Download as docx, pdf, or txt
You might also like
- Hidden Epidemic: Silent Oral Infections Cause Most Heart Attacks and Breast CancersFrom EverandHidden Epidemic: Silent Oral Infections Cause Most Heart Attacks and Breast CancersRating: 5 out of 5 stars5/5 (1)
- ARC132 U Toronto SyllabusDocument6 pagesARC132 U Toronto SyllabusEcon StudentNo ratings yet
- Dietary Manipulation To Reduce Nitrogen and Phosphorus Excretion by Dairy CowsDocument6 pagesDietary Manipulation To Reduce Nitrogen and Phosphorus Excretion by Dairy CowsLluís Morey100% (1)
- CURRENT Diagnosis & Treatment in Otolaryngology-Head & Neck Surgery, 3eDocument3 pagesCURRENT Diagnosis & Treatment in Otolaryngology-Head & Neck Surgery, 3eStephanie Vania EmbangNo ratings yet
- COVID - 19 and Sudden Sensorineural Hearing Loss ADocument8 pagesCOVID - 19 and Sudden Sensorineural Hearing Loss Abay aji15No ratings yet
- Bjorl: Hearing Loss in People With HIV/AIDS and Associated Factors: An Integrative ReviewDocument8 pagesBjorl: Hearing Loss in People With HIV/AIDS and Associated Factors: An Integrative ReviewFelipe Hernández SepúlvedaNo ratings yet
- Presbycusis JournalDocument11 pagesPresbycusis JournalJairah CandaoNo ratings yet
- Hearing LossDocument12 pagesHearing LossFirdha Aulia NisaNo ratings yet
- Kwame Nkrumah University of Science and Technology: College of Health Sciences School of Medical SciencesDocument25 pagesKwame Nkrumah University of Science and Technology: College of Health Sciences School of Medical SciencesEmmanuel DanquahNo ratings yet
- Pérdida Auditiva y Uso de Los Servicios de Salud Un Estudio Transversal de Base Poblacional Entre Adultos Mayores FinlandesesDocument11 pagesPérdida Auditiva y Uso de Los Servicios de Salud Un Estudio Transversal de Base Poblacional Entre Adultos Mayores FinlandesesMARTIN NICOLAS MORA STAGNONo ratings yet
- Guided Worksheet 1Document7 pagesGuided Worksheet 1EveNo ratings yet
- DD Hearing LossDocument13 pagesDD Hearing LossDavid-ortho Novi-rehabNo ratings yet
- ConditionsDocument2 pagesConditionsTon SawyerNo ratings yet
- AAF en AdultosDocument8 pagesAAF en AdultosJennifer ArévaloNo ratings yet
- Hearing Hta ReportDocument54 pagesHearing Hta ReportPaul RaduNo ratings yet
- Brainsci 10 00732Document11 pagesBrainsci 10 00732Nur Rahmi SeptiantyNo ratings yet
- Ijsrp p1486Document6 pagesIjsrp p1486Sandeep KumarNo ratings yet
- High-Frequency Audiometry For Early Detection of Hearing Loss: A Narrative ReviewDocument13 pagesHigh-Frequency Audiometry For Early Detection of Hearing Loss: A Narrative ReviewJennifer ArévaloNo ratings yet
- Assessment 104 Assignment 1 1Document7 pagesAssessment 104 Assignment 1 1api-314849412No ratings yet
- Tinnitus 2019Document20 pagesTinnitus 2019Leslie Lindsay AlvarezNo ratings yet
- Cochlear and Vestibular Functional Study in Patients With Sudden Deafness and Lyme DiseaseDocument5 pagesCochlear and Vestibular Functional Study in Patients With Sudden Deafness and Lyme DiseaseAura RachmawatiNo ratings yet
- Jurnal THTDocument6 pagesJurnal THTFeby Arin BindaNo ratings yet
- Management of Sudden Sensorineural Hearing Loss Among Primary Care Physicians in Canada: A Survey StudyDocument11 pagesManagement of Sudden Sensorineural Hearing Loss Among Primary Care Physicians in Canada: A Survey StudyBTS LGONo ratings yet
- Study of The Effect of Mobile Phones On HearingDocument5 pagesStudy of The Effect of Mobile Phones On HearingPranay DasNo ratings yet
- Amplification: The Treatment of Choice For Presbycusis: Eye & Ear DiseasesDocument3 pagesAmplification: The Treatment of Choice For Presbycusis: Eye & Ear DiseasesNi Wayan Ana PsNo ratings yet
