Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5825)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- Westby Play Scale (2000)Document5 pagesWestby Play Scale (2000)ads89% (9)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Woodenclock Gears-Pl PDFDocument8 pagesWoodenclock Gears-Pl PDFstaticfactory928178% (9)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- 2 PlseDocument7 pages2 PlseadsNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Satyanarayana PoojaDocument33 pagesSatyanarayana Poojasrinivas3us100% (1)
- Functional Assessment Tool For Behavior PDFDocument2 pagesFunctional Assessment Tool For Behavior PDFads100% (1)
- ChartDocument6 pagesChartmiller_girlNo ratings yet
- Saheli V Commissioner of Police DelhiDocument5 pagesSaheli V Commissioner of Police DelhisuryakumarNo ratings yet
- Clause Type and Word Saliency in Second Language Incidental Vocabulary Acquisition Mary L. WattsDocument22 pagesClause Type and Word Saliency in Second Language Incidental Vocabulary Acquisition Mary L. WattsadsNo ratings yet
- BPDS-Victoria SY17-18 Adult ClassesDocument1 pageBPDS-Victoria SY17-18 Adult ClassesadsNo ratings yet
- AscoDocument1 pageAscoadsNo ratings yet
- Project Description and MethodologyDocument14 pagesProject Description and MethodologyWellfroNo ratings yet
- MsdsDocument10 pagesMsdsFarida NurahmanNo ratings yet
- Software Requirements Specification: Version 1.0 ApprovedDocument8 pagesSoftware Requirements Specification: Version 1.0 Approvedkirtika patelNo ratings yet
- Manufacturing Process Lab 01 DoneDocument4 pagesManufacturing Process Lab 01 DoneRk RanaNo ratings yet
- Fire Safety Management AND Fire Emergency PlanDocument25 pagesFire Safety Management AND Fire Emergency Plankenoly123100% (5)
- Australian/New Zealand StandardDocument9 pagesAustralian/New Zealand StandardhanryNo ratings yet
- Unit 4 - GeneticsDocument28 pagesUnit 4 - GeneticsRughaya SalsabilaNo ratings yet
- Ifr Com120c Maint ManualDocument29 pagesIfr Com120c Maint ManualErmanno LanzellottoNo ratings yet
- SOP Facility and Equipment HygieneDocument6 pagesSOP Facility and Equipment HygieneHenry Taguma100% (1)
- Apxvdgll26exd 43-C-I20 PreDocument4 pagesApxvdgll26exd 43-C-I20 Precmsd01No ratings yet
- Orifice Laboratory.Document9 pagesOrifice Laboratory.Abas S. AcmadNo ratings yet
- Technical Data Sheet: Granucult™ Plate Count Skimmed Milk Agar Acc. Iso 4833 and Iso 17410Document4 pagesTechnical Data Sheet: Granucult™ Plate Count Skimmed Milk Agar Acc. Iso 4833 and Iso 17410Sofia BedoyaNo ratings yet
- NC State PDFDocument27 pagesNC State PDFquantum16No ratings yet
- Sankya Theory Number Wise.Document23 pagesSankya Theory Number Wise.Suresh Lakshmi NarasimhanNo ratings yet
- Lect NotesDocument6 pagesLect Notessichangi2008_2776556No ratings yet
- Yarn Modification: Cotton MercerizationDocument49 pagesYarn Modification: Cotton Mercerizationsolomonsai1No ratings yet
- LBYBIO1 Circulatory System-Venous SystemDocument27 pagesLBYBIO1 Circulatory System-Venous SystemJBNo ratings yet
- Cleaning and Sanitizing in The Milk Processing Industry 2010Document28 pagesCleaning and Sanitizing in The Milk Processing Industry 2010John WaweruNo ratings yet
- Theplantaes S3 331Document13 pagesTheplantaes S3 331Jimena HernandezNo ratings yet
- Sample Chart of Accounts For A Large Corporation: Current AssetsDocument2 pagesSample Chart of Accounts For A Large Corporation: Current AssetsJay Dequilato TumaleNo ratings yet
- Chemistry Class Xi Chapter - 1Document8 pagesChemistry Class Xi Chapter - 1DoNga AstoRias TurNerNo ratings yet
- Medical Terminolgy Trans 1 115 SlidesDocument14 pagesMedical Terminolgy Trans 1 115 SlidesSophia Nicole LibaoNo ratings yet
- API 570 Final Exam Close Book Questions 23Document10 pagesAPI 570 Final Exam Close Book Questions 23Ravindra S. Jivani100% (1)
- Doka Formwork Manual 999776002 - 2015 - 04 - OnlineDocument48 pagesDoka Formwork Manual 999776002 - 2015 - 04 - OnlineEyo Etim50% (2)
- Approval Document ASSET DOC LOC 537Document4 pagesApproval Document ASSET DOC LOC 537aNo ratings yet
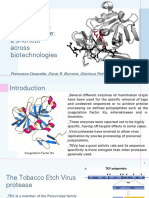
- Tobacco Etch Virus Protease: A Shortcut Across BiotechnologiesDocument16 pagesTobacco Etch Virus Protease: A Shortcut Across BiotechnologiesNhật ThiệnNo ratings yet
- PPTDocument17 pagesPPTTamil Videos100% (1)