Download as pdf or txt
You might also like
- Diagnostic Exam Nov 24Document25 pagesDiagnostic Exam Nov 24genita.keziahandrea100% (1)
- JCB Backhoe Loader JCB 3cx 4cx 5cx Service ManualDocument22 pagesJCB Backhoe Loader JCB 3cx 4cx 5cx Service Manualianclements260586qfi100% (129)
- Paediatric Clerking Sheet PDF Clinical Medicine Diseases and DisordersDocument1 pagePaediatric Clerking Sheet PDF Clinical Medicine Diseases and DisordersSITI AISYATUL ATHIRAH RUSNANNo ratings yet
- Clinical Toxicology 2013 CompleteDocument364 pagesClinical Toxicology 2013 Completenuttiya_w3294No ratings yet
- Essential Clinical Cases GP TraineesDocument3 pagesEssential Clinical Cases GP TraineesTahir AliNo ratings yet
- CH 20 Manter Gatz S Essentials of Clinical Neuroanatomy and NeurophysiologyDocument27 pagesCH 20 Manter Gatz S Essentials of Clinical Neuroanatomy and Neurophysiologyasarg214100% (1)
- Case PediatricsDocument6 pagesCase PediatricsHarsh NimavatNo ratings yet
- Pancytopenia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandPancytopenia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Diabetic Nephropathy, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandDiabetic Nephropathy, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Hypercalcemia, (High Blood Calcium) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHypercalcemia, (High Blood Calcium) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Drug-Induced Liver InjuryDocument26 pagesDrug-Induced Liver InjuryUsamaNo ratings yet
- GastritisDocument32 pagesGastritisDian Ekawati100% (2)
- Approach To Chronic DiarrheaDocument40 pagesApproach To Chronic DiarrheaJheng-Dao YangNo ratings yet
- JNC 8Document40 pagesJNC 8Nadira Wulandari100% (1)
- Medical Case 1: Language Centre of Malahayati University at 2010Document16 pagesMedical Case 1: Language Centre of Malahayati University at 2010putri1114No ratings yet
- GERIATRIC MEDICINE (Basic)Document41 pagesGERIATRIC MEDICINE (Basic)Medical AdvicesNo ratings yet
- GP Reg - Asthma and Spirometry 2011Document114 pagesGP Reg - Asthma and Spirometry 2011minerva_stanciuNo ratings yet
- Chest Pain PresentationDocument24 pagesChest Pain PresentationAnonymous 17awurSUNo ratings yet
- Nephrotic Syndrome in Children: January 2013Document7 pagesNephrotic Syndrome in Children: January 2013molenNo ratings yet
- Classification of Anemias: What Is Anemia, How Do You Diagnose Anemia, and How Are The Different Anemias Classified?Document78 pagesClassification of Anemias: What Is Anemia, How Do You Diagnose Anemia, and How Are The Different Anemias Classified?Kaushik Bhuva100% (1)
- Textbook Part 1Document89 pagesTextbook Part 1CY Onuorah100% (1)
- 2018 Severe Cutaneous Adverse Drug Reactions - Presentation, Risk Factors, and ManagementDocument9 pages2018 Severe Cutaneous Adverse Drug Reactions - Presentation, Risk Factors, and ManagementpablopabloortizortizNo ratings yet
- Kidney TransplantDocument11 pagesKidney TransplantPrincess Xzmae RamirezNo ratings yet
- Set 1 Checked: E. Pathological ConditionDocument60 pagesSet 1 Checked: E. Pathological ConditionKunal BhamareNo ratings yet
- A Practical Approach To Managing Patients With Myasthenia GravisDocument16 pagesA Practical Approach To Managing Patients With Myasthenia GravisStevanie SesiliaNo ratings yet
- #9 Ie 8 PDFDocument8 pages#9 Ie 8 PDFOmar BasimNo ratings yet
- Sample Case ScenarioDocument10 pagesSample Case ScenarioKarilee Salcedo AyunayunNo ratings yet
- Diagnostic Liver Biopsy PDFDocument7 pagesDiagnostic Liver Biopsy PDFAriadna MarielNo ratings yet
- SGD Case Presentation 8Document34 pagesSGD Case Presentation 8Karen C. Del Rosario100% (1)