- Services On Demand Article: Revista Brasileira de OtorrinolaringologiaDocument11 pagesServices On Demand Article: Revista Brasileira de OtorrinolaringologiaMauricio RodriguezNo ratings yet
- s13063 020 04579 6Document11 pagess13063 020 04579 6BTS LGONo ratings yet
- Copia de Otolaryngology Clinic of North America Evidence-Based Practice Management of Hoarseness-DysphoniaDocument18 pagesCopia de Otolaryngology Clinic of North America Evidence-Based Practice Management of Hoarseness-DysphoniaEdna R. Alvarez PaezNo ratings yet
- Screenshot 2021-03-03 at 8.03.31 PMDocument12 pagesScreenshot 2021-03-03 at 8.03.31 PMIhsan HanifNo ratings yet
- Managing Otitis Media With Effusion in Young Children: Practice GuidelineDocument11 pagesManaging Otitis Media With Effusion in Young Children: Practice GuidelineJohn ThunderNo ratings yet
- Indications For Cochlear ImplantsDocument12 pagesIndications For Cochlear Implantscristina georgianaNo ratings yet
- prevalenciaDocument4 pagesprevalenciaLaura Sofía Miranda RellánNo ratings yet
- Current Concepts: Review ArticleDocument7 pagesCurrent Concepts: Review ArticleMia Mia MiaNo ratings yet
- Sensor I NeuralDocument3 pagesSensor I NeuralReza AkbarNo ratings yet
- Hearing Loss AssessmentDocument31 pagesHearing Loss AssessmentKIBET ERNEST MUTAINo ratings yet
- Hearingloss: The Silent Risk For Psychiatric Disorders in Late LifeDocument9 pagesHearingloss: The Silent Risk For Psychiatric Disorders in Late LifeDhino Armand Quispe SánchezNo ratings yet
- Kung 2007Document10 pagesKung 2007Sarah fadlainiNo ratings yet
- G1a115016 - Tesa SeptiariDocument12 pagesG1a115016 - Tesa SeptiariTesa SeptiariNo ratings yet
- Obstructive Sleep ApneaDocument21 pagesObstructive Sleep ApneaIJAR JOURNALNo ratings yet
- Lecture NPPCD DeafnessDocument35 pagesLecture NPPCD DeafnessAkshay50% (2)
- A Holistic ApproachDocument13 pagesA Holistic ApproachsepthyaniNo ratings yet
- Geriatric Otolaryngology Author Hinrich StaeckerDocument22 pagesGeriatric Otolaryngology Author Hinrich StaeckerSHERIF ZAHERNo ratings yet
- Action Plan For Full Service Department of AudiologyDocument9 pagesAction Plan For Full Service Department of AudiologyANTHONY MURASKINo ratings yet
- DTSCH Arztebl Int-117 0690Document12 pagesDTSCH Arztebl Int-117 0690CoAsst MuhammadNuhAlhudawyNo ratings yet
- Otolaryngol - Head Neck Surg - 2020 - Basura - Clinical Practice Guideline M Ni Re S DiseaseDocument56 pagesOtolaryngol - Head Neck Surg - 2020 - Basura - Clinical Practice Guideline M Ni Re S DiseaseTruong Ngoc HuyNo ratings yet
- Reading 77Document17 pagesReading 77Kavalam GeorgeNo ratings yet
- Final Nguyen Petrik HivaidsDocument7 pagesFinal Nguyen Petrik Hivaidsapi-754056237No ratings yet
- Ear ChronicDocument44 pagesEar ChronicȜLaa AsHrafNo ratings yet
- World Hearing DayDocument27 pagesWorld Hearing DayPomy AgrawalNo ratings yet
- Infra Sound Brief Review of Toxicological LiteratureDocument51 pagesInfra Sound Brief Review of Toxicological Literaturesgcauri2157No ratings yet
- Ahl N DepressionDocument7 pagesAhl N DepressionDr Pavina RayamajhiNo ratings yet
- Noise 4Document34 pagesNoise 4NIKOLAOS CHATZAKISNo ratings yet
- Noise-Induced Hearing LossDocument34 pagesNoise-Induced Hearing LossKiswah YohanaNo ratings yet
- 2021 Auriculo e ZumbidoDocument12 pages2021 Auriculo e ZumbidoNáthaly de MoraesNo ratings yet
- Dapus 9 Referat 1Document6 pagesDapus 9 Referat 1Akramanto RidwanNo ratings yet
- Script Thesis ProposalDocument4 pagesScript Thesis Proposalpearl justado0% (2)
- Vestibular Neutitis & Labyrinthitis PDFDocument6 pagesVestibular Neutitis & Labyrinthitis PDFFika Khulma SofiaNo ratings yet
- 5912 PDFDocument10 pages5912 PDFemilia candraNo ratings yet
- Wa0007Document17 pagesWa0007Eko WidodoNo ratings yet
- Health Asme 7Document4 pagesHealth Asme 7Harmin HawkinsNo ratings yet
