
Drugs That Cause Movement Disorders: October 1, 2008 - Michele B. Kaufman, Pharmd, BSC, RPH
Drugs That Cause Movement Disorders: October 1, 2008 - Michele B. Kaufman, Pharmd, BSC, RPH
You might also like
- Dusi RDocument5 pagesDusi Remanuelxaviervale50% (2)
- Bicycle DayDocument2 pagesBicycle Daytexastig2347No ratings yet
- CIRCULAR NR 03 (PAF Anti-Narcotics Policy)Document4 pagesCIRCULAR NR 03 (PAF Anti-Narcotics Policy)Air ProvostNo ratings yet
- Medication-Induced Tardive Dyskinesia: A Review and Update: Reviews and Contemporary UpdatesDocument11 pagesMedication-Induced Tardive Dyskinesia: A Review and Update: Reviews and Contemporary UpdatesudzmaNo ratings yet
- Antipsychotic-Related Movement Disorders: Drug-Induced Parkinsonism vs. Tardive Dyskinesia-Key Differences in Pathophysiology and Clinical ManagementDocument16 pagesAntipsychotic-Related Movement Disorders: Drug-Induced Parkinsonism vs. Tardive Dyskinesia-Key Differences in Pathophysiology and Clinical ManagementudzmaNo ratings yet
- Tardive Dyskinesia Prevention, Treatment, and PrognosisDocument22 pagesTardive Dyskinesia Prevention, Treatment, and PrognosisTiago Manuel AfonsoNo ratings yet
- Antipsychotics,-WPS OfficeDocument7 pagesAntipsychotics,-WPS Officermconvidhya sri2015No ratings yet
- Schizophrenia Treatment & ManagementDocument16 pagesSchizophrenia Treatment & ManagementDimas Januar100% (2)
- Choosing WiselyDocument5 pagesChoosing WiselyHiba RahmanNo ratings yet
- Tardive DyskinesiaDocument2 pagesTardive DyskinesiaFabianNo ratings yet
- Psychotropic MedicationDocument28 pagesPsychotropic Medicationrmconvidhya sri2015No ratings yet
- Adverse Effects of Antipsychotic DrugsDocument18 pagesAdverse Effects of Antipsychotic DrugsBhumika PatelNo ratings yet
- Neuroleptic Malignant SyndromeDocument11 pagesNeuroleptic Malignant SyndromeEddy ChungNo ratings yet
- 2014 Tardive Dyskinesia in Patients Treated With Atypical AntipsychoticsDocument10 pages2014 Tardive Dyskinesia in Patients Treated With Atypical AntipsychoticsDiego HormacheaNo ratings yet
- Managementul BenzodiazepinelorDocument10 pagesManagementul BenzodiazepinelorSendruc OvidiuNo ratings yet
- PSYCHOPHARMACOLOGYDocument33 pagesPSYCHOPHARMACOLOGYAddisu EngdawNo ratings yet
- A Propofol Based Palliative Sedation Used To Treat Antipsychotic Resistant Agitated DeliriumDocument4 pagesA Propofol Based Palliative Sedation Used To Treat Antipsychotic Resistant Agitated DeliriumMaría LCNo ratings yet
- Polypharmacy in The: The Bagful of Pills: ElderlyDocument34 pagesPolypharmacy in The: The Bagful of Pills: ElderlyrandatagNo ratings yet
- NMSPostgrad Med J 2008 Jackson 121 6Document7 pagesNMSPostgrad Med J 2008 Jackson 121 6afeda_886608No ratings yet
- Flupentixol Melitracen Prescribing InformationDocument11 pagesFlupentixol Melitracen Prescribing Informationsa5856721No ratings yet
- Mental Health Nursing Care PlanDocument24 pagesMental Health Nursing Care Plancuicuita100% (4)
- Schizophrenia Treatment & Management - Approach Considerations, Antipsychotic Pharmacotherapy, Other PharmacotherapyDocument13 pagesSchizophrenia Treatment & Management - Approach Considerations, Antipsychotic Pharmacotherapy, Other PharmacotherapydilaNo ratings yet
