
Tratamiento de La Violación
Tratamiento de La Violación
You might also like
- CAMI QuestionnaireDocument3 pagesCAMI QuestionnaireArifPutraD'cliquersNo ratings yet
- Clinical Manual of Psychosomatic Medicine A Guide To ConsultatiDocument565 pagesClinical Manual of Psychosomatic Medicine A Guide To ConsultatiDalal HazelNo ratings yet
- Evidence Based Treatments for Trauma-Related Psychological Disorders: A Practical Guide for CliniciansFrom EverandEvidence Based Treatments for Trauma-Related Psychological Disorders: A Practical Guide for CliniciansUlrich SchnyderNo ratings yet
- Clinical Manual of Adolescent Substance Abuse TreatmentDocument519 pagesClinical Manual of Adolescent Substance Abuse TreatmentKhúc Minh Kiên100% (1)
- Clinical Manual Preventioin MentalDocument440 pagesClinical Manual Preventioin MentalimilagiNo ratings yet
- NLP Trauma Recovery Manual 2011 PDFDocument49 pagesNLP Trauma Recovery Manual 2011 PDFdpscribdzone100% (2)
- Clinical Manual For AssesmentsDocument356 pagesClinical Manual For AssesmentsJoel Sandoval100% (5)
- Act 580 Counsellors Act 1998Document37 pagesAct 580 Counsellors Act 1998Adam Haida & CoNo ratings yet
- Psychotic Depression by SwartzDocument345 pagesPsychotic Depression by Swartz88888888100% (2)
- Psychology BooksDocument100 pagesPsychology BooksKarthick Ganesan21% (14)
- A8 Deconstructing A Definition Social Maladjustment Versus Emotional DisturbanceDocument13 pagesA8 Deconstructing A Definition Social Maladjustment Versus Emotional Disturbanceapi-260211648No ratings yet
- Bernhard 2016Document38 pagesBernhard 2016aviones123No ratings yet
- Battering Typologies, Attachment Insecurity, and Personality Disorders-A Comprehensive Literature ReviewDocument18 pagesBattering Typologies, Attachment Insecurity, and Personality Disorders-A Comprehensive Literature Reviewjulian gomez sosaNo ratings yet
- Whalen Lipko Document 2018Document69 pagesWhalen Lipko Document 2018Masih LoghmaniNo ratings yet
- Galano (2018) - ESDocument190 pagesGalano (2018) - ESLara Perez MurciaNo ratings yet
- Pres XX Posttraumatic Growth Review Zoeller and Maercker 2006Document28 pagesPres XX Posttraumatic Growth Review Zoeller and Maercker 2006Bianca DurkovicsNo ratings yet
- Combined Pharmacotherapy and Psychological Therapies For Post Traumatic Stress Disorder (PTSD) (Review)Document40 pagesCombined Pharmacotherapy and Psychological Therapies For Post Traumatic Stress Disorder (PTSD) (Review)Qwerty QwertyNo ratings yet
- Clinical Manual For AutismDocument337 pagesClinical Manual For AutismTatiana ValicaNo ratings yet
- PDF Clinical Manual For The Assessment and Treatment of Suicidal Patients Second Edition John Chiles Ebook Full ChapterDocument53 pagesPDF Clinical Manual For The Assessment and Treatment of Suicidal Patients Second Edition John Chiles Ebook Full Chapterjohn.griffin660100% (2)
- Sma14-4816 LitreviewDocument279 pagesSma14-4816 LitreviewDavid QatamadzeNo ratings yet
- Broken Laws, Broken Lives: Medical Evidence of Torture by US Personnel and Its ImpactDocument130 pagesBroken Laws, Broken Lives: Medical Evidence of Torture by US Personnel and Its ImpactSara ShafikNo ratings yet
- MentalDocument439 pagesMentalGeorge Macovei100% (1)
