Download as pdf or txt
You might also like
- Calcifying Epithelial Odontogenic Tumor - A CaseDocument5 pagesCalcifying Epithelial Odontogenic Tumor - A CaseKharismaNisaNo ratings yet
- Ameloblastic Fibroma: Report of A Case: Su-Gwan Kim, DDS, PHD, and Hyun-Seon Jang, DDS, PHDDocument3 pagesAmeloblastic Fibroma: Report of A Case: Su-Gwan Kim, DDS, PHD, and Hyun-Seon Jang, DDS, PHDdoktergigikoeNo ratings yet
- Follicular With Plexiform Ameloblastoma in Anterior Mandible: Report of Case and Literature ReviewDocument6 pagesFollicular With Plexiform Ameloblastoma in Anterior Mandible: Report of Case and Literature Reviewluckytung07No ratings yet
- Saudi Journal of Pathology and Microbiology (SJPM) : Case ReportDocument3 pagesSaudi Journal of Pathology and Microbiology (SJPM) : Case ReportSuman ChaturvediNo ratings yet
- Bilateral Adenomatoid Odontogenic Tumour of The Maxilla in A 2-Year-Old Female-The Report of A Rare Case and Review of The LiteratureDocument7 pagesBilateral Adenomatoid Odontogenic Tumour of The Maxilla in A 2-Year-Old Female-The Report of A Rare Case and Review of The LiteratureStephanie LyonsNo ratings yet
- Case Report Ameloblastic Fibroma: Report of 3 Cases and Literature ReviewDocument5 pagesCase Report Ameloblastic Fibroma: Report of 3 Cases and Literature ReviewcareNo ratings yet
- Adenomatoid Odontogenic Tumor, An Uncommon TumorDocument3 pagesAdenomatoid Odontogenic Tumor, An Uncommon TumorHarshavardhan ReddyNo ratings yet
- Tumor Odontogenico EscamosoDocument4 pagesTumor Odontogenico Escamosoメカ バルカNo ratings yet
- Mandibular Ameloblastoma in A 10-Year-Old Child: Case Report and Review of The LiteratureDocument6 pagesMandibular Ameloblastoma in A 10-Year-Old Child: Case Report and Review of The LiteratureWidhi Satrio NugrohoNo ratings yet
- Peripheral Cemento-Ossifying Fibroma - A Case Report With A Glimpse On The Differential DiagnosisDocument5 pagesPeripheral Cemento-Ossifying Fibroma - A Case Report With A Glimpse On The Differential DiagnosisnjmdrNo ratings yet
- Unicystic Ameloblastoma - Investigation Into An Enigma: IOSR Journal of Dental and Medical Sciences February 2020Document5 pagesUnicystic Ameloblastoma - Investigation Into An Enigma: IOSR Journal of Dental and Medical Sciences February 2020dr.filipcristian87No ratings yet
- Lucrare Stiintifica ParodontologieDocument4 pagesLucrare Stiintifica ParodontologieReduceriAvonNo ratings yet
- Ameloblastoma Report CaseDocument6 pagesAmeloblastoma Report CaseYuzketNo ratings yet
- Gingival Squamous Cell Carcinoma: A Case Report: Dr. P.S.Rakhewar, Dr. Vrunda Kanjalkar, DR - Ruby SyedDocument3 pagesGingival Squamous Cell Carcinoma: A Case Report: Dr. P.S.Rakhewar, Dr. Vrunda Kanjalkar, DR - Ruby SyedGrecia SunurNo ratings yet
- JPNR - S04 - 233Document6 pagesJPNR - S04 - 233Ferisa paraswatiNo ratings yet
- PMR 2 1 6Document4 pagesPMR 2 1 6Adrian PermadiNo ratings yet
- AmeloblastomaDocument6 pagesAmeloblastomaNASTYHAIR 24No ratings yet
- Management of Unicystic Ameloblastoma Crossing Midline in Mandible in Geriatric Patient - July - 2020 - 9370586511 - 3513376Document3 pagesManagement of Unicystic Ameloblastoma Crossing Midline in Mandible in Geriatric Patient - July - 2020 - 9370586511 - 3513376Sowmya ManthaNo ratings yet
- Gingival Epulis: Report of Two Cases.: Dr. Praful Choudhari, Dr. Praneeta KambleDocument5 pagesGingival Epulis: Report of Two Cases.: Dr. Praful Choudhari, Dr. Praneeta KambleAnandNo ratings yet