- Aripiprazol in Delirium La Pacientii VarstniciDocument10 pagesAripiprazol in Delirium La Pacientii VarstniciRobert MovileanuNo ratings yet
- Are There Guidelines For The Responsible Prescription of Benzodiazepines?Document7 pagesAre There Guidelines For The Responsible Prescription of Benzodiazepines?Rian YupitaNo ratings yet
- Depression: Psychiatric DisordersDocument21 pagesDepression: Psychiatric DisordersNdoo NdooNo ratings yet
- Pharma AssignmentDocument41 pagesPharma AssignmentKhizra KhurshidNo ratings yet
- Pe 2 3 36Document6 pagesPe 2 3 36Oslo SaputraNo ratings yet
- Delirious You or The Patient?Document34 pagesDelirious You or The Patient?Vishala MishraNo ratings yet
- Metoclopramide - Induced Extrapyrami-Dal Signs and Symptoms - Brief Review of Literature and Case ReportDocument3 pagesMetoclopramide - Induced Extrapyrami-Dal Signs and Symptoms - Brief Review of Literature and Case ReportLulu LuwiiNo ratings yet
- Anti Psychotic MedicationsDocument6 pagesAnti Psychotic MedicationsCandace AngelNo ratings yet
- Extrapyramidal Symptoms - StatPearls - NCBI BookshelfDocument6 pagesExtrapyramidal Symptoms - StatPearls - NCBI BookshelfFitrah RahmadhaniNo ratings yet
- Delirium in Intensive Care UnitDocument13 pagesDelirium in Intensive Care UnitMedeiros SilvaNo ratings yet
- S 030 LblmineDocument14 pagesS 030 LblmineLeslie HouseNo ratings yet
- Treatment of Classic Syndromes in Idiopathic Focal Epilepsies in ChildhoodDocument9 pagesTreatment of Classic Syndromes in Idiopathic Focal Epilepsies in ChildhoodampalNo ratings yet
- Pharmacology (Psychosis and Mania)Document53 pagesPharmacology (Psychosis and Mania)lavanyakakarlaNo ratings yet
- 10 1016@j NCL 2020 01 004Document18 pages10 1016@j NCL 2020 01 004lucashortencioNo ratings yet
- Practice GuidelineDocument3 pagesPractice Guidelineclarajimena25No ratings yet
- Anti Psychotic DrugsDocument6 pagesAnti Psychotic DrugsJoseph NyirongoNo ratings yet
- Management of Parkinson's DiseaseDocument20 pagesManagement of Parkinson's DiseasePia S.No ratings yet
- Psy PRBLM 2 EsrdDocument5 pagesPsy PRBLM 2 EsrdNoreen ChoudhriNo ratings yet
- En A09v83n2s0 PDFDocument12 pagesEn A09v83n2s0 PDFRiriNo ratings yet
- Psychiatric Nursing - Psycho PharmacologyDocument50 pagesPsychiatric Nursing - Psycho PharmacologyKaren MichelleNo ratings yet
- 2012 Updates in Therapeutics: Geriatrics: Patient Case 1Document20 pages2012 Updates in Therapeutics: Geriatrics: Patient Case 1andirio7486No ratings yet
- Alterations of Dopamine D2 Receptors and Related Receptor-Interacting Proteins in Schizophrenia - The Pivotal Position of Dopamine Supersensitivity Psychosis in Treatment-Resistatn SchizophreniaDocument20 pagesAlterations of Dopamine D2 Receptors and Related Receptor-Interacting Proteins in Schizophrenia - The Pivotal Position of Dopamine Supersensitivity Psychosis in Treatment-Resistatn SchizophreniaJuan IgnacioNo ratings yet
- Antipsychotic Toxicity and Poisoning - CorePendiumDocument14 pagesAntipsychotic Toxicity and Poisoning - CorePendiumyvvs5f9m4mNo ratings yet
- Deanxit SPCDocument10 pagesDeanxit SPCXajepoxNo ratings yet
- ADR Medicine 36 7 2008Document5 pagesADR Medicine 36 7 2008Indri WidyantiNo ratings yet
- HaloperidolDocument4 pagesHaloperidolNickol BaylonNo ratings yet
- Sam ADocument10 pagesSam AAngela Rivas CastilloNo ratings yet