- NLP Trauma Recovery Manual 2011 PDFDocument49 pagesNLP Trauma Recovery Manual 2011 PDFdpscribdzone100% (1)
- SG3 - Case Analysis Manuscript - PTSD 1Document132 pagesSG3 - Case Analysis Manuscript - PTSD 1Karl Angelo MontanoNo ratings yet
- Diego Farren - Thesis ShortDocument85 pagesDiego Farren - Thesis ShortDiego RiedemannNo ratings yet
- Cognitive Processing TherapistDocument219 pagesCognitive Processing Therapistdrorgarbi100% (1)
- World Federation of Societies of Biological Psychiatry (WFSBP) Guidelines For Biological Treatment of Unipolar Depressive Disorders in Primary CareDocument38 pagesWorld Federation of Societies of Biological Psychiatry (WFSBP) Guidelines For Biological Treatment of Unipolar Depressive Disorders in Primary CareDorin DvornicNo ratings yet
- BRM Psy V11P1Document10 pagesBRM Psy V11P1simbawulaNo ratings yet
- Appi Books 9780890426807Document218 pagesAppi Books 9780890426807Heidy Bravo RamosNo ratings yet
- Twenge, Gentile, DeWall, Ma, Lacefield, & Schurtz (2010) PDFDocument10 pagesTwenge, Gentile, DeWall, Ma, Lacefield, & Schurtz (2010) PDFRicardo ZaidenbergNo ratings yet
- (Drug Text) - (PDF) - Drug War FactbookDocument120 pages(Drug Text) - (PDF) - Drug War FactbookMichael LasleyNo ratings yet
- Systematic Review of Suicidal Thoughts and Behaviors Among Police OfficersDocument20 pagesSystematic Review of Suicidal Thoughts and Behaviors Among Police OfficersBarbara SousaNo ratings yet
- 2018 ClinPsyD WhiteheadDocument162 pages2018 ClinPsyD Whitehead胡新No ratings yet
- NLP Trauma Recovery Manual 2011Document49 pagesNLP Trauma Recovery Manual 2011Francesco Fiorello100% (1)
- 2018 Trauma, Depression and Burnout in The Human Rights Field - Identifying Barriers and Pathways To Resilient AdvocacyDocument57 pages2018 Trauma, Depression and Burnout in The Human Rights Field - Identifying Barriers and Pathways To Resilient AdvocacyLuana SouzaNo ratings yet
- Proposed Treatment of Problematic Pornography Use - A Cognitive-BeDocument132 pagesProposed Treatment of Problematic Pornography Use - A Cognitive-BeFlávio Da Silva BorgesNo ratings yet
- Cognitive Dysfunction in Unipolar Depression ImplicationsDocument9 pagesCognitive Dysfunction in Unipolar Depression ImplicationsastrogliaNo ratings yet
- Clinicians Attitudes Towards Borderline Personality Disorder andDocument98 pagesClinicians Attitudes Towards Borderline Personality Disorder andsamoor00500No ratings yet
- Schema Therapy For Borderline Personality Disorder A Comprehensive Review of Its Empirical Foundations, Effectiveness and ImplementationDocument22 pagesSchema Therapy For Borderline Personality Disorder A Comprehensive Review of Its Empirical Foundations, Effectiveness and ImplementationMa Fernanda Claudio Sal100% (1)
- Encyclopedia BD Income-Associated BDDocument15 pagesEncyclopedia BD Income-Associated BDPeter MuennigNo ratings yet
- Psychiatric Symptoms in Caregivers of PaDocument12 pagesPsychiatric Symptoms in Caregivers of PaY FelixNo ratings yet
- Cyclophosphamide Versus Methylprednisolone For Treating Neuropsychiatric Involvement in Systemic Lupus Erythematosus (Review)Document33 pagesCyclophosphamide Versus Methylprednisolone For Treating Neuropsychiatric Involvement in Systemic Lupus Erythematosus (Review)Jocsi Barros HerreraNo ratings yet
