and Mineral Metabolism in Health and Diseasebiniam MesfinNo ratings yet
- Bone Metabolism: German VersionDocument17 pagesBone Metabolism: German VersionDapot SianiparNo ratings yet
- Exam A-3Document11 pagesExam A-3yapues87No ratings yet
- Bone and Cartilage PDFDocument50 pagesBone and Cartilage PDFalviraNo ratings yet
- 7 CalciumDocument83 pages7 Calciumtmqt2fbnzgNo ratings yet
- Bone Basic Science: Presenter: DR Nshimiyimana Alexis Orthopedic Resident-UrDocument36 pagesBone Basic Science: Presenter: DR Nshimiyimana Alexis Orthopedic Resident-UrNshimiyimana AlexisNo ratings yet
- 511-525chapter 6-8 (1) An Introduction To The Skeletal SystemDocument6 pages511-525chapter 6-8 (1) An Introduction To The Skeletal Systemtomorrow.today.yesterday .yesterdayNo ratings yet
- Seminar On Bone and CalciumDocument4 pagesSeminar On Bone and Calciumtshireletso “TROY” nkunaNo ratings yet
- Alveolar Bone FFDocument105 pagesAlveolar Bone FFshashi kant chaudharyNo ratings yet
- Chap 6 AnaphyDocument8 pagesChap 6 AnaphyNicholle VelosoNo ratings yet
- Ch. 10 and 6Document25 pagesCh. 10 and 6Bammary88909No ratings yet
- Physiologic Processes in The Skeletal SystemDocument6 pagesPhysiologic Processes in The Skeletal SystemAry Romeo ShakespeareNo ratings yet
- Anatomy & Physiology: Skeletal SystemDocument20 pagesAnatomy & Physiology: Skeletal SystemWilbert Antonino CabanbanNo ratings yet
- Human Anatomy 4th Edition Saladin Solutions Manual 1Document36 pagesHuman Anatomy 4th Edition Saladin Solutions Manual 1donnawugnwsjrzcxt100% (28)
- Human Anatomy 4Th Edition Saladin Solutions Manual Full Chapter PDFDocument27 pagesHuman Anatomy 4Th Edition Saladin Solutions Manual Full Chapter PDFdora.ivy892100% (22)
- Bone ResorptionDocument10 pagesBone ResorptionVibhor PradhanNo ratings yet
- COMPRE2Document13 pagesCOMPRE2Rodrigo SeriozaNo ratings yet
- 6.the Skeletal System Bone TissueDocument25 pages6.the Skeletal System Bone TissueKojo Yeboah EnchillNo ratings yet
- SKELETAL SYSTEM ReviewerDocument7 pagesSKELETAL SYSTEM ReviewerKrize Colene dela CruzNo ratings yet
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocument19 pagesWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsJade LolongNo ratings yet
- Bone Physiology 2Document27 pagesBone Physiology 2Nzau MuangeNo ratings yet
- MatthewVaracalloMD PhysiologyBoneDocument5 pagesMatthewVaracalloMD PhysiologyBonetulipaNo ratings yet
- Bone Formation: Hypothalamic Hormone, CRH, and The Pituitary Hormone, ACTHDocument3 pagesBone Formation: Hypothalamic Hormone, CRH, and The Pituitary Hormone, ACTHSimon AvilaNo ratings yet
- Bone Ash Estimation of Content of Bone Ash Project Submitted by PrashanthDocument3 pagesBone Ash Estimation of Content of Bone Ash Project Submitted by PrashanthHarsh Kumar0% (3)
- Alad Bihag Hizon Medicine Case StudyDocument103 pagesAlad Bihag Hizon Medicine Case StudyDan HizonNo ratings yet
- Chapter 3Document12 pagesChapter 3Deolita BadiangNo ratings yet
- Bones: A Hard SubjectDocument16 pagesBones: A Hard SubjectMaria Dini AdmiratiNo ratings yet
- Chemistry Project On Estimation of Content of Bone AshDocument18 pagesChemistry Project On Estimation of Content of Bone AshKim TaesiNo ratings yet