- Emergencymedicine Evaluationandmanagement Ofanemia: Brit Long,, Alex KoyfmanDocument22 pagesEmergencymedicine Evaluationandmanagement Ofanemia: Brit Long,, Alex KoyfmanCarlos Alberto Torres LópezNo ratings yet
- ICD 10 Codes For HIVDocument2 pagesICD 10 Codes For HIVmahi50No ratings yet
- 5 MED 4 - Approach To GI BleedingDocument6 pages5 MED 4 - Approach To GI BleedingIan CruzNo ratings yet
- Venous ThromboembolismDocument49 pagesVenous Thromboembolismadamu mohammadNo ratings yet
- Ecginami 111115073242 Phpapp02Document104 pagesEcginami 111115073242 Phpapp02ginaul100% (1)
- Hyperthyroidism: by TemesgenDocument33 pagesHyperthyroidism: by TemesgenTemesgen100% (2)
- GI Exam (RCT)Document6 pagesGI Exam (RCT)kenners100% (11)
- DRESS Syndrome A Detailed InsightDocument12 pagesDRESS Syndrome A Detailed InsightLeba SouloungerNo ratings yet
- Breast Milk Jaundice - JPG 2Document13 pagesBreast Milk Jaundice - JPG 2asmaaNo ratings yet
- Core Topics in Internal MedicineDocument4 pagesCore Topics in Internal MedicineKristina Anne CoNo ratings yet
- Acute Kidney InjuryDocument15 pagesAcute Kidney InjuryManish VijayNo ratings yet
- Prepared by Inzar Yasin Ammar LabibDocument47 pagesPrepared by Inzar Yasin Ammar LabibJohn Clements Galiza100% (1)
- MCQDocument33 pagesMCQSean Purrier50% (2)
- Renovascular Hypertension: Department of Vascular Interventional Radiology Kem HospitalDocument45 pagesRenovascular Hypertension: Department of Vascular Interventional Radiology Kem Hospitalamrita narangNo ratings yet
- PericarditisDocument29 pagesPericarditisPavin KumarNo ratings yet
- Descending ParalysisDocument7 pagesDescending ParalysisgianpinotNo ratings yet
- COPD Differential Diagnosis ModuleDocument44 pagesCOPD Differential Diagnosis ModulenicusoorNo ratings yet
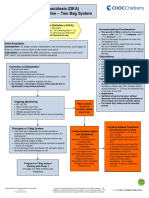
- Diabetic Ketoacidosis Care GuidelineDocument5 pagesDiabetic Ketoacidosis Care GuidelineRahma DhNo ratings yet
- Acute Liver FailureDocument69 pagesAcute Liver FailureAsif.N.IqbalNo ratings yet
- Preventive CardiologyDocument28 pagesPreventive CardiologyerizonNo ratings yet
- Neonatal Jaundice NotesDocument5 pagesNeonatal Jaundice NotesEros CuestaNo ratings yet
- Approach To Septic ShockDocument16 pagesApproach To Septic ShockRaja EllysyaNo ratings yet
- Corrosive PoisoningDocument4 pagesCorrosive PoisoningaBay AesculapianoNo ratings yet
- 620 General Internal MedicineDocument18 pages620 General Internal Medicinesteven rioNo ratings yet
- ERC Guidelines 2005Document186 pagesERC Guidelines 2005api-3743776No ratings yet
- CPT Case 4 PneumoniaDocument7 pagesCPT Case 4 PneumoniaAskine Jiezl Ico TadeoNo ratings yet
- Shock, Sirs & ModsDocument37 pagesShock, Sirs & ModsambitioustamannaNo ratings yet
- Psychiatry Chapter 3Document54 pagesPsychiatry Chapter 3Online Money In EthiopiaNo ratings yet
- MRCPI Combined General Medicine Regulations 2018Document32 pagesMRCPI Combined General Medicine Regulations 2018Shoukat MirzaNo ratings yet
- 7 Clinical History Taking and Physical Examination in Medical Practice in AfricaDocument3 pages7 Clinical History Taking and Physical Examination in Medical Practice in AfricaStephanie CalleNo ratings yet
- Surgery Ospe 322Document322 pagesSurgery Ospe 322fbf50269No ratings yet
- Cardiac EmergenciesDocument26 pagesCardiac Emergenciespreet kaurNo ratings yet
- IM NotesDocument74 pagesIM NotesRashed ShatnawiNo ratings yet
- Belle Preterm BirthDocument9 pagesBelle Preterm BirthRashed ShatnawiNo ratings yet
- Obsandgyne Tables 200pagesDocument221 pagesObsandgyne Tables 200pagesRashed ShatnawiNo ratings yet
- Belle Shoulder DystociaDocument2 pagesBelle Shoulder DystociaRashed ShatnawiNo ratings yet