- Anticholinergics and AmantadineDocument7 pagesAnticholinergics and Amantadineshofia nailahNo ratings yet
- Metoclopromide Related Secondary Parkinsonism and Domperidone Safety in Parkinson DiseaseDocument21 pagesMetoclopromide Related Secondary Parkinsonism and Domperidone Safety in Parkinson DiseaseHemabaluNo ratings yet
- MimdDocument7 pagesMimdwairimuagatha9No ratings yet
- Psychiatric Emergencies and Nursing ManagementDocument40 pagesPsychiatric Emergencies and Nursing Managementavanthikasathiya29No ratings yet
- TMP - 6100-Tardive PGMay04Article3Document7 pagesTMP - 6100-Tardive PGMay04Article3ajescoolNo ratings yet
- Anti PsychoticsDocument23 pagesAnti PsychoticstabletvodaNo ratings yet
- Acute Confusional State ManagementDocument18 pagesAcute Confusional State ManagementAhmed AbdelgelilNo ratings yet
- Journal Reading: Diagnosis and Treatment of Patients With Bipolar Disorder: A Review For Advanced Practice NursesDocument28 pagesJournal Reading: Diagnosis and Treatment of Patients With Bipolar Disorder: A Review For Advanced Practice NursesAditya Chandra ForestaNo ratings yet
- Parkinson's Disease: Neurovascular DisordersDocument24 pagesParkinson's Disease: Neurovascular DisordersNdoo NdooNo ratings yet
- AntipsychoticsDocument51 pagesAntipsychoticsShailja SharmaNo ratings yet
- Neuro Assignment-Syed Wajahat Ali NaqviDocument6 pagesNeuro Assignment-Syed Wajahat Ali NaqviSyed Wajahat AliNo ratings yet
- Wjem 13 01 26 PDFDocument9 pagesWjem 13 01 26 PDFMoises Vega RodriguezNo ratings yet
- Neuroleptic DrugDocument7 pagesNeuroleptic DrugyunikNo ratings yet
- Evidence Supported Interventions: Psychedelic-Assisted TherapyDocument8 pagesEvidence Supported Interventions: Psychedelic-Assisted TherapyJeanne PorgesNo ratings yet
- BK0136 Patterns and Trends of Amphetamine Type Stimulants ATS and ODocument152 pagesBK0136 Patterns and Trends of Amphetamine Type Stimulants ATS and OAnti NarkobaNo ratings yet
- Graylands Hospital Drug Bulletin: Focus On BenzodiazepinesDocument4 pagesGraylands Hospital Drug Bulletin: Focus On BenzodiazepinesStacia Carla CarolineNo ratings yet
- Drinking Age Bar Should Be at 21 Years OldDocument10 pagesDrinking Age Bar Should Be at 21 Years OldVincent ForbesNo ratings yet
- Addiction ScriptDocument19 pagesAddiction ScriptLaica A. LunetaNo ratings yet
- Lecture 8 Central Nervous System CnsDocument35 pagesLecture 8 Central Nervous System CnsakramuddaulaNo ratings yet
- Presented By:-11081506 (Ridhi) 11081524 (Khushboo) 11081560 (Shiny) 11081542 (Sakshi)Document17 pagesPresented By:-11081506 (Ridhi) 11081524 (Khushboo) 11081560 (Shiny) 11081542 (Sakshi)Akanksha KapoorNo ratings yet
- Mechanism and Side Effects of SSRI 1Document13 pagesMechanism and Side Effects of SSRI 1Andika MetrisiawanNo ratings yet
- Frisium Knowledge ModuleDocument7 pagesFrisium Knowledge ModulesiddiqrehanNo ratings yet
- Elfani Nur Sita Augustina-19084Document6 pagesElfani Nur Sita Augustina-19084elfannynr augustinaNo ratings yet
- Anxiolytics Sedatives Hypnotics Pharm 3Document38 pagesAnxiolytics Sedatives Hypnotics Pharm 3Peter Harris100% (1)
- Ethical Use of CannabisDocument3 pagesEthical Use of CannabisMile PrikopNo ratings yet