- Drugs Bone DisordersDocument38 pagesDrugs Bone Disordersalizwaxabanisa8No ratings yet
- Functions of The Musculoskeletal SystemDocument9 pagesFunctions of The Musculoskeletal SystemLinda XueNo ratings yet
- Department of Periodontics and Implantology: Calcium MetabolismDocument63 pagesDepartment of Periodontics and Implantology: Calcium Metabolismrasagna reddy100% (1)
- Bone Is A MineralizedDocument2 pagesBone Is A MineralizedZen Firhan ShahabNo ratings yet
- Human Anatomy 5th Edition Saladin Solutions ManualDocument7 pagesHuman Anatomy 5th Edition Saladin Solutions Manualjillhenrysetcjnzrfp100% (26)
- 7 - BoneDocument36 pages7 - BoneKhdhir M. SalemNo ratings yet
- Human Anatomy 5Th Edition Saladin Solutions Manual Full Chapter PDFDocument28 pagesHuman Anatomy 5Th Edition Saladin Solutions Manual Full Chapter PDFJenniferWhitebctr100% (12)
- Alveolar Bone: and It's Associated PathologiesDocument7 pagesAlveolar Bone: and It's Associated Pathologiesمحمد العراقيNo ratings yet
- Chemistry Project On Estimation of Content of Bone AshDocument13 pagesChemistry Project On Estimation of Content of Bone AshShlok Sah50% (2)
- Topic 5. Bone Microscopic Anatomy and Devt 1Document24 pagesTopic 5. Bone Microscopic Anatomy and Devt 1Janine Jerica JontilanoNo ratings yet
- The Main Functions of BonesDocument9 pagesThe Main Functions of BonesabbaslafeNo ratings yet
- Proteoglycans, Whose Main Glycosaminoglycans Are Chondroitin-4-Sulfate and Chondroitin-6Document14 pagesProteoglycans, Whose Main Glycosaminoglycans Are Chondroitin-4-Sulfate and Chondroitin-6Joseph Enoch ElisanNo ratings yet
- Lec 3 2010 02 6Document8 pagesLec 3 2010 02 6Ras WhoknowsmeNo ratings yet
- Intro Tothe Function of Parathyroid Gland, ConciseDocument34 pagesIntro Tothe Function of Parathyroid Gland, Conciseinka.elseNo ratings yet
- Orthopedic NursingDocument237 pagesOrthopedic Nursingɹǝʍdןnos100% (24)
- Kenkre Bassett 2018 The Bone Remodelling CycleDocument20 pagesKenkre Bassett 2018 The Bone Remodelling Cyclealealer2708No ratings yet
- Bone As A Living Dynamic TissueDocument14 pagesBone As A Living Dynamic TissueSuraj_Subedi100% (6)
- Agents That Affect Bone Mineral Homeostasis: Department of PharmacologyDocument44 pagesAgents That Affect Bone Mineral Homeostasis: Department of Pharmacologymichaelcyl100% (1)
- Physiology of BoneDocument32 pagesPhysiology of BoneAnandhu GNo ratings yet
- Ch07 - EOC - Skeletal SystemDocument4 pagesCh07 - EOC - Skeletal SystemGaveen CoatesNo ratings yet
- Bone: Biology, Harvesting, and Grafting for Dental Implants, 2nd EditionFrom EverandBone: Biology, Harvesting, and Grafting for Dental Implants, 2nd EditionNo ratings yet
- Renal Reflections: Exploring the Marvels of Nephrology: The Intricate Ballet of Kidney Functions UnveiledFrom EverandRenal Reflections: Exploring the Marvels of Nephrology: The Intricate Ballet of Kidney Functions UnveiledNo ratings yet
- Advanced farriery knowledge: A study guide and AWCF theory course companionFrom EverandAdvanced farriery knowledge: A study guide and AWCF theory course companionNo ratings yet