- Belle Instruments For OGDocument1 pageBelle Instruments For OGRashed ShatnawiNo ratings yet
- Endometrial Carcinoma Malignant Lesions of The Body of UterusDocument3 pagesEndometrial Carcinoma Malignant Lesions of The Body of UterusRashed ShatnawiNo ratings yet
- Fibroids Frequency Race Age AnatomyDocument4 pagesFibroids Frequency Race Age AnatomyRashed ShatnawiNo ratings yet
- (Belle) Diabetes in PregnancyDocument3 pages(Belle) Diabetes in PregnancyAray Al-AfiqahNo ratings yet
- Belle Cervical DiseaseDocument7 pagesBelle Cervical DiseaseRashed ShatnawiNo ratings yet
- Najmd V1 1009Document4 pagesNajmd V1 1009merliaNo ratings yet
- Acute Respiratory Distress SyndromeDocument17 pagesAcute Respiratory Distress SyndromeSherree Hayes100% (3)
- What Are Age-Specific Competencies?: Meets JCAHO Standards!Document18 pagesWhat Are Age-Specific Competencies?: Meets JCAHO Standards!itsmekringNo ratings yet
- Dietary Protein Supplementation in The Elderly For Limiting Muscle Mass LossDocument15 pagesDietary Protein Supplementation in The Elderly For Limiting Muscle Mass LossAndres Felipe Quimbayo CifuentesNo ratings yet
- Antenatal HandoutDocument16 pagesAntenatal HandoutZahNo ratings yet
- Notification 2017 FDA & SdaDocument43 pagesNotification 2017 FDA & SdaPinnam MallikarjunaNo ratings yet
- Historical Development, Trends & Issues in CardiologyDocument13 pagesHistorical Development, Trends & Issues in CardiologysoniaNo ratings yet
- SLCN Gazette Magazine, Volume 1, Issue 1, 2019Document20 pagesSLCN Gazette Magazine, Volume 1, Issue 1, 2019Mayzelle RizNo ratings yet
- Jurnal Carpal Tunnel SyndromeDocument11 pagesJurnal Carpal Tunnel SyndromeArjuna MarzaNo ratings yet
- Plabable-Gems-20. Epidemiology Plabable GemsDocument32 pagesPlabable-Gems-20. Epidemiology Plabable GemsKhalid HabibNo ratings yet
- Saito 2015Document5 pagesSaito 2015didingNo ratings yet
- Biochem 322-Final 2005Document1 pageBiochem 322-Final 2005api-3763291No ratings yet
- Sim Medium 2 (English)Document2 pagesSim Medium 2 (English)TheLobitoNo ratings yet
- Molecular Biology BT401: BiotechnologyDocument12 pagesMolecular Biology BT401: BiotechnologyVivek GuptaNo ratings yet
- Oxidative Phosphorylation Glycolysis: 2 Phosphates Krebs/citric/TCA Cycle: 1 PhosphateDocument17 pagesOxidative Phosphorylation Glycolysis: 2 Phosphates Krebs/citric/TCA Cycle: 1 PhosphatereeNo ratings yet
- The Five TibetansDocument12 pagesThe Five TibetansKarhysNo ratings yet
- Jaeger ChartDocument2 pagesJaeger ChartDavid Andres Cañas Suarez100% (1)
- Fam Care PlanDocument3 pagesFam Care PlanGraiLe Joy Palbusa Ngina-BadayNo ratings yet
- Cardiovascula R Imaging: Dept. of Diagnostic Radiology Diponegoro Univ./Dr - Kariadi General HospitalDocument85 pagesCardiovascula R Imaging: Dept. of Diagnostic Radiology Diponegoro Univ./Dr - Kariadi General HospitalvaniaNo ratings yet
- Ethical Considerations in Research 2Document9 pagesEthical Considerations in Research 2muhendaaron33No ratings yet
- Sore Throat TreatmentsDocument16 pagesSore Throat Treatmentskuldip1951100% (1)
- Journal of Scleroderma and Related Disorders: Authorship Change FormDocument1 pageJournal of Scleroderma and Related Disorders: Authorship Change FormYaraNo ratings yet
- 8-1-11 - Pig Heart Dissection - LessonDocument7 pages8-1-11 - Pig Heart Dissection - LessonJoan NicoleNo ratings yet
- 7 Healing Oils: Found in The BibleDocument10 pages7 Healing Oils: Found in The BibleJacqueline100% (1)
- Midline DiastemaDocument4 pagesMidline DiastemasmritiNo ratings yet
- CREATIVE FOLK DANCE 2023 Criteri For JudgingDocument4 pagesCREATIVE FOLK DANCE 2023 Criteri For Judgingivy macalaladNo ratings yet