Download as pdf or txt
You might also like
- To Make Flip Flop Led Flasher Circuit Using Transistor Bc547Document17 pagesTo Make Flip Flop Led Flasher Circuit Using Transistor Bc547ananyabedekar83No ratings yet
- The Essentials of Psychodynamic PsychotherapyDocument6 pagesThe Essentials of Psychodynamic PsychotherapyMarthaRamirez100% (3)
- Gastroschisis DNYDocument37 pagesGastroschisis DNYDonny Artya KesumaNo ratings yet
- Lab2 PDFDocument3 pagesLab2 PDFMd.Arifur RahmanNo ratings yet
- Bullying, Stalking and ExtortionDocument17 pagesBullying, Stalking and ExtortionJLafge83% (6)
- Non Aero Revenue - MBA ProjectDocument68 pagesNon Aero Revenue - MBA ProjectSuresh Kumar100% (2)
- Postoperative Complications and Functional Outcome After Esophageal Atresia Repair: Results From Longitudinal Single-Center Follow-UpDocument9 pagesPostoperative Complications and Functional Outcome After Esophageal Atresia Repair: Results From Longitudinal Single-Center Follow-Upzivl1984No ratings yet
- Imaging of Congenital Anomalies of The Gastrointestinal TractDocument12 pagesImaging of Congenital Anomalies of The Gastrointestinal TractMateen ShukriNo ratings yet
- Pa Tho Physiology of HirschprungDocument4 pagesPa Tho Physiology of HirschprungRenz Javier Tuñacao LustreNo ratings yet
- Reflection For 79th Annual Clinical Congress 24th Asian Congress of SurgeryDocument4 pagesReflection For 79th Annual Clinical Congress 24th Asian Congress of Surgerysjmc.surgeryresidentsNo ratings yet
- Incarceratedpediatric Hernias: Sophia A. Abdulhai,, Ian C. Glenn,, Todd A. PonskyDocument17 pagesIncarceratedpediatric Hernias: Sophia A. Abdulhai,, Ian C. Glenn,, Todd A. PonskyPhytoplankton DiatomsNo ratings yet
- AfrJPaediatrSurg122119-3052943 082849 PDFDocument3 pagesAfrJPaediatrSurg122119-3052943 082849 PDFAndikaNo ratings yet
- Temporary Retrograde Occlusion of High-Flow Tracheo-Esophageal FistulaDocument6 pagesTemporary Retrograde Occlusion of High-Flow Tracheo-Esophageal FistulaGunduz AgaNo ratings yet
- De La TorreDocument11 pagesDe La TorreRAPTOR111No ratings yet
- New Developments in Anal Surgery Congenital Ano RectalDocument5 pagesNew Developments in Anal Surgery Congenital Ano RectalOctavianus KevinNo ratings yet
- Peg & TPNDocument23 pagesPeg & TPNapi-3722454100% (1)
- Basic Principles of Enteral Feeding: Hale AkbaylarDocument6 pagesBasic Principles of Enteral Feeding: Hale AkbaylarAbdul NazirNo ratings yet
- Management of Rectal Prolapse P WAGDocument19 pagesManagement of Rectal Prolapse P WAGWaNda GrNo ratings yet
- Supra-Transumbilical Laparotomy (STL) Approach For Small Bowel Atresia Repair: Our Experience and Review of The LiteratureDocument5 pagesSupra-Transumbilical Laparotomy (STL) Approach For Small Bowel Atresia Repair: Our Experience and Review of The LiteratureFebri Nick Daniel SihombingNo ratings yet
- GASTROSCHISISDocument4 pagesGASTROSCHISISVin Custodio100% (1)
- 10.7556 Jaoa.2011.111.1.44Document5 pages10.7556 Jaoa.2011.111.1.44DianaNo ratings yet
- Management of Rectal Prolapse in Children: Our Experience of Thiersch Stitch ProcedureDocument4 pagesManagement of Rectal Prolapse in Children: Our Experience of Thiersch Stitch Procedureade-djufrieNo ratings yet
- Tracheoesophageal Atresia: Mrs - Smitha.M Associate Professor Vijaya College of Nursing KottarakkaraDocument10 pagesTracheoesophageal Atresia: Mrs - Smitha.M Associate Professor Vijaya College of Nursing KottarakkarakrishnasreeNo ratings yet