- Rangkuman Week 5 (PBL) - OsteomyelitisDocument9 pagesRangkuman Week 5 (PBL) - OsteomyelitisMaria Dini AdmiratiNo ratings yet
- Rangkuman Week 3 (PBL) - RADocument27 pagesRangkuman Week 3 (PBL) - RAMaria Dini AdmiratiNo ratings yet
- Week 1 HumanAnat&Fisio - 6 Agustus 2012Document17 pagesWeek 1 HumanAnat&Fisio - 6 Agustus 2012Maria Dini AdmiratiNo ratings yet
- Week 3 JointInflammatoryDisease - 27 Agustus 2012Document19 pagesWeek 3 JointInflammatoryDisease - 27 Agustus 2012Maria Dini AdmiratiNo ratings yet
- Week 1 BlockMuscle - 6 Agustus 2012Document21 pagesWeek 1 BlockMuscle - 6 Agustus 2012Maria Dini AdmiratiNo ratings yet
- Week 4 MetabolicBoneDisease - 3 September 2012week 4 MetabolicBoneDisease - 3 September 2012Document16 pagesWeek 4 MetabolicBoneDisease - 3 September 2012week 4 MetabolicBoneDisease - 3 September 2012Maria Dini AdmiratiNo ratings yet
- Week 4 BackBoneAnatomy - 3 September 2012Document20 pagesWeek 4 BackBoneAnatomy - 3 September 2012Maria Dini AdmiratiNo ratings yet
- Bones: A Hard SubjectDocument16 pagesBones: A Hard SubjectMaria Dini AdmiratiNo ratings yet
- Week 2 Blpressoureoduph - 20 Februari 2012week 2 Blpressoureoduph - 20 Februari 2012Document43 pagesWeek 2 Blpressoureoduph - 20 Februari 2012week 2 Blpressoureoduph - 20 Februari 2012Maria Dini AdmiratiNo ratings yet
- Week 4 Embryology Development of Gastrointestinal: DR Marselina TanDocument29 pagesWeek 4 Embryology Development of Gastrointestinal: DR Marselina TanMaria Dini AdmiratiNo ratings yet
- Heat Related Illnesses: Erwin Mulyawan, DR, Span, DpbaDocument42 pagesHeat Related Illnesses: Erwin Mulyawan, DR, Span, DpbaMaria Dini AdmiratiNo ratings yet
- Is An Irregular Shape Cylinder With Narrow Opening Superiorly and A Large Inferiorly OpeningDocument27 pagesIs An Irregular Shape Cylinder With Narrow Opening Superiorly and A Large Inferiorly OpeningMaria Dini AdmiratiNo ratings yet
- Communication Between Nerve Cells.: V. Sutarmo SetiadjiDocument35 pagesCommunication Between Nerve Cells.: V. Sutarmo SetiadjiMaria Dini AdmiratiNo ratings yet
- Laboratory Logistics HandbookDocument96 pagesLaboratory Logistics HandbookMohd Fahmi MastukiNo ratings yet
- POLYSEED Application Procedure 3.15Document2 pagesPOLYSEED Application Procedure 3.15ALVARO ENRIQUE CANTILLO GUZMANNo ratings yet
- Chronic Pain and Road MappingDocument3 pagesChronic Pain and Road MappingkasiaNo ratings yet
- Why Antibiotics Should Not Be Overused. Write A Short Note?Document4 pagesWhy Antibiotics Should Not Be Overused. Write A Short Note?Danger TigerNo ratings yet
- Cauti CDC 2018Document17 pagesCauti CDC 2018NasikhatulNo ratings yet
- FDAR ChartingDocument50 pagesFDAR ChartingNathaniel PulidoNo ratings yet
- Womens - Era July 2017Document148 pagesWomens - Era July 2017taruniNo ratings yet
- Q A Random - 16Document8 pagesQ A Random - 16ja100% (1)
- Traditional Medicine & Herbal TechnologyDocument39 pagesTraditional Medicine & Herbal TechnologyDivyam14No ratings yet
- Ilness and BiomagnetismDocument3 pagesIlness and BiomagnetismSilvia Arias100% (2)
- Oklahoma Commission On Opioid Abuse Final ReportDocument12 pagesOklahoma Commission On Opioid Abuse Final ReportOKCFOXNo ratings yet
