Download as pdf or txt
You might also like
- MRCPExamResult 2 PDFDocument2 pagesMRCPExamResult 2 PDFumair100% (1)
- Ankle FracturesDocument47 pagesAnkle FracturesAbhishek UpadhyayNo ratings yet
- Lower Limb FracturesDocument124 pagesLower Limb FracturesMaríaJosé Dip100% (3)
- Comen Catalog 2021 - 4Document31 pagesComen Catalog 2021 - 4AroelNo ratings yet
- Femoral Shaft FractureDocument44 pagesFemoral Shaft FracturePrabuddha ThihawaNo ratings yet
- Complications and Outcomes of The Transfibular Approach For Posterolateral Fractures of The Tibial Plateau PDFDocument19 pagesComplications and Outcomes of The Transfibular Approach For Posterolateral Fractures of The Tibial Plateau PDFSergio Tomas Cortés MoralesNo ratings yet
- Case Report (Ola)Document44 pagesCase Report (Ola)amel015No ratings yet
- Trauma - Intertrochanteric Fracture - RustiniDocument7 pagesTrauma - Intertrochanteric Fracture - Rustinidedyalkarni08No ratings yet
- Extracapsular NOF #: Sarath Raveendran 2 0 0 7 M B B SDocument14 pagesExtracapsular NOF #: Sarath Raveendran 2 0 0 7 M B B SSarath RaveendranNo ratings yet
- La Consolacion College Manila: Femoral Neck FractureDocument3 pagesLa Consolacion College Manila: Femoral Neck FractureIvan Liquiran AvenadoNo ratings yet
- Closed Fracture of Midshaft Femur FracturesDocument33 pagesClosed Fracture of Midshaft Femur FracturesLana AdilaNo ratings yet
- Management of Avn HipDocument13 pagesManagement of Avn Hipterencedsza100% (1)
- Fracture of Neck of FemurDocument13 pagesFracture of Neck of FemurRosemarie AbelaNo ratings yet
- Fractures of Proximal FemurDocument38 pagesFractures of Proximal FemurMisoNo ratings yet
- AAOS2003 SpineDocument61 pagesAAOS2003 SpineHizkyas KassayeNo ratings yet
- Amputation RehabilitationDocument59 pagesAmputation RehabilitationAnushree DatarNo ratings yet
- 8.8.2017 - Fracture of FemurDocument57 pages8.8.2017 - Fracture of FemurUlfa Sari Al-Bahmi100% (1)
- BIKO OrthopaediDocument96 pagesBIKO OrthopaedikadekNo ratings yet
- FracturePPT UpdatedDocument108 pagesFracturePPT Updatedgaile pattugalanNo ratings yet
- Femur Shaft FracturesDocument26 pagesFemur Shaft FracturesOana Alexandra100% (3)
- Fracture FemurDocument28 pagesFracture FemurKulsoom ShahNo ratings yet
- Open Fracture Tibia Fibula FixDocument42 pagesOpen Fracture Tibia Fibula Fixannisaoktoviani100% (1)
- Fracture in Leg Tibia and FibulaDocument27 pagesFracture in Leg Tibia and Fibulachilsya shajiNo ratings yet
- Closed Fractures of The Tibial Diaphysis: David L. Rothberg, MD Erik N. Kubiak, MDDocument64 pagesClosed Fractures of The Tibial Diaphysis: David L. Rothberg, MD Erik N. Kubiak, MDtilahunthmNo ratings yet
- Avascular Necrosis and Related Complications Following Healed Osteoporotic Intertrochanteric FracturesDocument4 pagesAvascular Necrosis and Related Complications Following Healed Osteoporotic Intertrochanteric FracturesNasrull BinHzNo ratings yet
- BackgroundDocument5 pagesBackgroundMaricar K. BrionesNo ratings yet
- Surgical Treatment of Neglected Malunion of Shaft Femur: Case ReportDocument13 pagesSurgical Treatment of Neglected Malunion of Shaft Femur: Case ReportNando OktariNo ratings yet
- Fracture It FemurDocument50 pagesFracture It FemurSonal RaikwarNo ratings yet
- ResStudy StatementsDocument380 pagesResStudy StatementscooperorthopaedicsNo ratings yet
- Ortho Fraktur 1/3 Proximal Humerus DextraDocument57 pagesOrtho Fraktur 1/3 Proximal Humerus DextraFian ChristoNo ratings yet