- A Test of Self-Control Theory Using General Patterns of DevianceDocument105 pagesA Test of Self-Control Theory Using General Patterns of DevianceMuhammad Zakie ArfiansyahNo ratings yet
- 62136Document367 pages62136Todd AndersonNo ratings yet
- Narcissistic Borderline Disorders ReducedDocument253 pagesNarcissistic Borderline Disorders Reduceddebhon100% (16)
- Psychosocial and Pharmacological Treatments For Deliberate Self Harm (Review)Document44 pagesPsychosocial and Pharmacological Treatments For Deliberate Self Harm (Review)Rooney WillardNo ratings yet
- Study of International Students Definations of and PerceptionsDocument85 pagesStudy of International Students Definations of and PerceptionsMylene Joy A. PeñafloridaNo ratings yet
- Clinical Psychology Review: Alex M. Wood, Jeffrey J. Froh, Adam W.A. GeraghtyDocument16 pagesClinical Psychology Review: Alex M. Wood, Jeffrey J. Froh, Adam W.A. GeraghtyHDzung PhamNo ratings yet
- Kortikosteroid Utk TBMDocument66 pagesKortikosteroid Utk TBModellistaNo ratings yet
- Textbook Transgender Mental Health 1St Edition Eric Yarbrough Ebook All Chapter PDFDocument53 pagesTextbook Transgender Mental Health 1St Edition Eric Yarbrough Ebook All Chapter PDFbrittani.ibarra321100% (2)
- Pathological GamblingDocument287 pagesPathological GamblingSandro BrunoNo ratings yet
- (Files - Indowebster.com) - 4 Clinical ManualDocument337 pages(Files - Indowebster.com) - 4 Clinical ManualBangun Samudra UtamaNo ratings yet
- Gunter Whitt Al DisseminationDocument9 pagesGunter Whitt Al Disseminationgazellehouse8259No ratings yet
- Aggression and Violent BehaviorDocument11 pagesAggression and Violent Behaviorernie moreNo ratings yet
- Quick Reference Guide FallDocument62 pagesQuick Reference Guide FallKreshnik IdrizajNo ratings yet
- Neurobiology of Anxiety Disorders: Michael J. Meaney, Michael R. Liebowitz, and E. David LeonardoDocument43 pagesNeurobiology of Anxiety Disorders: Michael J. Meaney, Michael R. Liebowitz, and E. David LeonardoOscar René Hernández PérezNo ratings yet
- NFNTSX Handbook eDocument122 pagesNFNTSX Handbook eowaiskhan91No ratings yet
- Diagnostico Dual y Conducta CriminalDocument87 pagesDiagnostico Dual y Conducta CriminalEliana Orozco HenaoNo ratings yet
- Ketamine JaffdispubDocument12 pagesKetamine JaffdispubT Smith AndresNo ratings yet
- Mothers Who Kill The Forensic Use and JuDocument45 pagesMothers Who Kill The Forensic Use and JuUdruzenje PravnikaNo ratings yet
- Trick Ey 2012Document17 pagesTrick Ey 2012pikagaming838No ratings yet
- Worry and its Psychological Disorders: Theory, Assessment and TreatmentFrom EverandWorry and its Psychological Disorders: Theory, Assessment and TreatmentNo ratings yet
- Treatment of High-Risk Sexual Offenders: An Integrated ApproachFrom EverandTreatment of High-Risk Sexual Offenders: An Integrated ApproachNo ratings yet
- The Coach - Athlete Relationship QuestionnaireDocument38 pagesThe Coach - Athlete Relationship QuestionnaireMarco Antonio Aravena FernándezNo ratings yet
- Uso y Abuso de Alcohol y Drogas en Criminales Violentos Sexuales y No SexualesDocument12 pagesUso y Abuso de Alcohol y Drogas en Criminales Violentos Sexuales y No SexualesMarco Antonio Aravena FernándezNo ratings yet