- REBTDocument18 pagesREBTGayathree ChandranNo ratings yet
- Cognitive Behaviour Therapy For Depression in Young People Manual For TherapistsDocument120 pagesCognitive Behaviour Therapy For Depression in Young People Manual For TherapistsSundar PrabhuNo ratings yet
- Byproducts From Cassava ProcessingDocument29 pagesByproducts From Cassava ProcessingasokmithraNo ratings yet
- UPSC Medical ScienceDocument7 pagesUPSC Medical ScienceAbhishek JoshiNo ratings yet
- Herbal CosmeticsDocument40 pagesHerbal CosmeticsBiren Shah100% (1)
- PDF DipiroDocument16 pagesPDF DipiroYolandaFandraIINo ratings yet
- Swedish MassageDocument22 pagesSwedish Massagealejandro jean100% (3)
- Swollen Neck Lymph Nodes - Causes - Better MedicineDocument6 pagesSwollen Neck Lymph Nodes - Causes - Better MedicineDanao ErickNo ratings yet
- Starch Industry in IndiaDocument3 pagesStarch Industry in Indiabanapte59No ratings yet
- Leisure Awareness ActivitiesDocument9 pagesLeisure Awareness Activitiesapi-301398957No ratings yet
- The Clinical Management of Awake BruxismDocument30 pagesThe Clinical Management of Awake BruxismSahana RangarajanNo ratings yet
- SPDX Week 8 - Perfusion TechnologyDocument2 pagesSPDX Week 8 - Perfusion TechnologyerikajoydmrmtNo ratings yet
- Koppenaal2020 Article EffectivenessAndCost-effectiveDocument13 pagesKoppenaal2020 Article EffectivenessAndCost-effectivePaulomds1991No ratings yet
- 1-Legal Med Notes PDFDocument19 pages1-Legal Med Notes PDFFrenza Joy FresnidoNo ratings yet
- Super fi cial roughness on composite surface, composite enamel and composite dentin junctions after different fi nishing and polishing procedures. Part I: roughness after treatments with tungsten carbide vs diamond bursDocument20 pagesSuper fi cial roughness on composite surface, composite enamel and composite dentin junctions after different fi nishing and polishing procedures. Part I: roughness after treatments with tungsten carbide vs diamond bursCinthyaNavarroNo ratings yet
- ATI Module - Ethical Principles For Mental HealthDocument6 pagesATI Module - Ethical Principles For Mental HealthChelsea HebertNo ratings yet
- Cholelithiasis When They Are in The Bile CholedocolithiasisDocument15 pagesCholelithiasis When They Are in The Bile Choledocolithiasishisabumohamed100% (1)
- Cai Songfang Wujishi Breathing Exercises Medicine Health Publishing Co. 1994Document119 pagesCai Songfang Wujishi Breathing Exercises Medicine Health Publishing Co. 1994Amlen Singha100% (2)




































































































Download as pdf or txt
You might also like
- Addiction Treatment: A Strengths PerspectiveDocument2 pagesAddiction Treatment: A Strengths PerspectiveKatherine van Wormer50% (4)
- Anaphy C7 Oral Rec.Document3 pagesAnaphy C7 Oral Rec.Katrina ParbaNo ratings yet
- Musculoskeltal SystemDocument18 pagesMusculoskeltal Systemhy7tnNo ratings yet
- Formation: Blood Calcium Level - Calcium HydroxyapatiteDocument13 pagesFormation: Blood Calcium Level - Calcium HydroxyapatiteClarissa IsuriñaNo ratings yet