- Distal Radius FracturesDocument68 pagesDistal Radius Fracturescalvin_c_wangNo ratings yet
- Femur Shaft FractureDocument33 pagesFemur Shaft FractureAkash KoulNo ratings yet
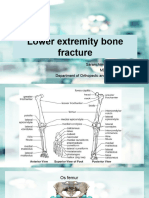
- Lower Extremity Bone Fracture Lecture 3Document88 pagesLower Extremity Bone Fracture Lecture 3Tselmeg TselmegNo ratings yet
- Case Study of "Subtrochanteric Femur": Prepared By: John Ress A. Escobal Group 1Document11 pagesCase Study of "Subtrochanteric Femur": Prepared By: John Ress A. Escobal Group 1J.r. MercadoNo ratings yet
- Fractures of Forearm: Oktya Veny Simbolon Pattiyah Prehandini AyuningtyasDocument90 pagesFractures of Forearm: Oktya Veny Simbolon Pattiyah Prehandini AyuningtyaspattiyahNo ratings yet
- Frienchzel Joy A. Asis Group 3 BSN 3-ADocument14 pagesFrienchzel Joy A. Asis Group 3 BSN 3-AKenneth Louis GalizaNo ratings yet
- FSP ORP Handout English Intertrochanteric Femoral Fractures FinalDocument10 pagesFSP ORP Handout English Intertrochanteric Femoral Fractures FinalPratiwi Indah SayektiNo ratings yet
- Facial InjuriesDocument61 pagesFacial InjuriesafifrspmNo ratings yet
- Manejo de Fracturas Mediales de Cadera 2015 Femoral Neck Fractures - Current ManagementDocument9 pagesManejo de Fracturas Mediales de Cadera 2015 Femoral Neck Fractures - Current ManagementSergio Tomas Cortés MoralesNo ratings yet
- Fracture of Shaft Tibia FibulaDocument26 pagesFracture of Shaft Tibia Fibulagalih widodoNo ratings yet
- Case Report Juli 2013Document21 pagesCase Report Juli 2013NahdiaNo ratings yet
- Femoral Neck FractureDocument28 pagesFemoral Neck FractureayuegpNo ratings yet
- Closed Fracture of Right Tibial Plateau Schatzker VI: Case ReportDocument45 pagesClosed Fracture of Right Tibial Plateau Schatzker VI: Case ReportRido RdNo ratings yet
- Case Study - Intertrochanteric Hip FractureDocument13 pagesCase Study - Intertrochanteric Hip FractureLei Ortega100% (6)
- Intra-Capsular Neck of Femur Fractures: Sheweidin AZIZ - Sep 2015Document39 pagesIntra-Capsular Neck of Femur Fractures: Sheweidin AZIZ - Sep 2015ShaastieNo ratings yet
- 35 Daksh EtalDocument4 pages35 Daksh EtaleditorijmrhsNo ratings yet
- Case ReportDocument32 pagesCase Reportsul11No ratings yet
- Lect 8 - Internal Fixation - IIDocument21 pagesLect 8 - Internal Fixation - IIAnkit LakshyaNo ratings yet
- Distal Humeros PedDocument55 pagesDistal Humeros PedSuad StambulieNo ratings yet
- Oite 2006Document823 pagesOite 2006dastroh100% (1)
- Case Report Supracondylar Fracture of Right FemurDocument37 pagesCase Report Supracondylar Fracture of Right FemurSri Mahtufa Riski100% (1)
- Femoral Neck FracturesDocument10 pagesFemoral Neck FracturesMorshed Mahbub AbirNo ratings yet
- Fractures in Brief Intertrochanteric Hip FracturesDocument3 pagesFractures in Brief Intertrochanteric Hip FracturesikhwanNo ratings yet
- Open Reduction Internal FixationDocument7 pagesOpen Reduction Internal FixationalcojonicNo ratings yet
- U04 Fxs of Humeral ShaftDocument88 pagesU04 Fxs of Humeral Shaftadrian_mogosNo ratings yet
- P and o SelfDocument443 pagesP and o SelfDeepa SeiraNo ratings yet
- Intertrochanteric Femur Fracture - StatPearls - NCBI BookshelfDocument9 pagesIntertrochanteric Femur Fracture - StatPearls - NCBI Bookshelfmingchuan chuNo ratings yet
- 32 Yadkikar EtalDocument6 pages32 Yadkikar EtaleditorijmrhsNo ratings yet