- Ameloblastic Fibro-Dentinoma of Mandible: A Case ReportDocument3 pagesAmeloblastic Fibro-Dentinoma of Mandible: A Case ReportBrutusRexNo ratings yet
- Adenomatoid Odontogenic Tumour of Maxilla A Case ReportDocument6 pagesAdenomatoid Odontogenic Tumour of Maxilla A Case ReportAthenaeum Scientific PublishersNo ratings yet
- CarcinomaDocument5 pagesCarcinomaLori SimmonsNo ratings yet
- 2019 Article 867Document8 pages2019 Article 867Reyes Ivan García CuevasNo ratings yet
- Chondrosarcome MandiDocument8 pagesChondrosarcome MandiKarim OuniNo ratings yet
- Ameloblastoma Arising in The Wall of Dentigerous Cyst - A Case ReportDocument3 pagesAmeloblastoma Arising in The Wall of Dentigerous Cyst - A Case ReportSenussi IbtisamNo ratings yet
- Adenoid Cystic Carcinoma of Hard Palate: A Case ReportDocument5 pagesAdenoid Cystic Carcinoma of Hard Palate: A Case ReportHemant GuptaNo ratings yet
- Eruption CystDocument4 pagesEruption CystHeri Papangah FarhanNo ratings yet
- Odontogenic Cysts and Odontogenic Tumors in A Large Rural Area From India. A 10-Year ReflectionDocument5 pagesOdontogenic Cysts and Odontogenic Tumors in A Large Rural Area From India. A 10-Year ReflectionAlan VargasNo ratings yet
- Case Report The Challenging Diagnosis of Primordial Odontogenic TumorDocument5 pagesCase Report The Challenging Diagnosis of Primordial Odontogenic Tumorlee zaraNo ratings yet
- Maxillary Unicystic Ameloblastoma: A Review of The LiteratureDocument0 pagesMaxillary Unicystic Ameloblastoma: A Review of The LiteratureXatly OviedoNo ratings yet
- Maxillary Unicystic Ameloblastoma: A Case: BMC Research NotesDocument6 pagesMaxillary Unicystic Ameloblastoma: A Case: BMC Research NotesIftinan LQNo ratings yet
- 10º-Adenoid Cystic Carcinoma of Alveolar Mucosa A Rare CaseDocument3 pages10º-Adenoid Cystic Carcinoma of Alveolar Mucosa A Rare Casecihece7650No ratings yet
- JDS 17 370Document15 pagesJDS 17 370Ferry HendrawanNo ratings yet
- Osseous Choristoma of The Periodontium: Case ReportDocument3 pagesOsseous Choristoma of The Periodontium: Case ReportAndykaYayanSetiawanNo ratings yet
- 2 51 1647598330 5ijmpsjun202205Document10 pages2 51 1647598330 5ijmpsjun202205TJPRC PublicationsNo ratings yet
- Ameloblastoma: Notorious Tumor of The Jaw - Report of A CaseDocument3 pagesAmeloblastoma: Notorious Tumor of The Jaw - Report of A CaseUwie MoumootNo ratings yet
- Ameloblastoma: A Clinicoradiographic and Histopathologic Correlation of 11 Cases Seen in Goa During 2008-2012Document6 pagesAmeloblastoma: A Clinicoradiographic and Histopathologic Correlation of 11 Cases Seen in Goa During 2008-2012Tiara NurhasanahNo ratings yet
- 15l8m04Document4 pages15l8m04chd9r5hr5kNo ratings yet
- Histopathological Insight of An Adenomatoid Odontogenic Lesion - A Cyst, Tumor or Hamartoma?Document6 pagesHistopathological Insight of An Adenomatoid Odontogenic Lesion - A Cyst, Tumor or Hamartoma?gunawan121982No ratings yet
- Dentigerous Cyst: A Retrospective Study of 20 Cases in S. S. Medical College Rewa, Madhya PradeshDocument4 pagesDentigerous Cyst: A Retrospective Study of 20 Cases in S. S. Medical College Rewa, Madhya PradeshnjmdrNo ratings yet
- Primary Ameloblastic Carcinoma of The Maxilla A CaDocument9 pagesPrimary Ameloblastic Carcinoma of The Maxilla A CaMuhammad Avicenna AdjiNo ratings yet
- Cholesteatoma of External Auditory CanalDocument5 pagesCholesteatoma of External Auditory CanallolNo ratings yet
- Squamous Cell Carcinoma of The Mandibular Gingiva: Pei-Yu Li, DDS Ling Auyeung, DDS, MS Shun-Chen Huang, MDDocument5 pagesSquamous Cell Carcinoma of The Mandibular Gingiva: Pei-Yu Li, DDS Ling Auyeung, DDS, MS Shun-Chen Huang, MDtsntiNo ratings yet