- Combatiendo El FemicidioDocument2 pagesCombatiendo El FemicidioMarco Antonio Aravena FernándezNo ratings yet
- Evaluación Del Riesgo Suicida NiñosDocument6 pagesEvaluación Del Riesgo Suicida NiñosMarco Antonio Aravena FernándezNo ratings yet
- Mapping How Emotions Manifest in The BodyDocument4 pagesMapping How Emotions Manifest in The BodyMarco Antonio Aravena Fernández100% (1)
- Accepted Manuscript: Behavioural Brain ResearchDocument21 pagesAccepted Manuscript: Behavioural Brain ResearchPsiholog Monica StănescuNo ratings yet
- Sample Case Analysis UuDocument7 pagesSample Case Analysis UuLailiWafaNo ratings yet
- Executive Functioning, by Dr. Thomas BrownDocument6 pagesExecutive Functioning, by Dr. Thomas BrownDerekNo ratings yet
- Balint 1969Document8 pagesBalint 1969IsabelGuijarroMartinezNo ratings yet
- Dulcan's Textbook of Child and Adolescent Psychiatry Edited by Mina K. Dulcan, M.D.Document875 pagesDulcan's Textbook of Child and Adolescent Psychiatry Edited by Mina K. Dulcan, M.D.farhanNo ratings yet
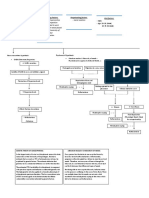
- Predisposing Factors: Precipitating Factors: Perpetuating Factors: Risk FactorsDocument3 pagesPredisposing Factors: Precipitating Factors: Perpetuating Factors: Risk FactorsRein TamayoNo ratings yet
- Pathological LyingDocument14 pagesPathological LyingDanielaNo ratings yet
- Psychiatry Paper-I: Final Exam National Board of Examinations December 2020Document1 pagePsychiatry Paper-I: Final Exam National Board of Examinations December 2020isbegin. comNo ratings yet
- Contaminated Aircraft AirDocument8 pagesContaminated Aircraft AirDhananjaya HathurusingheNo ratings yet
- Learning Insights Related To Nursing PracticeDocument2 pagesLearning Insights Related To Nursing Practicezhekinangene100% (4)
- Defense Mechanisms:: (Type Here)Document4 pagesDefense Mechanisms:: (Type Here)Hack MeNo ratings yet
- Reuben M. Mwangi, PH.D., LPC, CAADC: Mwang1r@cmich - EduDocument7 pagesReuben M. Mwangi, PH.D., LPC, CAADC: Mwang1r@cmich - Eduapi-5234606860% (1)
- Journal 9Document18 pagesJournal 9ameraizahNo ratings yet
- Hallucinations in ChildrenDocument9 pagesHallucinations in ChildrenEnda RafiqohNo ratings yet
- Psychiatric Emergencies What Do I Do Now Emergency Medicine Eileen Baker All ChapterDocument67 pagesPsychiatric Emergencies What Do I Do Now Emergency Medicine Eileen Baker All Chapterrita.rolf773100% (6)
- Social Emotional HealthDocument7 pagesSocial Emotional HealthAdel SaNo ratings yet
- Psychiatric EmergencyDocument11 pagesPsychiatric EmergencyShradha100% (1)
- Passing The MRCPsych v11Document6 pagesPassing The MRCPsych v11sayed Alpha100% (1)
- Psychology FraudDocument32 pagesPsychology FraudJuan JeannitonNo ratings yet
- Bipolar Disorder 3eDocument302 pagesBipolar Disorder 3eahmustNo ratings yet
- Addiction CaseDocument4 pagesAddiction CasePooja VarmaNo ratings yet
- FC Child-Adolescent Intake Forms Fisa AdolescentDocument4 pagesFC Child-Adolescent Intake Forms Fisa Adolescentnicoletagr2744No ratings yet
- Voluntary AdmissionDocument1 pageVoluntary Admissionapi-414703292No ratings yet
- Ghazban A 10 1541 1 1591fe7Document11 pagesGhazban A 10 1541 1 1591fe7Adila amalitaNo ratings yet
- EMDR Grief and MourningDocument14 pagesEMDR Grief and MourningMarta Martínez Palmer100% (2)

























































































