Download as doc, pdf, or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5822)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Normal Flora of HumanDocument54 pagesNormal Flora of Humankumari astha rupaliNo ratings yet
- Pediatrics 1951 Glicklich 859 76Document20 pagesPediatrics 1951 Glicklich 859 76Gaetano Di GiovanniNo ratings yet
- Jurnal SkripsiDocument29 pagesJurnal SkripsiVivin Novitasari Ptr ZNNo ratings yet
- Chemicals EvaluatedDocument41 pagesChemicals EvaluatedSophia LeãoNo ratings yet
- Ibbi I. Emmanuel - Curriculum VitaeDocument12 pagesIbbi I. Emmanuel - Curriculum VitaeWakaye AbbaNo ratings yet
- Week 8 - Chapter 10 PDFDocument35 pagesWeek 8 - Chapter 10 PDFnajlaNo ratings yet
- PHYSIOLOGY Chapter 1Document4 pagesPHYSIOLOGY Chapter 1HUBERT JOHN RAMOSNo ratings yet
- HI Life ProductsDocument10 pagesHI Life ProductsAbhinav GargNo ratings yet
- INOUE-BALLOON Catheter - TORAYDocument3 pagesINOUE-BALLOON Catheter - TORAYwahyuNo ratings yet
- Assessing A Brachial Artery Blood PressureDocument21 pagesAssessing A Brachial Artery Blood PressureEric ParmleyNo ratings yet
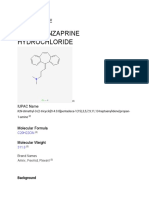
- Cyclobenzaprine Hydrochloride: Drug ProfileDocument13 pagesCyclobenzaprine Hydrochloride: Drug ProfileShruti ThakurNo ratings yet
- Unit III Plant Disease and SymptomsDocument23 pagesUnit III Plant Disease and SymptomsKhenan James NarismaNo ratings yet
- Presentation On: Pueperal Sepsis: Submitted To: Sandhya Maam Submitted By: Dhana BC Kismita Rai BSC 3 YearDocument31 pagesPresentation On: Pueperal Sepsis: Submitted To: Sandhya Maam Submitted By: Dhana BC Kismita Rai BSC 3 YearRumi Maharjan100% (1)
- Current Diagnosis and Treatment Pediatrics 23Rd Edition William W Hay JR Full ChapterDocument67 pagesCurrent Diagnosis and Treatment Pediatrics 23Rd Edition William W Hay JR Full Chapterkaty.manley552100% (6)
- 123 Cocos NuciferaDocument15 pages123 Cocos NuciferaOrockjoNo ratings yet
- Comments Nbde ExamsDocument9 pagesComments Nbde ExamsMark GebrailNo ratings yet
- Concept PaperDocument3 pagesConcept PaperNndaydna0% (1)
- Title 42 Letter To Dr. Walensky From MGB & HMS ColleaguesDocument14 pagesTitle 42 Letter To Dr. Walensky From MGB & HMS Colleaguesdialynn dwyerNo ratings yet
- Daftar PustakaDocument3 pagesDaftar PustakaSatria Rao RezaNo ratings yet
- Amikinhal TrialDocument11 pagesAmikinhal TrialBreno Bertozo SilvaNo ratings yet
- Case Study 31 Adime NoteDocument3 pagesCase Study 31 Adime Noteapi-533641139No ratings yet
- PDF High Acuity Nursing 7Th Edition Kathleen Wagner Ebook Full ChapterDocument53 pagesPDF High Acuity Nursing 7Th Edition Kathleen Wagner Ebook Full Chapterwilliam.krasner11867% (3)
- Maria Victoria Hofileña, M.D.: AnesthesiologyDocument6 pagesMaria Victoria Hofileña, M.D.: AnesthesiologyAbegail IbañezNo ratings yet
- ATLS, AHA, Rosen & Barkin's 5-Minute Emergency Medicine Consult, 3rd EditionDocument35 pagesATLS, AHA, Rosen & Barkin's 5-Minute Emergency Medicine Consult, 3rd EditionRai LaksmiNo ratings yet
- Muse 123, Fall 2014 Breathing For Singing (James Mckinney, Kimberly James, Costanza Cuccaro)Document2 pagesMuse 123, Fall 2014 Breathing For Singing (James Mckinney, Kimberly James, Costanza Cuccaro)MerrillLeeRasmussenNo ratings yet
- Master ActivatorDocument30 pagesMaster ActivatorcuriosityunshackledfranceNo ratings yet
- DRG Overview of All Patient Refined Diagostic Related GroupsDocument42 pagesDRG Overview of All Patient Refined Diagostic Related Groupsjaypee pengNo ratings yet
- Ijpm Sep 20 PDFDocument104 pagesIjpm Sep 20 PDFsriniNo ratings yet
- IRON5Document11 pagesIRON5scgtm6gc46No ratings yet
- Maternal and Child Health Nursing TransesDocument17 pagesMaternal and Child Health Nursing Transesmainek42No ratings yet