- Drug Education and Vice ControlDocument25 pagesDrug Education and Vice ControlShan Jerome Lapuz SamoyNo ratings yet
- MDTH: Mood Disorders Treatment History FormDocument3 pagesMDTH: Mood Disorders Treatment History FormLaura ParkaNo ratings yet
- Chapter Overview: Psychoactive Drugs: Classification and HistoryDocument20 pagesChapter Overview: Psychoactive Drugs: Classification and HistorySiddharth soniNo ratings yet
- Annotated BibliographyDocument6 pagesAnnotated Bibliographyapi-451590039No ratings yet
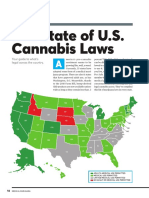
- The State of U.S. Cannabis Laws, AbridgedDocument6 pagesThe State of U.S. Cannabis Laws, AbridgedPaul Marini100% (1)
- Cannabidiol (CBD)Document8 pagesCannabidiol (CBD)Isaias Sanches LopezNo ratings yet
- RA 9165 ComprehensiveDangerous Drugs Act of 2002 An Overview Presented ByCRIMINOLOGY INTERNDocument4 pagesRA 9165 ComprehensiveDangerous Drugs Act of 2002 An Overview Presented ByCRIMINOLOGY INTERNRaemmanlagradaNo ratings yet
- 2 Executive Order On BADACDocument8 pages2 Executive Order On BADACSto Niño PagadianNo ratings yet
- Sedative and HypnoticsDocument26 pagesSedative and HypnoticsZarish IftikharNo ratings yet
- Drug StudyDocument3 pagesDrug StudyJezen SucalitNo ratings yet
- Cannabinoid and Terpene InfoDocument2 pagesCannabinoid and Terpene Infosirwilliam1991No ratings yet
- Clinical AssignmentDocument22 pagesClinical AssignmentKeziah GillNo ratings yet
- BupropionDocument13 pagesBupropion18.10.1986No ratings yet
- PHR 302: Medicinal Chemistry-I: Sedative-Hypnotic DrugsDocument63 pagesPHR 302: Medicinal Chemistry-I: Sedative-Hypnotic Drugs53-Deepankar SutradharNo ratings yet
- Drugs: What Is A Drug??Document9 pagesDrugs: What Is A Drug??Alyzza BorrasNo ratings yet
























































































Download as docx, pdf, or txt
You might also like
- Dusi RDocument5 pagesDusi Remanuelxaviervale50% (2)
- Bicycle DayDocument2 pagesBicycle Daytexastig2347No ratings yet
- CIRCULAR NR 03 (PAF Anti-Narcotics Policy)Document4 pagesCIRCULAR NR 03 (PAF Anti-Narcotics Policy)Air ProvostNo ratings yet
- Medication-Induced Tardive Dyskinesia: A Review and Update: Reviews and Contemporary UpdatesDocument11 pagesMedication-Induced Tardive Dyskinesia: A Review and Update: Reviews and Contemporary UpdatesudzmaNo ratings yet
- Antipsychotic-Related Movement Disorders: Drug-Induced Parkinsonism vs. Tardive Dyskinesia-Key Differences in Pathophysiology and Clinical ManagementDocument16 pagesAntipsychotic-Related Movement Disorders: Drug-Induced Parkinsonism vs. Tardive Dyskinesia-Key Differences in Pathophysiology and Clinical ManagementudzmaNo ratings yet
- Tardive Dyskinesia Prevention, Treatment, and PrognosisDocument22 pagesTardive Dyskinesia Prevention, Treatment, and PrognosisTiago Manuel AfonsoNo ratings yet
- Antipsychotics,-WPS OfficeDocument7 pagesAntipsychotics,-WPS Officermconvidhya sri2015No ratings yet
- Schizophrenia Treatment & ManagementDocument16 pagesSchizophrenia Treatment & ManagementDimas Januar100% (2)
- Choosing WiselyDocument5 pagesChoosing WiselyHiba RahmanNo ratings yet
- Tardive DyskinesiaDocument2 pagesTardive DyskinesiaFabianNo ratings yet
- Psychotropic MedicationDocument28 pagesPsychotropic Medicationrmconvidhya sri2015No ratings yet
