Download as pdf or txt
You might also like
- Mechanical Ventilation Made EasyDocument5 pagesMechanical Ventilation Made EasypraveenbhavniNo ratings yet
- 5fcdfd7d3d29a PDFDocument177 pages5fcdfd7d3d29a PDFAnamika100% (1)
- Iabp PosterDocument2 pagesIabp PosterRaghavendra Prasad100% (2)
- Burn Manual PDFDocument56 pagesBurn Manual PDFBea Valerio100% (1)
- Small Animal Cardiopulmonary Medicine - Wendy A. WareDocument289 pagesSmall Animal Cardiopulmonary Medicine - Wendy A. WareCarla Ester100% (2)
- Obstetrical Nursing Practice ExamDocument11 pagesObstetrical Nursing Practice Examstuffednurse83% (12)
- Small Animal Cardiology PDFDocument208 pagesSmall Animal Cardiology PDFRoberto AmpueroNo ratings yet
- Hemodynamic MonitoringDocument111 pagesHemodynamic MonitoringVenkatesan AnnamalaiNo ratings yet
- Cardiac CycleDocument2 pagesCardiac CyclevamshidhNo ratings yet
- Co 2019 Controle Glicemico IntDocument8 pagesCo 2019 Controle Glicemico InthauhauNo ratings yet
- Intra Aortic Balloon Pump (IABP) 2009Document57 pagesIntra Aortic Balloon Pump (IABP) 2009nurminsyahNo ratings yet
- J Clin Endocrinol Metab. 2012 97 16 38Document23 pagesJ Clin Endocrinol Metab. 2012 97 16 38rizwan234No ratings yet
- IABC Intra Aortic Balloon Counter Pulsation Nicvd PresentationDocument54 pagesIABC Intra Aortic Balloon Counter Pulsation Nicvd PresentationNavojit Chowdhury100% (1)
- The Cardiac CycleDocument9 pagesThe Cardiac CycleKaylababy Hamilton BlackNo ratings yet
- Cerebral Spinal Fluid & The MeningesDocument25 pagesCerebral Spinal Fluid & The MeningeschintyamontangNo ratings yet
- Swan Ganz FinalDocument36 pagesSwan Ganz FinalDanial HassanNo ratings yet
- Heart MuscleDocument10 pagesHeart Muscle22194No ratings yet
- Assessment and Treatment of Hyperglycemia in Critically IllDocument6 pagesAssessment and Treatment of Hyperglycemia in Critically IllYousif ElmasryNo ratings yet
- Vasoactive TherapyDocument26 pagesVasoactive Therapylidya agustin100% (1)
- Basic EP IntervalsDocument13 pagesBasic EP IntervalsdrharoonmohdNo ratings yet
- Cardiac Output Monitoring Mark VivianDocument32 pagesCardiac Output Monitoring Mark VivianpritaNo ratings yet
- Sinus Node DysfunctionDocument11 pagesSinus Node DysfunctionVasishta Nadella100% (1)
- Anaphylaxis For AnaesthetistsDocument14 pagesAnaphylaxis For AnaesthetistsJoe Wild100% (1)
- Liverpool Ni Modi PineDocument5 pagesLiverpool Ni Modi Pinerachmat fajar noor kNo ratings yet
- Ventilator Weaning and Spontaneous Breathing Trials An Educational Review 2016Document7 pagesVentilator Weaning and Spontaneous Breathing Trials An Educational Review 2016Tarran PhagooNo ratings yet
- The Alveolar Gas EquationDocument4 pagesThe Alveolar Gas Equationstewart_fNo ratings yet
- Drug Guideline Title: Remifentanil: SummaryDocument11 pagesDrug Guideline Title: Remifentanil: SummaryyafetNo ratings yet
- Henry Edmund Gaskin Boyle: Compiled by Department of Anaesthesia, DR - Psims & RFDocument10 pagesHenry Edmund Gaskin Boyle: Compiled by Department of Anaesthesia, DR - Psims & RFMinaz PatelNo ratings yet
- Cardiac Action PotentialDocument41 pagesCardiac Action PotentialRadijska Postaja KoprivnicaNo ratings yet
- HUTTDocument25 pagesHUTTdrdj14100% (1)
- Acid Base Equilibrium, Clinical Concepts and Acid Base DisordersDocument64 pagesAcid Base Equilibrium, Clinical Concepts and Acid Base DisordersevanNo ratings yet
- Blood Pressure Regulation-2Document40 pagesBlood Pressure Regulation-2Juliza FelicianoNo ratings yet
- Echocardiography in ShockDocument7 pagesEchocardiography in ShockRaul ForjanNo ratings yet
- Difficult Weaning From Cardiopulmonary Bypass Final Edit LiaDocument41 pagesDifficult Weaning From Cardiopulmonary Bypass Final Edit LiaYuri SadewoNo ratings yet
- Uptake and Distribution of Inhalational AnestheticsDocument12 pagesUptake and Distribution of Inhalational AnestheticsSuresh KumarNo ratings yet