Download as pdf or txt
You might also like
- CAMI QuestionnaireDocument3 pagesCAMI QuestionnaireArifPutraD'cliquersNo ratings yet
- Clinical Manual of Psychosomatic Medicine A Guide To ConsultatiDocument565 pagesClinical Manual of Psychosomatic Medicine A Guide To ConsultatiDalal HazelNo ratings yet
- Evidence Based Treatments for Trauma-Related Psychological Disorders: A Practical Guide for CliniciansFrom EverandEvidence Based Treatments for Trauma-Related Psychological Disorders: A Practical Guide for CliniciansUlrich SchnyderNo ratings yet
- Clinical Manual of Adolescent Substance Abuse TreatmentDocument519 pagesClinical Manual of Adolescent Substance Abuse TreatmentKhúc Minh Kiên100% (1)
- Clinical Manual Preventioin MentalDocument440 pagesClinical Manual Preventioin MentalimilagiNo ratings yet
- NLP Trauma Recovery Manual 2011 PDFDocument49 pagesNLP Trauma Recovery Manual 2011 PDFdpscribdzone100% (2)
- Clinical Manual For AssesmentsDocument356 pagesClinical Manual For AssesmentsJoel Sandoval100% (5)
- Act 580 Counsellors Act 1998Document37 pagesAct 580 Counsellors Act 1998Adam Haida & CoNo ratings yet
- Psychotic Depression by SwartzDocument345 pagesPsychotic Depression by Swartz88888888100% (2)
- Psychology BooksDocument100 pagesPsychology BooksKarthick Ganesan21% (14)
- A8 Deconstructing A Definition Social Maladjustment Versus Emotional DisturbanceDocument13 pagesA8 Deconstructing A Definition Social Maladjustment Versus Emotional Disturbanceapi-260211648No ratings yet
- Bernhard 2016Document38 pagesBernhard 2016aviones123No ratings yet
- Battering Typologies, Attachment Insecurity, and Personality Disorders-A Comprehensive Literature ReviewDocument18 pagesBattering Typologies, Attachment Insecurity, and Personality Disorders-A Comprehensive Literature Reviewjulian gomez sosaNo ratings yet
- Whalen Lipko Document 2018Document69 pagesWhalen Lipko Document 2018Masih LoghmaniNo ratings yet
- Galano (2018) - ESDocument190 pagesGalano (2018) - ESLara Perez MurciaNo ratings yet
- Pres XX Posttraumatic Growth Review Zoeller and Maercker 2006Document28 pagesPres XX Posttraumatic Growth Review Zoeller and Maercker 2006Bianca DurkovicsNo ratings yet
- Combined Pharmacotherapy and Psychological Therapies For Post Traumatic Stress Disorder (PTSD) (Review)Document40 pagesCombined Pharmacotherapy and Psychological Therapies For Post Traumatic Stress Disorder (PTSD) (Review)Qwerty QwertyNo ratings yet
- Clinical Manual For AutismDocument337 pagesClinical Manual For AutismTatiana ValicaNo ratings yet
- PDF Clinical Manual For The Assessment and Treatment of Suicidal Patients Second Edition John Chiles Ebook Full ChapterDocument53 pagesPDF Clinical Manual For The Assessment and Treatment of Suicidal Patients Second Edition John Chiles Ebook Full Chapterjohn.griffin660100% (2)
- Sma14-4816 LitreviewDocument279 pagesSma14-4816 LitreviewDavid QatamadzeNo ratings yet
- Broken Laws, Broken Lives: Medical Evidence of Torture by US Personnel and Its ImpactDocument130 pagesBroken Laws, Broken Lives: Medical Evidence of Torture by US Personnel and Its ImpactSara ShafikNo ratings yet
- MentalDocument439 pagesMentalGeorge Macovei100% (1)