- A Retrospective Clinical Study of Perforation Peritonitis in Rural Area in Andhra Pradesh November 2022 9921131660 120 PDFDocument9 pagesA Retrospective Clinical Study of Perforation Peritonitis in Rural Area in Andhra Pradesh November 2022 9921131660 120 PDFVijay KumarNo ratings yet
- Management of Jejunoileal Atresia: Our 5 Year ExperienceDocument4 pagesManagement of Jejunoileal Atresia: Our 5 Year ExperienceOvamelia JulioNo ratings yet
- Fistula Enterokutan 1Document8 pagesFistula Enterokutan 1Amalia GrahaniNo ratings yet
- OmphaloceleDocument23 pagesOmphaloceleFred PupeNo ratings yet
- Fistula Enterokutan 1Document8 pagesFistula Enterokutan 1Amalia GrahaniNo ratings yet
- Colonic Atresia Revision 1Document10 pagesColonic Atresia Revision 1HenggarAPNo ratings yet
- Atresia Esofágica Con Fistula Traqueoesofágica DistalDocument24 pagesAtresia Esofágica Con Fistula Traqueoesofágica DistalChristian PA100% (1)
- 2 Gastric and Duodenal Peptic Ulcer Disease 2Document35 pages2 Gastric and Duodenal Peptic Ulcer Disease 2rayNo ratings yet
- Paediatric AnsDocument142 pagesPaediatric AnsAbdulkadir HasanNo ratings yet
- Shalita Dastamuar Pediatric Surgery Subdivision, Surgery Department Mohammad Hoesin HospitalDocument18 pagesShalita Dastamuar Pediatric Surgery Subdivision, Surgery Department Mohammad Hoesin HospitalSoni TfacNo ratings yet
- Hernia Hiatal 3Document10 pagesHernia Hiatal 3María Alejandra García QNo ratings yet
- Common Pediatric Surgery ProblemsDocument141 pagesCommon Pediatric Surgery Problemssedaka26100% (4)
- Common Neonatal Surgical Conditions: Intensive Care Nursery House Staff ManualDocument6 pagesCommon Neonatal Surgical Conditions: Intensive Care Nursery House Staff ManualSayf QisthiNo ratings yet
- Common Complication: What Is It?Document5 pagesCommon Complication: What Is It?khalidicuNo ratings yet
- Chylous Ascites Following Kasai PortoentDocument3 pagesChylous Ascites Following Kasai PortoentАлександра КондряNo ratings yet
- Gastro SCH Is IsDocument13 pagesGastro SCH Is IsferoNo ratings yet
- A Literature Review of Percutaneous Endoscopic Gastrostomy: Dealing With ComplicationsDocument9 pagesA Literature Review of Percutaneous Endoscopic Gastrostomy: Dealing With ComplicationsHenry BarberenaNo ratings yet
- Enteral Feeding: Gastric Versus Post-Pyloric: Table 1Document22 pagesEnteral Feeding: Gastric Versus Post-Pyloric: Table 1tasmeow23No ratings yet
- Case Report On Spontaneous Restoration of Bowel ContinuityDocument5 pagesCase Report On Spontaneous Restoration of Bowel Continuityofficial.drjainNo ratings yet
- BaldwinDocument6 pagesBaldwinalexafarrenNo ratings yet
- Seminars in Pediatric Surgery: Short Bowel Syndrome in Children: Surgical and Medical PerspectivesDocument7 pagesSeminars in Pediatric Surgery: Short Bowel Syndrome in Children: Surgical and Medical PerspectivesrodyNo ratings yet
- Outcomes of Percutaneous Endoscopic Gastrostomy in ChildrenDocument7 pagesOutcomes of Percutaneous Endoscopic Gastrostomy in ChildrenHenry BarberenaNo ratings yet
- Pyloric Stenosis WDocument11 pagesPyloric Stenosis WKlaue Neiv CallaNo ratings yet
- Oesophageal Atresia by GabriellaDocument7 pagesOesophageal Atresia by GabriellaGabrielleNo ratings yet