- Proximal Hamstring Tears: From Endoscopic Repair to Open ReconstructionFrom EverandProximal Hamstring Tears: From Endoscopic Repair to Open ReconstructionThomas YoumNo ratings yet
- Acetabular Fractures in Older Patients: Assessment and ManagementFrom EverandAcetabular Fractures in Older Patients: Assessment and ManagementTheodore T. MansonNo ratings yet
- Refusal FormDocument1 pageRefusal FormViral Chann3LNo ratings yet
- Presbyterian Hospital Nursing School Durtlang, Aizawl: MizoramDocument9 pagesPresbyterian Hospital Nursing School Durtlang, Aizawl: Mizoramlaltea2677No ratings yet
- Stages of LaborDocument5 pagesStages of LaborRosemae Literatos100% (1)
- Daftar PustakaDocument2 pagesDaftar PustakatiarNo ratings yet
- Fractured Neck of FemurDocument20 pagesFractured Neck of Femurrajvikram87No ratings yet
- Anatomy of Fascial SpacesDocument40 pagesAnatomy of Fascial SpacesAKSHAYA SUBHASHINEE DNo ratings yet
- Artifacts in CytopathologyDocument25 pagesArtifacts in Cytopathologysamuel adagaNo ratings yet
- Classification of Health Care OrganizationsDocument34 pagesClassification of Health Care OrganizationsKoushali BanerjeeNo ratings yet
- Gynecological ExaminationDocument20 pagesGynecological Examinationwahyu kijang ramadhanNo ratings yet
- Advances en Pediatrics 2013Document395 pagesAdvances en Pediatrics 2013Gris C. RicoNo ratings yet
- Voluntary Surgical Contraception For Women Tubal Occlusion: Dr. Duddy S. Nataprawira, Spog (K)Document60 pagesVoluntary Surgical Contraception For Women Tubal Occlusion: Dr. Duddy S. Nataprawira, Spog (K)Pebri HantoNo ratings yet
- Patient Handover, Patient EndorsementDocument12 pagesPatient Handover, Patient Endorsementgladz25100% (2)
- DTLLDocument8 pagesDTLLSuchitKNo ratings yet
- Policy Action Plan 1Document7 pagesPolicy Action Plan 1api-548969267No ratings yet
- Dystocia Due To Bull Dog Foetal Monster Calf in A Buffaloe PDFDocument1 pageDystocia Due To Bull Dog Foetal Monster Calf in A Buffaloe PDFRavi RaidurgNo ratings yet
- EpisiotomyDocument6 pagesEpisiotomyNishaThakuri100% (1)
- Post Partum HaemorrhageDocument21 pagesPost Partum HaemorrhageKanika VermaNo ratings yet
- American Society For Reproductive MedicineDocument3 pagesAmerican Society For Reproductive MedicineShanti Natalia NababanNo ratings yet
- Anatomy - B. Rabischong - GRDocument20 pagesAnatomy - B. Rabischong - GRAnonymous UHnQSkxLBDNo ratings yet
- Khaled Said, M.D.: 12/2008 To Present Hamad Medical Corporation, QatarDocument4 pagesKhaled Said, M.D.: 12/2008 To Present Hamad Medical Corporation, QatarKhaled F. SaidNo ratings yet
- Workload Indicators (Staffing Norms)Document131 pagesWorkload Indicators (Staffing Norms)asimsiNo ratings yet
- Basal Cell Carcinoma: CausesDocument5 pagesBasal Cell Carcinoma: CausesRini LianingsihNo ratings yet
- CURS 5 Abnormalities of The Umbilical Cord and Amniotic FluidDocument33 pagesCURS 5 Abnormalities of The Umbilical Cord and Amniotic FluidFayad AlmohamedNo ratings yet
- BC PDFDocument2 pagesBC PDFRitesh SharmaNo ratings yet
- Positioning in NursingDocument6 pagesPositioning in NursingArsheen BalouchNo ratings yet
- Resume - Laura Robbins RN BSN 2023 Dec 2023Document1 pageResume - Laura Robbins RN BSN 2023 Dec 2023api-605816436No ratings yet
- ObGyn Board Review PDFDocument85 pagesObGyn Board Review PDFCoolrobertizNo ratings yet
- Prenatal CareDocument67 pagesPrenatal CareAllurie Umel100% (3)