- Lec 1516 Bone Tissue and Skeletal SystemDocument28 pagesLec 1516 Bone Tissue and Skeletal SystemonegaonnweNo ratings yet
- Functional Anatomy and Physiology 1Document6 pagesFunctional Anatomy and Physiology 1AtiqahNo ratings yet
- Kalsifikasi, Deposisi Dan Resorpsi TulangDocument40 pagesKalsifikasi, Deposisi Dan Resorpsi TulangrifkaNo ratings yet
- Calcium Homeostasis and Osteoporosis - McMaster Pathophysiology ReviewDocument8 pagesCalcium Homeostasis and Osteoporosis - McMaster Pathophysiology ReviewEzayu AzeraNo ratings yet
- Bone and Mineral Metabolism in Health and DiseaseDocument14 pagesBone and Mineral Metabolism in Health and Diseasebiniam MesfinNo ratings yet
- Bone Metabolism: German VersionDocument17 pagesBone Metabolism: German VersionDapot SianiparNo ratings yet
- Exam A-3Document11 pagesExam A-3yapues87No ratings yet
- Bone and Cartilage PDFDocument50 pagesBone and Cartilage PDFalviraNo ratings yet
- 7 CalciumDocument83 pages7 Calciumtmqt2fbnzgNo ratings yet
- Bone Basic Science: Presenter: DR Nshimiyimana Alexis Orthopedic Resident-UrDocument36 pagesBone Basic Science: Presenter: DR Nshimiyimana Alexis Orthopedic Resident-UrNshimiyimana AlexisNo ratings yet
- 511-525chapter 6-8 (1) An Introduction To The Skeletal SystemDocument6 pages511-525chapter 6-8 (1) An Introduction To The Skeletal Systemtomorrow.today.yesterday .yesterdayNo ratings yet
- Seminar On Bone and CalciumDocument4 pagesSeminar On Bone and Calciumtshireletso “TROY” nkunaNo ratings yet
- Alveolar Bone FFDocument105 pagesAlveolar Bone FFshashi kant chaudharyNo ratings yet
- Chap 6 AnaphyDocument8 pagesChap 6 AnaphyNicholle VelosoNo ratings yet
- Ch. 10 and 6Document25 pagesCh. 10 and 6Bammary88909No ratings yet
- Physiologic Processes in The Skeletal SystemDocument6 pagesPhysiologic Processes in The Skeletal SystemAry Romeo ShakespeareNo ratings yet
- Anatomy & Physiology: Skeletal SystemDocument20 pagesAnatomy & Physiology: Skeletal SystemWilbert Antonino CabanbanNo ratings yet
- Human Anatomy 4th Edition Saladin Solutions Manual 1Document36 pagesHuman Anatomy 4th Edition Saladin Solutions Manual 1donnawugnwsjrzcxt100% (28)
- Human Anatomy 4Th Edition Saladin Solutions Manual Full Chapter PDFDocument27 pagesHuman Anatomy 4Th Edition Saladin Solutions Manual Full Chapter PDFdora.ivy892100% (22)
- Bone ResorptionDocument10 pagesBone ResorptionVibhor PradhanNo ratings yet
- COMPRE2Document13 pagesCOMPRE2Rodrigo SeriozaNo ratings yet
- 6.the Skeletal System Bone TissueDocument25 pages6.the Skeletal System Bone TissueKojo Yeboah EnchillNo ratings yet
- SKELETAL SYSTEM ReviewerDocument7 pagesSKELETAL SYSTEM ReviewerKrize Colene dela CruzNo ratings yet
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocument19 pagesWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsJade LolongNo ratings yet
- Bone Physiology 2Document27 pagesBone Physiology 2Nzau MuangeNo ratings yet
- MatthewVaracalloMD PhysiologyBoneDocument5 pagesMatthewVaracalloMD PhysiologyBonetulipaNo ratings yet
- Bone Formation: Hypothalamic Hormone, CRH, and The Pituitary Hormone, ACTHDocument3 pagesBone Formation: Hypothalamic Hormone, CRH, and The Pituitary Hormone, ACTHSimon AvilaNo ratings yet