- NLP Trauma Recovery Manual 2011 PDFDocument49 pagesNLP Trauma Recovery Manual 2011 PDFdpscribdzone100% (1)
- SG3 - Case Analysis Manuscript - PTSD 1Document132 pagesSG3 - Case Analysis Manuscript - PTSD 1Karl Angelo MontanoNo ratings yet
- Diego Farren - Thesis ShortDocument85 pagesDiego Farren - Thesis ShortDiego RiedemannNo ratings yet
- Cognitive Processing TherapistDocument219 pagesCognitive Processing Therapistdrorgarbi100% (1)
- World Federation of Societies of Biological Psychiatry (WFSBP) Guidelines For Biological Treatment of Unipolar Depressive Disorders in Primary CareDocument38 pagesWorld Federation of Societies of Biological Psychiatry (WFSBP) Guidelines For Biological Treatment of Unipolar Depressive Disorders in Primary CareDorin DvornicNo ratings yet
- BRM Psy V11P1Document10 pagesBRM Psy V11P1simbawulaNo ratings yet
- Appi Books 9780890426807Document218 pagesAppi Books 9780890426807Heidy Bravo RamosNo ratings yet
- Twenge, Gentile, DeWall, Ma, Lacefield, & Schurtz (2010) PDFDocument10 pagesTwenge, Gentile, DeWall, Ma, Lacefield, & Schurtz (2010) PDFRicardo ZaidenbergNo ratings yet
- (Drug Text) - (PDF) - Drug War FactbookDocument120 pages(Drug Text) - (PDF) - Drug War FactbookMichael LasleyNo ratings yet
- Systematic Review of Suicidal Thoughts and Behaviors Among Police OfficersDocument20 pagesSystematic Review of Suicidal Thoughts and Behaviors Among Police OfficersBarbara SousaNo ratings yet
- 2018 ClinPsyD WhiteheadDocument162 pages2018 ClinPsyD Whitehead胡新No ratings yet
- NLP Trauma Recovery Manual 2011Document49 pagesNLP Trauma Recovery Manual 2011Francesco Fiorello100% (1)
- 2018 Trauma, Depression and Burnout in The Human Rights Field - Identifying Barriers and Pathways To Resilient AdvocacyDocument57 pages2018 Trauma, Depression and Burnout in The Human Rights Field - Identifying Barriers and Pathways To Resilient AdvocacyLuana SouzaNo ratings yet
- Proposed Treatment of Problematic Pornography Use - A Cognitive-BeDocument132 pagesProposed Treatment of Problematic Pornography Use - A Cognitive-BeFlávio Da Silva BorgesNo ratings yet
- Cognitive Dysfunction in Unipolar Depression ImplicationsDocument9 pagesCognitive Dysfunction in Unipolar Depression ImplicationsastrogliaNo ratings yet
- Clinicians Attitudes Towards Borderline Personality Disorder andDocument98 pagesClinicians Attitudes Towards Borderline Personality Disorder andsamoor00500No ratings yet
- Schema Therapy For Borderline Personality Disorder A Comprehensive Review of Its Empirical Foundations, Effectiveness and ImplementationDocument22 pagesSchema Therapy For Borderline Personality Disorder A Comprehensive Review of Its Empirical Foundations, Effectiveness and ImplementationMa Fernanda Claudio Sal100% (1)
- Encyclopedia BD Income-Associated BDDocument15 pagesEncyclopedia BD Income-Associated BDPeter MuennigNo ratings yet
- Psychiatric Symptoms in Caregivers of PaDocument12 pagesPsychiatric Symptoms in Caregivers of PaY FelixNo ratings yet
- Cyclophosphamide Versus Methylprednisolone For Treating Neuropsychiatric Involvement in Systemic Lupus Erythematosus (Review)Document33 pagesCyclophosphamide Versus Methylprednisolone For Treating Neuropsychiatric Involvement in Systemic Lupus Erythematosus (Review)Jocsi Barros HerreraNo ratings yet