- Adverse Effects of Antipsychotic DrugsDocument18 pagesAdverse Effects of Antipsychotic DrugsBhumika PatelNo ratings yet
- Neuroleptic Malignant SyndromeDocument11 pagesNeuroleptic Malignant SyndromeEddy ChungNo ratings yet
- 2014 Tardive Dyskinesia in Patients Treated With Atypical AntipsychoticsDocument10 pages2014 Tardive Dyskinesia in Patients Treated With Atypical AntipsychoticsDiego HormacheaNo ratings yet
- Managementul BenzodiazepinelorDocument10 pagesManagementul BenzodiazepinelorSendruc OvidiuNo ratings yet
- PSYCHOPHARMACOLOGYDocument33 pagesPSYCHOPHARMACOLOGYAddisu EngdawNo ratings yet
- A Propofol Based Palliative Sedation Used To Treat Antipsychotic Resistant Agitated DeliriumDocument4 pagesA Propofol Based Palliative Sedation Used To Treat Antipsychotic Resistant Agitated DeliriumMaría LCNo ratings yet
- Polypharmacy in The: The Bagful of Pills: ElderlyDocument34 pagesPolypharmacy in The: The Bagful of Pills: ElderlyrandatagNo ratings yet
- NMSPostgrad Med J 2008 Jackson 121 6Document7 pagesNMSPostgrad Med J 2008 Jackson 121 6afeda_886608No ratings yet
- Flupentixol Melitracen Prescribing InformationDocument11 pagesFlupentixol Melitracen Prescribing Informationsa5856721No ratings yet
- Mental Health Nursing Care PlanDocument24 pagesMental Health Nursing Care Plancuicuita100% (4)
- Schizophrenia Treatment & Management - Approach Considerations, Antipsychotic Pharmacotherapy, Other PharmacotherapyDocument13 pagesSchizophrenia Treatment & Management - Approach Considerations, Antipsychotic Pharmacotherapy, Other PharmacotherapydilaNo ratings yet
- Aripiprazol in Delirium La Pacientii VarstniciDocument10 pagesAripiprazol in Delirium La Pacientii VarstniciRobert MovileanuNo ratings yet
- Are There Guidelines For The Responsible Prescription of Benzodiazepines?Document7 pagesAre There Guidelines For The Responsible Prescription of Benzodiazepines?Rian YupitaNo ratings yet
- Depression: Psychiatric DisordersDocument21 pagesDepression: Psychiatric DisordersNdoo NdooNo ratings yet
- Pharma AssignmentDocument41 pagesPharma AssignmentKhizra KhurshidNo ratings yet
- Pe 2 3 36Document6 pagesPe 2 3 36Oslo SaputraNo ratings yet
- Delirious You or The Patient?Document34 pagesDelirious You or The Patient?Vishala MishraNo ratings yet
- Metoclopramide - Induced Extrapyrami-Dal Signs and Symptoms - Brief Review of Literature and Case ReportDocument3 pagesMetoclopramide - Induced Extrapyrami-Dal Signs and Symptoms - Brief Review of Literature and Case ReportLulu LuwiiNo ratings yet
- Anti Psychotic MedicationsDocument6 pagesAnti Psychotic MedicationsCandace AngelNo ratings yet
- Extrapyramidal Symptoms - StatPearls - NCBI BookshelfDocument6 pagesExtrapyramidal Symptoms - StatPearls - NCBI BookshelfFitrah RahmadhaniNo ratings yet
- Delirium in Intensive Care UnitDocument13 pagesDelirium in Intensive Care UnitMedeiros SilvaNo ratings yet
- S 030 LblmineDocument14 pagesS 030 LblmineLeslie HouseNo ratings yet
- Treatment of Classic Syndromes in Idiopathic Focal Epilepsies in ChildhoodDocument9 pagesTreatment of Classic Syndromes in Idiopathic Focal Epilepsies in ChildhoodampalNo ratings yet
- Pharmacology (Psychosis and Mania)Document53 pagesPharmacology (Psychosis and Mania)lavanyakakarlaNo ratings yet