- Bone Ash Estimation of Content of Bone Ash Project Submitted by PrashanthDocument3 pagesBone Ash Estimation of Content of Bone Ash Project Submitted by PrashanthHarsh Kumar0% (3)
- Alad Bihag Hizon Medicine Case StudyDocument103 pagesAlad Bihag Hizon Medicine Case StudyDan HizonNo ratings yet
- Chapter 3Document12 pagesChapter 3Deolita BadiangNo ratings yet
- Bones: A Hard SubjectDocument16 pagesBones: A Hard SubjectMaria Dini AdmiratiNo ratings yet
- Chemistry Project On Estimation of Content of Bone AshDocument18 pagesChemistry Project On Estimation of Content of Bone AshKim TaesiNo ratings yet
- Drugs Bone DisordersDocument38 pagesDrugs Bone Disordersalizwaxabanisa8No ratings yet
- Functions of The Musculoskeletal SystemDocument9 pagesFunctions of The Musculoskeletal SystemLinda XueNo ratings yet
- Department of Periodontics and Implantology: Calcium MetabolismDocument63 pagesDepartment of Periodontics and Implantology: Calcium Metabolismrasagna reddy100% (1)
- Bone Is A MineralizedDocument2 pagesBone Is A MineralizedZen Firhan ShahabNo ratings yet
- Human Anatomy 5th Edition Saladin Solutions ManualDocument7 pagesHuman Anatomy 5th Edition Saladin Solutions Manualjillhenrysetcjnzrfp100% (26)
- 7 - BoneDocument36 pages7 - BoneKhdhir M. SalemNo ratings yet
- Human Anatomy 5Th Edition Saladin Solutions Manual Full Chapter PDFDocument28 pagesHuman Anatomy 5Th Edition Saladin Solutions Manual Full Chapter PDFJenniferWhitebctr100% (12)
- Alveolar Bone: and It's Associated PathologiesDocument7 pagesAlveolar Bone: and It's Associated Pathologiesمحمد العراقيNo ratings yet
- Chemistry Project On Estimation of Content of Bone AshDocument13 pagesChemistry Project On Estimation of Content of Bone AshShlok Sah50% (2)
- Topic 5. Bone Microscopic Anatomy and Devt 1Document24 pagesTopic 5. Bone Microscopic Anatomy and Devt 1Janine Jerica JontilanoNo ratings yet
- The Main Functions of BonesDocument9 pagesThe Main Functions of BonesabbaslafeNo ratings yet
- Proteoglycans, Whose Main Glycosaminoglycans Are Chondroitin-4-Sulfate and Chondroitin-6Document14 pagesProteoglycans, Whose Main Glycosaminoglycans Are Chondroitin-4-Sulfate and Chondroitin-6Joseph Enoch ElisanNo ratings yet
- Lec 3 2010 02 6Document8 pagesLec 3 2010 02 6Ras WhoknowsmeNo ratings yet
- Intro Tothe Function of Parathyroid Gland, ConciseDocument34 pagesIntro Tothe Function of Parathyroid Gland, Conciseinka.elseNo ratings yet
- Orthopedic NursingDocument237 pagesOrthopedic Nursingɹǝʍdןnos100% (24)
- Kenkre Bassett 2018 The Bone Remodelling CycleDocument20 pagesKenkre Bassett 2018 The Bone Remodelling Cyclealealer2708No ratings yet
- Bone As A Living Dynamic TissueDocument14 pagesBone As A Living Dynamic TissueSuraj_Subedi100% (6)
- Agents That Affect Bone Mineral Homeostasis: Department of PharmacologyDocument44 pagesAgents That Affect Bone Mineral Homeostasis: Department of Pharmacologymichaelcyl100% (1)
- Physiology of BoneDocument32 pagesPhysiology of BoneAnandhu GNo ratings yet
- Ch07 - EOC - Skeletal SystemDocument4 pagesCh07 - EOC - Skeletal SystemGaveen CoatesNo ratings yet