- A Test of Self-Control Theory Using General Patterns of DevianceDocument105 pagesA Test of Self-Control Theory Using General Patterns of DevianceMuhammad Zakie ArfiansyahNo ratings yet
- 62136Document367 pages62136Todd AndersonNo ratings yet
- Narcissistic Borderline Disorders ReducedDocument253 pagesNarcissistic Borderline Disorders Reduceddebhon100% (16)
- Psychosocial and Pharmacological Treatments For Deliberate Self Harm (Review)Document44 pagesPsychosocial and Pharmacological Treatments For Deliberate Self Harm (Review)Rooney WillardNo ratings yet
- Study of International Students Definations of and PerceptionsDocument85 pagesStudy of International Students Definations of and PerceptionsMylene Joy A. PeñafloridaNo ratings yet
- Clinical Psychology Review: Alex M. Wood, Jeffrey J. Froh, Adam W.A. GeraghtyDocument16 pagesClinical Psychology Review: Alex M. Wood, Jeffrey J. Froh, Adam W.A. GeraghtyHDzung PhamNo ratings yet
- Kortikosteroid Utk TBMDocument66 pagesKortikosteroid Utk TBModellistaNo ratings yet
- Textbook Transgender Mental Health 1St Edition Eric Yarbrough Ebook All Chapter PDFDocument53 pagesTextbook Transgender Mental Health 1St Edition Eric Yarbrough Ebook All Chapter PDFbrittani.ibarra321100% (2)
- Pathological GamblingDocument287 pagesPathological GamblingSandro BrunoNo ratings yet
- (Files - Indowebster.com) - 4 Clinical ManualDocument337 pages(Files - Indowebster.com) - 4 Clinical ManualBangun Samudra UtamaNo ratings yet
- Gunter Whitt Al DisseminationDocument9 pagesGunter Whitt Al Disseminationgazellehouse8259No ratings yet
- Aggression and Violent BehaviorDocument11 pagesAggression and Violent Behaviorernie moreNo ratings yet
- Quick Reference Guide FallDocument62 pagesQuick Reference Guide FallKreshnik IdrizajNo ratings yet
- Neurobiology of Anxiety Disorders: Michael J. Meaney, Michael R. Liebowitz, and E. David LeonardoDocument43 pagesNeurobiology of Anxiety Disorders: Michael J. Meaney, Michael R. Liebowitz, and E. David LeonardoOscar René Hernández PérezNo ratings yet
- NFNTSX Handbook eDocument122 pagesNFNTSX Handbook eowaiskhan91No ratings yet
- Diagnostico Dual y Conducta CriminalDocument87 pagesDiagnostico Dual y Conducta CriminalEliana Orozco HenaoNo ratings yet
- Ketamine JaffdispubDocument12 pagesKetamine JaffdispubT Smith AndresNo ratings yet
- Mothers Who Kill The Forensic Use and JuDocument45 pagesMothers Who Kill The Forensic Use and JuUdruzenje PravnikaNo ratings yet
- Trick Ey 2012Document17 pagesTrick Ey 2012pikagaming838No ratings yet
- Worry and its Psychological Disorders: Theory, Assessment and TreatmentFrom EverandWorry and its Psychological Disorders: Theory, Assessment and TreatmentNo ratings yet
- Treatment of High-Risk Sexual Offenders: An Integrated ApproachFrom EverandTreatment of High-Risk Sexual Offenders: An Integrated ApproachNo ratings yet
- The Coach - Athlete Relationship QuestionnaireDocument38 pagesThe Coach - Athlete Relationship QuestionnaireMarco Antonio Aravena FernándezNo ratings yet
- Uso y Abuso de Alcohol y Drogas en Criminales Violentos Sexuales y No SexualesDocument12 pagesUso y Abuso de Alcohol y Drogas en Criminales Violentos Sexuales y No SexualesMarco Antonio Aravena FernándezNo ratings yet
