Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5822)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Procedures For Submitting Samples For Testing For Ebola Virus InfectionDocument3 pagesProcedures For Submitting Samples For Testing For Ebola Virus InfectionssucbbaNo ratings yet
- Vastarel MR From Decades of Clinical Experience inDocument6 pagesVastarel MR From Decades of Clinical Experience inJonathan Ian ArinsolNo ratings yet
- Penyusunan Status PsikiatriDocument82 pagesPenyusunan Status PsikiatrikharisaNo ratings yet
- Viva Questions of Final Professional ExaminationDocument48 pagesViva Questions of Final Professional ExaminationFaisol KabirNo ratings yet
- TPS 2020 - Bahasa Inggris: Pilihan A (Salah), Karena Teks Ini BukanDocument11 pagesTPS 2020 - Bahasa Inggris: Pilihan A (Salah), Karena Teks Ini BukanFarayaNo ratings yet
- Benchmark Evidence BasedDocument11 pagesBenchmark Evidence BasedPeterNo ratings yet
- Ntruhs Dissertation Topics in PaediatricsDocument8 pagesNtruhs Dissertation Topics in PaediatricsNeedHelpWriteMyPaperCanada100% (1)
- Annexure-A Form No 2 UCO Bank Application For Commutation of Pension Subject To Medical Examination. (To Be Submitted in Duplicate) Part-IDocument7 pagesAnnexure-A Form No 2 UCO Bank Application For Commutation of Pension Subject To Medical Examination. (To Be Submitted in Duplicate) Part-Ipranav11No ratings yet
- Cough, Cold and AllergiesDocument68 pagesCough, Cold and AllergiesLeonardo RanderNo ratings yet
- E2 Writing Subtest 3Document4 pagesE2 Writing Subtest 3njNo ratings yet
- What Are The Core Elements of PCC A Narrative ReviewDocument12 pagesWhat Are The Core Elements of PCC A Narrative ReviewDario SanabriaNo ratings yet
- Booklet ECbgugiuDMFR2014Document33 pagesBooklet ECbgugiuDMFR2014Oana MariaNo ratings yet
- ChoreaDocument6 pagesChoreamainehoonaNo ratings yet
- Jurnal 1Document9 pagesJurnal 1Aulia Putri ANo ratings yet
- 3 AmphetaminesDocument4 pages3 AmphetaminesNouman Safdar AliNo ratings yet
- Gynecology & Obstetrics Medical Conferences-The Ovary UnraveledDocument12 pagesGynecology & Obstetrics Medical Conferences-The Ovary Unraveledovary2009No ratings yet
- Sifrol® ER: What Is in This LeafletDocument3 pagesSifrol® ER: What Is in This LeafletDenaraAshaPutriNo ratings yet
- Onions: The Talmud Further Elucidates The Benefits of Onions With Regard To The Treatment of WoundsDocument2 pagesOnions: The Talmud Further Elucidates The Benefits of Onions With Regard To The Treatment of Woundsoutdash2No ratings yet
- CRM in HospitalsDocument5 pagesCRM in HospitalsSubramanya DgNo ratings yet
- Abnormalpuerperium 190328060723 1Document126 pagesAbnormalpuerperium 190328060723 1Preeti ChouhanNo ratings yet
- 2 Medical Knowledge and The Power of GodDocument5 pages2 Medical Knowledge and The Power of Godapi-247725573No ratings yet
- Michael Angelo A. Nombre (BSN-2D) : "Medical Abbreviations On Pharmacy Prescriptions"Document25 pagesMichael Angelo A. Nombre (BSN-2D) : "Medical Abbreviations On Pharmacy Prescriptions"clint xavier odangoNo ratings yet
- A Rat Model For Oral Mucositis Induced byDocument7 pagesA Rat Model For Oral Mucositis Induced byYanski DarmantoNo ratings yet
- Possessive Adjectives and Object PronounsDocument4 pagesPossessive Adjectives and Object PronounsHugo MoreyraNo ratings yet
- Chen, S., Et - Al. (2020) - (01-11)Document11 pagesChen, S., Et - Al. (2020) - (01-11)Vielia IrmayantiNo ratings yet
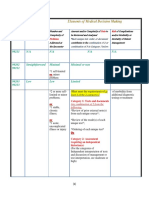
- 3-Level of MDMDocument3 pages3-Level of MDMmedical codingNo ratings yet
- 11 BreastDocument22 pages11 BreastMohammed GhozzNo ratings yet
- Ophthalmology Easy GuideDocument46 pagesOphthalmology Easy Guidesri sinaga0% (1)
- Argumentative Essay Revised1Document8 pagesArgumentative Essay Revised1api-253812610100% (1)
- Tablets 100 MG: DipyridamoleDocument1 pageTablets 100 MG: DipyridamoleAat Prayoga MuhtarNo ratings yet