- 2010 Grossi Pycnogenol Improves Tinnitus SymptomsDocument5 pages2010 Grossi Pycnogenol Improves Tinnitus Symptomsjulian_rosengrenNo ratings yet
- Biography of John Mordecai Gottman 1Document4 pagesBiography of John Mordecai Gottman 1kalitkalitNo ratings yet
- Railway Accounting: Indian Railway Accounts ServiceDocument5 pagesRailway Accounting: Indian Railway Accounts ServiceAbhijeet AsthanaNo ratings yet
- GHB FactsheetDocument2 pagesGHB FactsheetABC Action NewsNo ratings yet
- Prosecutor v. FurundzijaDocument1 pageProsecutor v. Furundzijacrlstinaaa100% (1)
- Checklist For T&C of Chemical Fire Suppression SystemDocument2 pagesChecklist For T&C of Chemical Fire Suppression Systembeho2000No ratings yet
- Bombas SumergiblesDocument79 pagesBombas SumergiblesInstinct_brNo ratings yet
- Father's of Various FieldsDocument5 pagesFather's of Various FieldsAsad AliNo ratings yet
- Journal of Colloid and Interface Science: Michael P. Brandon, Deirdre M. Ledwith, John M. KellyDocument8 pagesJournal of Colloid and Interface Science: Michael P. Brandon, Deirdre M. Ledwith, John M. KellyCharles TayNo ratings yet
- NYJC Prelim 2006 P2Document12 pagesNYJC Prelim 2006 P2miiewNo ratings yet
- Thrive The Vegan Nutrition Guide Brendan Brazier.15709 - 1contents - and - IntroductionDocument8 pagesThrive The Vegan Nutrition Guide Brendan Brazier.15709 - 1contents - and - IntroductionCristhian ChávezNo ratings yet
- Process, People, and Conflict Management in OrganizationsDocument6 pagesProcess, People, and Conflict Management in OrganizationsMeldy IamNo ratings yet
- Vaxigrip Tetra Pi Nh19-20Document2 pagesVaxigrip Tetra Pi Nh19-20A. shahizaNo ratings yet
- Reportable in The Supreme Court of India Criminal Appellate Jurisdiction Criminal Appeal NO. 615 of 2020 (Arising Out of SLP (CRL.) No.8260/2018)Document38 pagesReportable in The Supreme Court of India Criminal Appellate Jurisdiction Criminal Appeal NO. 615 of 2020 (Arising Out of SLP (CRL.) No.8260/2018)GunjeetNo ratings yet
- Unit 5. PHCDocument24 pagesUnit 5. PHCFenembar MekonnenNo ratings yet
- 2022 WCRC Rules and Regulations - 2021-12-06Document32 pages2022 WCRC Rules and Regulations - 2021-12-06Adhi MuhyidinNo ratings yet
- Vidura Niti Snaskrit Text With English TranslationDocument217 pagesVidura Niti Snaskrit Text With English TranslationBivak BhattacharjeeNo ratings yet
- 11th Zoology Volume 1 New School Books Download English MediumDocument240 pages11th Zoology Volume 1 New School Books Download English Mediumaishikanta beheraNo ratings yet
- Heridity: Table of SpecificationsDocument8 pagesHeridity: Table of SpecificationsJoseph GratilNo ratings yet
- Pamphlet 21 (NCl3)Document210 pagesPamphlet 21 (NCl3)victorNo ratings yet
- Vashikaran Mantra For Love PDFDocument4 pagesVashikaran Mantra For Love PDFmustafaaldin0% (2)
- 1.2 Safety & Rules in Biology LaboratoryDocument32 pages1.2 Safety & Rules in Biology LaboratoryasyuraNo ratings yet
- Food and FarmingDocument38 pagesFood and FarmingKevin LlorenteNo ratings yet
- Department of Education: Republic of The PhilippinesDocument14 pagesDepartment of Education: Republic of The PhilippinesJanna GunioNo ratings yet
- Reference HelicoilDocument1 pageReference HelicoilPetrotrim ServicesNo ratings yet
- Radiation HazardDocument27 pagesRadiation Hazardlelu ojhaNo ratings yet
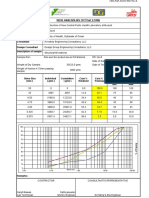
- CED-PQP-5225-F01 Rev.0 Sieve AnalysisDocument4 pagesCED-PQP-5225-F01 Rev.0 Sieve AnalysisSslan seelanNo ratings yet
- 8 - Human Reproduction - G12 - G12 - DR Ross-1Document55 pages8 - Human Reproduction - G12 - G12 - DR Ross-1sibusisiwekhanyile.333No ratings yet
- Msds Heksana - 2 PDFDocument6 pagesMsds Heksana - 2 PDFGelisaNo ratings yet