- Νευρολογία σύνολο απαντήσεωνDocument38 pagesΝευρολογία σύνολο απαντήσεωνCheng Kuao HengNo ratings yet
- Hemodynamic Monitoring Pocket CardDocument5 pagesHemodynamic Monitoring Pocket CardFitz JaminitNo ratings yet
- Physics of Anaesthesia Made Easy: Review ArticleDocument7 pagesPhysics of Anaesthesia Made Easy: Review ArticleEinstein A. MustafaNo ratings yet
- Cardiac CycleDocument30 pagesCardiac CycleAdel100% (1)
- Appendix A: Doppler Ultrasound and Ankle-Brachial Pressure IndexDocument26 pagesAppendix A: Doppler Ultrasound and Ankle-Brachial Pressure IndexabigailNo ratings yet
- Cardiology Notes (Chris Andersen, ICUPrimaryPrep - Com) PDFDocument16 pagesCardiology Notes (Chris Andersen, ICUPrimaryPrep - Com) PDFPkernNo ratings yet
- Fibrous Skeleton of Heart PDFDocument2 pagesFibrous Skeleton of Heart PDFMeghan0% (1)
- Adult Bradycardia Algorithm: Identify and Treat Underlying CauseDocument1 pageAdult Bradycardia Algorithm: Identify and Treat Underlying CausenebrasNo ratings yet
- Cardiac Electrophysiology Basics (RL-204-Tn)Document5 pagesCardiac Electrophysiology Basics (RL-204-Tn)Navojit ChowdhuryNo ratings yet
- Anesthesia For Tracheoesophageal Fistula RepairDocument29 pagesAnesthesia For Tracheoesophageal Fistula RepairArop AkechNo ratings yet
- Mechanism of Action of Local AnaestheticsDocument19 pagesMechanism of Action of Local AnaestheticsSumit Bhardwaj100% (1)
- National ECG Workshop AIMST MMA 2015Document217 pagesNational ECG Workshop AIMST MMA 2015Sara100% (1)
- Sleep Apnoea - Prof - DR K.K.PDocument44 pagesSleep Apnoea - Prof - DR K.K.PjialeongNo ratings yet
- Blood Gas Analysis For Bedside DiagnosisDocument6 pagesBlood Gas Analysis For Bedside DiagnosisMuhamad Wirawan AdityoNo ratings yet
- Focal Atrial Tachycardia I: Clinical Features, DiagnosisDocument10 pagesFocal Atrial Tachycardia I: Clinical Features, Diagnosisapi-26166949No ratings yet
- MsmaidsDocument31 pagesMsmaidsnbrassarNo ratings yet
- 1) Vasoplegia During Cardiac Surgery Current Concepts and Management 2010Document5 pages1) Vasoplegia During Cardiac Surgery Current Concepts and Management 2010Carolina QuirogaNo ratings yet
- Renovascular Hypertension (RVH) SeminarDocument58 pagesRenovascular Hypertension (RVH) SeminarfaizalmasoodiNo ratings yet
- Diastolic Stress Echocardiography PDFDocument23 pagesDiastolic Stress Echocardiography PDFSofia KusumadewiNo ratings yet
- Antiarrhythmic Drugs - Classification and Mechanism of Action.Document1 pageAntiarrhythmic Drugs - Classification and Mechanism of Action.SUMIT KUMAR DASNo ratings yet
- Difficult Airway AlgorithmDocument48 pagesDifficult Airway AlgorithmshikhaNo ratings yet
- Ecmo and SepsisDocument37 pagesEcmo and SepsisMarckus BrodyNo ratings yet
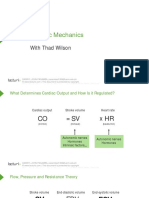
- Cardiac Mechanics: With Thad WilsonDocument26 pagesCardiac Mechanics: With Thad WilsonpasambalyrradjohndarNo ratings yet
- Protocol On Transcutaneous PacingDocument7 pagesProtocol On Transcutaneous PacingAnusha VergheseNo ratings yet
- HW InotropesDocument3 pagesHW InotropesNatalie YeohNo ratings yet
- Principles and Practice of Pharmacology for AnaesthetistsFrom EverandPrinciples and Practice of Pharmacology for AnaesthetistsRating: 5 out of 5 stars5/5 (1)
- 1.cardiac CycleDocument43 pages1.cardiac CycleNatasha Grace NtembwaNo ratings yet
- The Cardiac CycleDocument19 pagesThe Cardiac CycleRebi NesroNo ratings yet
- 293SPA Vismin Flyer 02232019Document1 page293SPA Vismin Flyer 02232019Bea ValerioNo ratings yet
- SK Conceptual FrameworkDocument1 pageSK Conceptual FrameworkBea ValerioNo ratings yet
- WASH Program: ProgramsDocument4 pagesWASH Program: ProgramsBea ValerioNo ratings yet
- TreatmentDocument1 pageTreatmentBea ValerioNo ratings yet
- Multifetal Gestation: Abesamis, Julius Bryan CDocument81 pagesMultifetal Gestation: Abesamis, Julius Bryan CBea ValerioNo ratings yet