- Intestinal Atresia: A Case ReportDocument3 pagesIntestinal Atresia: A Case ReportOvamelia JulioNo ratings yet
- Explor LaparotomyDocument14 pagesExplor LaparotomyGracia NievesNo ratings yet
- Adult Intussusception A Case ReportDocument4 pagesAdult Intussusception A Case ReportRahmanssNo ratings yet
- Minimallyinvasive Esophagectomyforbenign Disease: Blair A. JobeDocument10 pagesMinimallyinvasive Esophagectomyforbenign Disease: Blair A. JobeYacine Tarik AizelNo ratings yet
- 3 Common Pediatric Surgery ContinuedDocument5 pages3 Common Pediatric Surgery ContinuedMohamed Al-zichrawyNo ratings yet
- Infant With Pentalogy of Cantrell and Tetralogy of Fallot Requiring Omphalocele RepairDocument6 pagesInfant With Pentalogy of Cantrell and Tetralogy of Fallot Requiring Omphalocele RepairThia SanjayaNo ratings yet
- Transanal Endorectal PullthroughDocument8 pagesTransanal Endorectal PullthroughMuhammad Harmen Reza SiregarNo ratings yet
- Tubular Ileal Duplication Causing Small Bowel Obstruction in A ChildDocument5 pagesTubular Ileal Duplication Causing Small Bowel Obstruction in A ChildDiego Leonardo Herrera OjedaNo ratings yet
- 1 s2.0 S105585861200090X MainDocument6 pages1 s2.0 S105585861200090X Mainmchojnacki81No ratings yet
- j.jpedsurg.2019.12.020Document6 pagesj.jpedsurg.2019.12.020Cirugia pediatrica CMN RAZA Cirugia pediatricaNo ratings yet
- Intestinaltransplantin Children: Nidhi Rawal,, Nada YazigiDocument7 pagesIntestinaltransplantin Children: Nidhi Rawal,, Nada YazigimacedovendezuNo ratings yet
- Gastroesophageal Reflux With Relevance To Pediatric Surgery - Presentation TranscriptDocument4 pagesGastroesophageal Reflux With Relevance To Pediatric Surgery - Presentation TranscriptAbdul Ghaffar AbdullahNo ratings yet
- Hirschsprun G'S Disease: Dr. Manish Kumar Gupta Assistant Professor Department of Paediatric Surgery AIIMS, RishikeshDocument48 pagesHirschsprun G'S Disease: Dr. Manish Kumar Gupta Assistant Professor Department of Paediatric Surgery AIIMS, RishikeshArchana Mahata100% (1)
- 19-Pediatric SurgeryDocument39 pages19-Pediatric Surgerycallisto3487No ratings yet
- Neonatal Tracheostomy - JonathanWalsh 2018Document12 pagesNeonatal Tracheostomy - JonathanWalsh 2018Ismael Erazo AstudilloNo ratings yet
- AtresiaDocument5 pagesAtresiakirtiNo ratings yet
- Laparoscopic Hernia Repair in Neonates, Infants and ChildrenDocument9 pagesLaparoscopic Hernia Repair in Neonates, Infants and ChildrenErick OematanNo ratings yet
- Prune Belly SyndromeDocument39 pagesPrune Belly SyndromeHudaNo ratings yet
- Esophageal Preservation and Replacement in ChildrenFrom EverandEsophageal Preservation and Replacement in ChildrenAshwin PimpalwarNo ratings yet
- Fingertips Injury: Literature ReviewDocument24 pagesFingertips Injury: Literature ReviewDonny Artya KesumaNo ratings yet
- Wound Infection SepsisDocument27 pagesWound Infection SepsisDonny Artya KesumaNo ratings yet
- Green 2016Document6 pagesGreen 2016Donny Artya KesumaNo ratings yet
- AsianJNeurosurg82112-3813641 103536Document4 pagesAsianJNeurosurg82112-3813641 103536Donny Artya KesumaNo ratings yet
- Bedah Saraf OscaDocument11 pagesBedah Saraf OscaDonny Artya KesumaNo ratings yet
- JCO 2005 Low 2726 34Document9 pagesJCO 2005 Low 2726 34Donny Artya KesumaNo ratings yet
- Percutaneous Aponeurotomy and Lipofilling: A Regenerative Alternative To Flap Reconstruction?Document11 pagesPercutaneous Aponeurotomy and Lipofilling: A Regenerative Alternative To Flap Reconstruction?Donny Artya KesumaNo ratings yet