- Bone: Biology, Harvesting, and Grafting for Dental Implants, 2nd EditionFrom EverandBone: Biology, Harvesting, and Grafting for Dental Implants, 2nd EditionNo ratings yet
- Renal Reflections: Exploring the Marvels of Nephrology: The Intricate Ballet of Kidney Functions UnveiledFrom EverandRenal Reflections: Exploring the Marvels of Nephrology: The Intricate Ballet of Kidney Functions UnveiledNo ratings yet
- Advanced farriery knowledge: A study guide and AWCF theory course companionFrom EverandAdvanced farriery knowledge: A study guide and AWCF theory course companionNo ratings yet
- Rangkuman Week 5 (PBL) - OsteomyelitisDocument9 pagesRangkuman Week 5 (PBL) - OsteomyelitisMaria Dini AdmiratiNo ratings yet
- Rangkuman Week 3 (PBL) - RADocument27 pagesRangkuman Week 3 (PBL) - RAMaria Dini AdmiratiNo ratings yet
- Week 1 HumanAnat&Fisio - 6 Agustus 2012Document17 pagesWeek 1 HumanAnat&Fisio - 6 Agustus 2012Maria Dini AdmiratiNo ratings yet
- Week 3 JointInflammatoryDisease - 27 Agustus 2012Document19 pagesWeek 3 JointInflammatoryDisease - 27 Agustus 2012Maria Dini AdmiratiNo ratings yet
- Week 1 BlockMuscle - 6 Agustus 2012Document21 pagesWeek 1 BlockMuscle - 6 Agustus 2012Maria Dini AdmiratiNo ratings yet
- Week 4 MetabolicBoneDisease - 3 September 2012week 4 MetabolicBoneDisease - 3 September 2012Document16 pagesWeek 4 MetabolicBoneDisease - 3 September 2012week 4 MetabolicBoneDisease - 3 September 2012Maria Dini AdmiratiNo ratings yet
- Week 4 BackBoneAnatomy - 3 September 2012Document20 pagesWeek 4 BackBoneAnatomy - 3 September 2012Maria Dini AdmiratiNo ratings yet
- Bones: A Hard SubjectDocument16 pagesBones: A Hard SubjectMaria Dini AdmiratiNo ratings yet
- Week 2 Blpressoureoduph - 20 Februari 2012week 2 Blpressoureoduph - 20 Februari 2012Document43 pagesWeek 2 Blpressoureoduph - 20 Februari 2012week 2 Blpressoureoduph - 20 Februari 2012Maria Dini AdmiratiNo ratings yet
- Week 4 Embryology Development of Gastrointestinal: DR Marselina TanDocument29 pagesWeek 4 Embryology Development of Gastrointestinal: DR Marselina TanMaria Dini AdmiratiNo ratings yet
- Heat Related Illnesses: Erwin Mulyawan, DR, Span, DpbaDocument42 pagesHeat Related Illnesses: Erwin Mulyawan, DR, Span, DpbaMaria Dini AdmiratiNo ratings yet
- Is An Irregular Shape Cylinder With Narrow Opening Superiorly and A Large Inferiorly OpeningDocument27 pagesIs An Irregular Shape Cylinder With Narrow Opening Superiorly and A Large Inferiorly OpeningMaria Dini AdmiratiNo ratings yet
- Communication Between Nerve Cells.: V. Sutarmo SetiadjiDocument35 pagesCommunication Between Nerve Cells.: V. Sutarmo SetiadjiMaria Dini AdmiratiNo ratings yet
- Laboratory Logistics HandbookDocument96 pagesLaboratory Logistics HandbookMohd Fahmi MastukiNo ratings yet
- POLYSEED Application Procedure 3.15Document2 pagesPOLYSEED Application Procedure 3.15ALVARO ENRIQUE CANTILLO GUZMANNo ratings yet
- Chronic Pain and Road MappingDocument3 pagesChronic Pain and Road MappingkasiaNo ratings yet
- Why Antibiotics Should Not Be Overused. Write A Short Note?Document4 pagesWhy Antibiotics Should Not Be Overused. Write A Short Note?Danger TigerNo ratings yet