- Block F Duty ScheduleDocument3 pagesBlock F Duty ScheduleBea ValerioNo ratings yet
- Course in The WardsDocument9 pagesCourse in The WardsBea ValerioNo ratings yet
- Venue: When: March 28 and 29 What Time: 7:30-9:00pm Where: "CAS SC BulletinDocument5 pagesVenue: When: March 28 and 29 What Time: 7:30-9:00pm Where: "CAS SC BulletinBea ValerioNo ratings yet
- Answers To ExercisesDocument19 pagesAnswers To ExercisesBea ValerioNo ratings yet
- PDH DeficiencyDocument5 pagesPDH DeficiencyBea ValerioNo ratings yet
- The Chieftest Mourner by Aida Rivera FordDocument4 pagesThe Chieftest Mourner by Aida Rivera FordBea Valerio0% (1)
- Simulator PDFDocument16 pagesSimulator PDFsssadangiNo ratings yet
- Analysis of PCGDocument7 pagesAnalysis of PCGMidhun DNo ratings yet
- Physio 2 - NotesDocument157 pagesPhysio 2 - NotesSivaranjini BhalaNo ratings yet
- Care of Adults 25 Cardiovascular ManagementDocument39 pagesCare of Adults 25 Cardiovascular ManagementGaras AnnaBerniceNo ratings yet
- Heart AssessmentDocument7 pagesHeart AssessmentKinn Noha100% (1)
- Cardio Vascular Assessment: Manali H Solanki F.Y.M.Sc - Nursing J G College of NursingDocument46 pagesCardio Vascular Assessment: Manali H Solanki F.Y.M.Sc - Nursing J G College of NursingmeghanaNo ratings yet
- Omd 551 - Part A & Part BDocument17 pagesOmd 551 - Part A & Part Baarthir88100% (2)
- Ashhad's Step 2 CK UW Notes PDFDocument166 pagesAshhad's Step 2 CK UW Notes PDFabNo ratings yet
- The Cardiovascular SystemDocument18 pagesThe Cardiovascular SystemVENUS LIRIA PANTINo ratings yet
- History and Physical ExaminationDocument18 pagesHistory and Physical ExaminationadesamboraNo ratings yet
- Chapter 5 Care of The Clients With Cardiovascular DisordersDocument226 pagesChapter 5 Care of The Clients With Cardiovascular DisordersDon Felicisimo EbronNo ratings yet
- Collecting Objective DataDocument61 pagesCollecting Objective DataAdrianAripNo ratings yet
- ASSESSMENT OF THORAX, LUNGS, Heart Neck Vessels, Breast, Lymphatic, Peripheral Vascular SystemDocument33 pagesASSESSMENT OF THORAX, LUNGS, Heart Neck Vessels, Breast, Lymphatic, Peripheral Vascular Systemandramercadejas730No ratings yet
- TEAMS - MCQsDocument34 pagesTEAMS - MCQsLyness Kay CheushiNo ratings yet
- Elective II FinalsDocument15 pagesElective II FinalsAljon Dofeliz LlamasNo ratings yet
- Chapter 20 Heart and Neck VesselsDocument10 pagesChapter 20 Heart and Neck Vesselsannoja selvaNo ratings yet
- Assessment of The Heart-Neck Vessels-Peripheral Vessels-PULSEDocument27 pagesAssessment of The Heart-Neck Vessels-Peripheral Vessels-PULSEJonah R. MeranoNo ratings yet
- Case Study FormatDocument15 pagesCase Study FormatLavie GangwarNo ratings yet
- Cardiovascular System: The Heart: Student Learning OutcomesDocument10 pagesCardiovascular System: The Heart: Student Learning Outcomeslily1liang-1No ratings yet
- (O. Nelson) Small Animal CardiologyDocument208 pages(O. Nelson) Small Animal CardiologyLoredana Gutu100% (1)
- Cardiac Anatomy and Phvsiologv A Review - Aorn800Document16 pagesCardiac Anatomy and Phvsiologv A Review - Aorn800Citra Ayu ApriliaNo ratings yet
- Physical Assessment of Cardiovascular SystemDocument31 pagesPhysical Assessment of Cardiovascular SystemaagNo ratings yet
- Cardiovascular AP & Nursing AssessmentDocument24 pagesCardiovascular AP & Nursing AssessmentIssy2703No ratings yet
- Valvular Heart DiseasesDocument29 pagesValvular Heart Diseasesbpt2No ratings yet
- HISTORY TAKING AND PE OF CARDIAC PATIENTS. Original.Document69 pagesHISTORY TAKING AND PE OF CARDIAC PATIENTS. Original.api-3858544No ratings yet
- De Veyra Assignment WK 3Document12 pagesDe Veyra Assignment WK 3adrian lozanoNo ratings yet
- Ebstein Anomaly in The Adult PatientDocument11 pagesEbstein Anomaly in The Adult PatientRJMNo ratings yet