- Combatiendo El FemicidioDocument2 pagesCombatiendo El FemicidioMarco Antonio Aravena FernándezNo ratings yet
- Evaluación Del Riesgo Suicida NiñosDocument6 pagesEvaluación Del Riesgo Suicida NiñosMarco Antonio Aravena FernándezNo ratings yet
- Mapping How Emotions Manifest in The BodyDocument4 pagesMapping How Emotions Manifest in The BodyMarco Antonio Aravena Fernández100% (1)
- Accepted Manuscript: Behavioural Brain ResearchDocument21 pagesAccepted Manuscript: Behavioural Brain ResearchPsiholog Monica StănescuNo ratings yet
- Sample Case Analysis UuDocument7 pagesSample Case Analysis UuLailiWafaNo ratings yet
- Executive Functioning, by Dr. Thomas BrownDocument6 pagesExecutive Functioning, by Dr. Thomas BrownDerekNo ratings yet
- Balint 1969Document8 pagesBalint 1969IsabelGuijarroMartinezNo ratings yet
- Dulcan's Textbook of Child and Adolescent Psychiatry Edited by Mina K. Dulcan, M.D.Document875 pagesDulcan's Textbook of Child and Adolescent Psychiatry Edited by Mina K. Dulcan, M.D.farhanNo ratings yet
- Predisposing Factors: Precipitating Factors: Perpetuating Factors: Risk FactorsDocument3 pagesPredisposing Factors: Precipitating Factors: Perpetuating Factors: Risk FactorsRein TamayoNo ratings yet
- Pathological LyingDocument14 pagesPathological LyingDanielaNo ratings yet
- Psychiatry Paper-I: Final Exam National Board of Examinations December 2020Document1 pagePsychiatry Paper-I: Final Exam National Board of Examinations December 2020isbegin. comNo ratings yet
- Contaminated Aircraft AirDocument8 pagesContaminated Aircraft AirDhananjaya HathurusingheNo ratings yet
- Learning Insights Related To Nursing PracticeDocument2 pagesLearning Insights Related To Nursing Practicezhekinangene100% (4)
- Defense Mechanisms:: (Type Here)Document4 pagesDefense Mechanisms:: (Type Here)Hack MeNo ratings yet
- Reuben M. Mwangi, PH.D., LPC, CAADC: Mwang1r@cmich - EduDocument7 pagesReuben M. Mwangi, PH.D., LPC, CAADC: Mwang1r@cmich - Eduapi-5234606860% (1)
- Journal 9Document18 pagesJournal 9ameraizahNo ratings yet
- Hallucinations in ChildrenDocument9 pagesHallucinations in ChildrenEnda RafiqohNo ratings yet
- Psychiatric Emergencies What Do I Do Now Emergency Medicine Eileen Baker All ChapterDocument67 pagesPsychiatric Emergencies What Do I Do Now Emergency Medicine Eileen Baker All Chapterrita.rolf773100% (6)
- Social Emotional HealthDocument7 pagesSocial Emotional HealthAdel SaNo ratings yet
- Psychiatric EmergencyDocument11 pagesPsychiatric EmergencyShradha100% (1)
- Passing The MRCPsych v11Document6 pagesPassing The MRCPsych v11sayed Alpha100% (1)
- Psychology FraudDocument32 pagesPsychology FraudJuan JeannitonNo ratings yet
- Bipolar Disorder 3eDocument302 pagesBipolar Disorder 3eahmustNo ratings yet
- Addiction CaseDocument4 pagesAddiction CasePooja VarmaNo ratings yet
- FC Child-Adolescent Intake Forms Fisa AdolescentDocument4 pagesFC Child-Adolescent Intake Forms Fisa Adolescentnicoletagr2744No ratings yet
- Voluntary AdmissionDocument1 pageVoluntary Admissionapi-414703292No ratings yet
- Ghazban A 10 1541 1 1591fe7Document11 pagesGhazban A 10 1541 1 1591fe7Adila amalitaNo ratings yet
- EMDR Grief and MourningDocument14 pagesEMDR Grief and MourningMarta Martínez Palmer100% (2)