- Cauti CDC 2018Document17 pagesCauti CDC 2018NasikhatulNo ratings yet
- FDAR ChartingDocument50 pagesFDAR ChartingNathaniel PulidoNo ratings yet
- Womens - Era July 2017Document148 pagesWomens - Era July 2017taruniNo ratings yet
- Q A Random - 16Document8 pagesQ A Random - 16ja100% (1)
- Traditional Medicine & Herbal TechnologyDocument39 pagesTraditional Medicine & Herbal TechnologyDivyam14No ratings yet
- Ilness and BiomagnetismDocument3 pagesIlness and BiomagnetismSilvia Arias100% (2)
- Oklahoma Commission On Opioid Abuse Final ReportDocument12 pagesOklahoma Commission On Opioid Abuse Final ReportOKCFOXNo ratings yet
- REBTDocument18 pagesREBTGayathree ChandranNo ratings yet
- Cognitive Behaviour Therapy For Depression in Young People Manual For TherapistsDocument120 pagesCognitive Behaviour Therapy For Depression in Young People Manual For TherapistsSundar PrabhuNo ratings yet
- Byproducts From Cassava ProcessingDocument29 pagesByproducts From Cassava ProcessingasokmithraNo ratings yet
- UPSC Medical ScienceDocument7 pagesUPSC Medical ScienceAbhishek JoshiNo ratings yet
- Herbal CosmeticsDocument40 pagesHerbal CosmeticsBiren Shah100% (1)
- PDF DipiroDocument16 pagesPDF DipiroYolandaFandraIINo ratings yet
- Swedish MassageDocument22 pagesSwedish Massagealejandro jean100% (3)
- Swollen Neck Lymph Nodes - Causes - Better MedicineDocument6 pagesSwollen Neck Lymph Nodes - Causes - Better MedicineDanao ErickNo ratings yet
- Starch Industry in IndiaDocument3 pagesStarch Industry in Indiabanapte59No ratings yet
- Leisure Awareness ActivitiesDocument9 pagesLeisure Awareness Activitiesapi-301398957No ratings yet
- The Clinical Management of Awake BruxismDocument30 pagesThe Clinical Management of Awake BruxismSahana RangarajanNo ratings yet
- SPDX Week 8 - Perfusion TechnologyDocument2 pagesSPDX Week 8 - Perfusion TechnologyerikajoydmrmtNo ratings yet
- Koppenaal2020 Article EffectivenessAndCost-effectiveDocument13 pagesKoppenaal2020 Article EffectivenessAndCost-effectivePaulomds1991No ratings yet
- 1-Legal Med Notes PDFDocument19 pages1-Legal Med Notes PDFFrenza Joy FresnidoNo ratings yet
- Super fi cial roughness on composite surface, composite enamel and composite dentin junctions after different fi nishing and polishing procedures. Part I: roughness after treatments with tungsten carbide vs diamond bursDocument20 pagesSuper fi cial roughness on composite surface, composite enamel and composite dentin junctions after different fi nishing and polishing procedures. Part I: roughness after treatments with tungsten carbide vs diamond bursCinthyaNavarroNo ratings yet
- ATI Module - Ethical Principles For Mental HealthDocument6 pagesATI Module - Ethical Principles For Mental HealthChelsea HebertNo ratings yet
- Cholelithiasis When They Are in The Bile CholedocolithiasisDocument15 pagesCholelithiasis When They Are in The Bile Choledocolithiasishisabumohamed100% (1)
- Cai Songfang Wujishi Breathing Exercises Medicine Health Publishing Co. 1994Document119 pagesCai Songfang Wujishi Breathing Exercises Medicine Health Publishing Co. 1994Amlen Singha100% (2)