- Kon Trak TurDocument6 pagesKon Trak TurZico ParadigmaNo ratings yet
- EoI DocumentDocument45 pagesEoI Documentudi969No ratings yet
- Senwa Mobile - S615 - Android 3.5inDocument6 pagesSenwa Mobile - S615 - Android 3.5inSERGIO_MANNo ratings yet
- Product Data Sheet Ingenuity Core LRDocument16 pagesProduct Data Sheet Ingenuity Core LRCeoĐứcTrườngNo ratings yet
- Shaping The Way We Teach English:: Successful Practices Around The WorldDocument5 pagesShaping The Way We Teach English:: Successful Practices Around The WorldCristina DiaconuNo ratings yet
- Linkages and NetworkDocument28 pagesLinkages and NetworkJoltzen GuarticoNo ratings yet
- Piglia - Hotel AlmagroDocument2 pagesPiglia - Hotel AlmagroJustin LokeNo ratings yet
- Teacher Learning Walk Templates - 2017 - 1Document13 pagesTeacher Learning Walk Templates - 2017 - 1Zakaria Md SaadNo ratings yet
- Present Continuous - Present Simple Vs Present ContinuousDocument2 pagesPresent Continuous - Present Simple Vs Present ContinuouseewuanNo ratings yet
- PBL KaleidoscopeDocument3 pagesPBL KaleidoscopeWilson Tie Wei ShenNo ratings yet
- Artificial Intelligence and Patent LawDocument4 pagesArtificial Intelligence and Patent LawSaksham TyagiNo ratings yet
- The Quiescent Benefits and Drawbacks of Coffee IntakeDocument6 pagesThe Quiescent Benefits and Drawbacks of Coffee IntakeVikram Singh ChauhanNo ratings yet
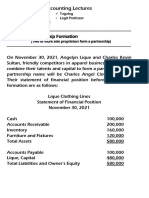
- 8 Lec 03 - Partnership Formation With BusinessDocument2 pages8 Lec 03 - Partnership Formation With BusinessNathalie GetinoNo ratings yet
- LEARNING THEORIES Ausubel's Learning TheoryDocument17 pagesLEARNING THEORIES Ausubel's Learning TheoryCleoNo ratings yet
- Proposal (Objective Jpurpose Jscope)Document3 pagesProposal (Objective Jpurpose Jscope)Lee ChloeNo ratings yet
- British Baker Top Bakery Trends 2023Document15 pagesBritish Baker Top Bakery Trends 2023kiagus artaNo ratings yet
- Comprehension Toolkit 1Document3 pagesComprehension Toolkit 1api-510893209No ratings yet
- Security and Privacy Issues: A Survey On Fintech: (Kg71231W, Mqiu, Xs43599N) @pace - EduDocument12 pagesSecurity and Privacy Issues: A Survey On Fintech: (Kg71231W, Mqiu, Xs43599N) @pace - EduthebestNo ratings yet
- GIS Based Analysis On Walkability of Commercial Streets at Continuing Growth Stages - EditedDocument11 pagesGIS Based Analysis On Walkability of Commercial Streets at Continuing Growth Stages - EditedemmanuelNo ratings yet
- Tunis Stock ExchangeDocument54 pagesTunis Stock ExchangeAnonymous AoDxR5Rp4JNo ratings yet
- M HealthDocument81 pagesM HealthAbebe ChekolNo ratings yet
- Common AddictionsDocument13 pagesCommon AddictionsMaría Cecilia CarattoliNo ratings yet
- Asco Power Transfer Switch Comparison Features-3149 134689 0Document2 pagesAsco Power Transfer Switch Comparison Features-3149 134689 0angel aguilarNo ratings yet
- Metaverse Report - Thought Leadership 1Document17 pagesMetaverse Report - Thought Leadership 1Tejas KNo ratings yet
- Unit - 2 Sensor Networks - Introduction & ArchitecturesDocument32 pagesUnit - 2 Sensor Networks - Introduction & Architecturesmurlak37No ratings yet
- Print - Udyam Registration CertificateDocument2 pagesPrint - Udyam Registration CertificatesahityaasthaNo ratings yet