- 10 1016@j NCL 2020 01 004Document18 pages10 1016@j NCL 2020 01 004lucashortencioNo ratings yet
- Practice GuidelineDocument3 pagesPractice Guidelineclarajimena25No ratings yet
- Anti Psychotic DrugsDocument6 pagesAnti Psychotic DrugsJoseph NyirongoNo ratings yet
- Management of Parkinson's DiseaseDocument20 pagesManagement of Parkinson's DiseasePia S.No ratings yet
- Psy PRBLM 2 EsrdDocument5 pagesPsy PRBLM 2 EsrdNoreen ChoudhriNo ratings yet
- En A09v83n2s0 PDFDocument12 pagesEn A09v83n2s0 PDFRiriNo ratings yet
- Psychiatric Nursing - Psycho PharmacologyDocument50 pagesPsychiatric Nursing - Psycho PharmacologyKaren MichelleNo ratings yet
- 2012 Updates in Therapeutics: Geriatrics: Patient Case 1Document20 pages2012 Updates in Therapeutics: Geriatrics: Patient Case 1andirio7486No ratings yet
- Alterations of Dopamine D2 Receptors and Related Receptor-Interacting Proteins in Schizophrenia - The Pivotal Position of Dopamine Supersensitivity Psychosis in Treatment-Resistatn SchizophreniaDocument20 pagesAlterations of Dopamine D2 Receptors and Related Receptor-Interacting Proteins in Schizophrenia - The Pivotal Position of Dopamine Supersensitivity Psychosis in Treatment-Resistatn SchizophreniaJuan IgnacioNo ratings yet
- Antipsychotic Toxicity and Poisoning - CorePendiumDocument14 pagesAntipsychotic Toxicity and Poisoning - CorePendiumyvvs5f9m4mNo ratings yet
- Deanxit SPCDocument10 pagesDeanxit SPCXajepoxNo ratings yet
- ADR Medicine 36 7 2008Document5 pagesADR Medicine 36 7 2008Indri WidyantiNo ratings yet
- HaloperidolDocument4 pagesHaloperidolNickol BaylonNo ratings yet
- Sam ADocument10 pagesSam AAngela Rivas CastilloNo ratings yet
- Anticholinergics and AmantadineDocument7 pagesAnticholinergics and Amantadineshofia nailahNo ratings yet
- Metoclopromide Related Secondary Parkinsonism and Domperidone Safety in Parkinson DiseaseDocument21 pagesMetoclopromide Related Secondary Parkinsonism and Domperidone Safety in Parkinson DiseaseHemabaluNo ratings yet
- MimdDocument7 pagesMimdwairimuagatha9No ratings yet
- Psychiatric Emergencies and Nursing ManagementDocument40 pagesPsychiatric Emergencies and Nursing Managementavanthikasathiya29No ratings yet
- TMP - 6100-Tardive PGMay04Article3Document7 pagesTMP - 6100-Tardive PGMay04Article3ajescoolNo ratings yet
- Anti PsychoticsDocument23 pagesAnti PsychoticstabletvodaNo ratings yet
- Acute Confusional State ManagementDocument18 pagesAcute Confusional State ManagementAhmed AbdelgelilNo ratings yet
- Journal Reading: Diagnosis and Treatment of Patients With Bipolar Disorder: A Review For Advanced Practice NursesDocument28 pagesJournal Reading: Diagnosis and Treatment of Patients With Bipolar Disorder: A Review For Advanced Practice NursesAditya Chandra ForestaNo ratings yet
- Parkinson's Disease: Neurovascular DisordersDocument24 pagesParkinson's Disease: Neurovascular DisordersNdoo NdooNo ratings yet
- AntipsychoticsDocument51 pagesAntipsychoticsShailja SharmaNo ratings yet
- Neuro Assignment-Syed Wajahat Ali NaqviDocument6 pagesNeuro Assignment-Syed Wajahat Ali NaqviSyed Wajahat AliNo ratings yet
- Wjem 13 01 26 PDFDocument9 pagesWjem 13 01 26 PDFMoises Vega RodriguezNo ratings yet
- Neuroleptic DrugDocument7 pagesNeuroleptic DrugyunikNo ratings yet
- Evidence Supported Interventions: Psychedelic-Assisted TherapyDocument8 pagesEvidence Supported Interventions: Psychedelic-Assisted TherapyJeanne PorgesNo ratings yet
- BK0136 Patterns and Trends of Amphetamine Type Stimulants ATS and ODocument152 pagesBK0136 Patterns and Trends of Amphetamine Type Stimulants ATS and OAnti NarkobaNo ratings yet
- Graylands Hospital Drug Bulletin: Focus On BenzodiazepinesDocument4 pagesGraylands Hospital Drug Bulletin: Focus On BenzodiazepinesStacia Carla CarolineNo ratings yet
- Drinking Age Bar Should Be at 21 Years OldDocument10 pagesDrinking Age Bar Should Be at 21 Years OldVincent ForbesNo ratings yet
- Addiction ScriptDocument19 pagesAddiction ScriptLaica A. LunetaNo ratings yet
- Lecture 8 Central Nervous System CnsDocument35 pagesLecture 8 Central Nervous System CnsakramuddaulaNo ratings yet
- Presented By:-11081506 (Ridhi) 11081524 (Khushboo) 11081560 (Shiny) 11081542 (Sakshi)Document17 pagesPresented By:-11081506 (Ridhi) 11081524 (Khushboo) 11081560 (Shiny) 11081542 (Sakshi)Akanksha KapoorNo ratings yet
- Mechanism and Side Effects of SSRI 1Document13 pagesMechanism and Side Effects of SSRI 1Andika MetrisiawanNo ratings yet
- Frisium Knowledge ModuleDocument7 pagesFrisium Knowledge ModulesiddiqrehanNo ratings yet
- Elfani Nur Sita Augustina-19084Document6 pagesElfani Nur Sita Augustina-19084elfannynr augustinaNo ratings yet
- Anxiolytics Sedatives Hypnotics Pharm 3Document38 pagesAnxiolytics Sedatives Hypnotics Pharm 3Peter Harris100% (1)
- Ethical Use of CannabisDocument3 pagesEthical Use of CannabisMile PrikopNo ratings yet
- Drug Education and Vice ControlDocument25 pagesDrug Education and Vice ControlShan Jerome Lapuz SamoyNo ratings yet
- MDTH: Mood Disorders Treatment History FormDocument3 pagesMDTH: Mood Disorders Treatment History FormLaura ParkaNo ratings yet
- Chapter Overview: Psychoactive Drugs: Classification and HistoryDocument20 pagesChapter Overview: Psychoactive Drugs: Classification and HistorySiddharth soniNo ratings yet
- Annotated BibliographyDocument6 pagesAnnotated Bibliographyapi-451590039No ratings yet
- The State of U.S. Cannabis Laws, AbridgedDocument6 pagesThe State of U.S. Cannabis Laws, AbridgedPaul Marini100% (1)
- Cannabidiol (CBD)Document8 pagesCannabidiol (CBD)Isaias Sanches LopezNo ratings yet
- RA 9165 ComprehensiveDangerous Drugs Act of 2002 An Overview Presented ByCRIMINOLOGY INTERNDocument4 pagesRA 9165 ComprehensiveDangerous Drugs Act of 2002 An Overview Presented ByCRIMINOLOGY INTERNRaemmanlagradaNo ratings yet
- 2 Executive Order On BADACDocument8 pages2 Executive Order On BADACSto Niño PagadianNo ratings yet
- Sedative and HypnoticsDocument26 pagesSedative and HypnoticsZarish IftikharNo ratings yet
- Drug StudyDocument3 pagesDrug StudyJezen SucalitNo ratings yet
- Cannabinoid and Terpene InfoDocument2 pagesCannabinoid and Terpene Infosirwilliam1991No ratings yet
- Clinical AssignmentDocument22 pagesClinical AssignmentKeziah GillNo ratings yet
- BupropionDocument13 pagesBupropion18.10.1986No ratings yet
- PHR 302: Medicinal Chemistry-I: Sedative-Hypnotic DrugsDocument63 pagesPHR 302: Medicinal Chemistry-I: Sedative-Hypnotic Drugs53-Deepankar SutradharNo ratings yet
- Drugs: What Is A Drug??Document9 pagesDrugs: What Is A Drug??Alyzza BorrasNo ratings yet