- dmf2SA Presentasi01Document5 pagesdmf2SA Presentasi01Iftinan LQNo ratings yet
- TOECDocument4 pagesTOECSaul SilvaNo ratings yet
- Li Tiejun2006Document8 pagesLi Tiejun2006Herpika DianaNo ratings yet
- Osteosarcoma of Mandible: Abst TDocument3 pagesOsteosarcoma of Mandible: Abst TTriLightNo ratings yet
- An Expanded Odontogenic Myxoma in MaxillaDocument7 pagesAn Expanded Odontogenic Myxoma in MaxillaHerpika DianaNo ratings yet
- International Journal of Dental Science and Innovative Research (IJDSIR)Document7 pagesInternational Journal of Dental Science and Innovative Research (IJDSIR)bella07ciaoNo ratings yet
- Cemento-Ossifying Fibroma of The Mandible: Presentation of A Case and Review of The LiteratureDocument5 pagesCemento-Ossifying Fibroma of The Mandible: Presentation of A Case and Review of The LiteratureMutia Martha HeldaNo ratings yet
- Crim Medicine2013-407967Document3 pagesCrim Medicine2013-407967Greisy Saym Cruz FelixNo ratings yet
- Clinical Case Reports - 2022 - Khalifa - Compound Complex Odontoma A Rare Case ReportDocument4 pagesClinical Case Reports - 2022 - Khalifa - Compound Complex Odontoma A Rare Case ReportAlbert OliveraNo ratings yet
- Ijohns 2018081616134070Document5 pagesIjohns 2018081616134070alifaNo ratings yet
- Cystic Mass of The Floor of The MouthDocument4 pagesCystic Mass of The Floor of The MouthMARIA KARINA HERNANDEZ PEREZNo ratings yet
- Case Report: ISPUB - An Unusual Case of Unicystic Ameloblastoma Involvi..Document3 pagesCase Report: ISPUB - An Unusual Case of Unicystic Ameloblastoma Involvi..johnnychickenfootNo ratings yet
- Amhsr 3 285Document3 pagesAmhsr 3 285Dwi Dayanti AgustinaNo ratings yet
- Treatmen AotDocument5 pagesTreatmen Aotgunawanmulyana12No ratings yet
- Unicystic Ameloblastoma in A 23 Year Old Male: A Case: Richa Wadhawan, Bhuvnesh Sharma, Pulkit Sharma and Dharti GajjarDocument6 pagesUnicystic Ameloblastoma in A 23 Year Old Male: A Case: Richa Wadhawan, Bhuvnesh Sharma, Pulkit Sharma and Dharti GajjarTriana Amaliah JayantiNo ratings yet
- Non-Syndromic Multiple Odontogenic Keratocyst A Case ReportDocument7 pagesNon-Syndromic Multiple Odontogenic Keratocyst A Case ReportReza ApriandiNo ratings yet
- OHNS--Otolaryngology; Head and Neck surgery: pocket field guideFrom EverandOHNS--Otolaryngology; Head and Neck surgery: pocket field guideNo ratings yet
- Frequencies: StatisticsDocument5 pagesFrequencies: StatisticsEzza RiezaNo ratings yet
- Australian Dental Journal: The Contemporary Management of Third MolarsDocument8 pagesAustralian Dental Journal: The Contemporary Management of Third MolarsEzza RiezaNo ratings yet
- The Effect of Various Classes of Malocclusions On The Maxillary Arch Forms and Dimensions in Jordanian PopulationDocument7 pagesThe Effect of Various Classes of Malocclusions On The Maxillary Arch Forms and Dimensions in Jordanian PopulationEzza RiezaNo ratings yet
- Lembaran Rekap PedodonsiaDocument1 pageLembaran Rekap PedodonsiaEzza RiezaNo ratings yet
- 2212 4403Document18 pages2212 4403Ezza RiezaNo ratings yet
- Kista Odontogenik Di Rumah Sakit Dr. Wahidin Sudirohusodo MakassarDocument8 pagesKista Odontogenik Di Rumah Sakit Dr. Wahidin Sudirohusodo MakassarEzza RiezaNo ratings yet
- Ameloblastoma: A Clinical Review and Trends in ManagementDocument13 pagesAmeloblastoma: A Clinical Review and Trends in ManagementEzza RiezaNo ratings yet
- Farooq 2000Document9 pagesFarooq 2000Ezza RiezaNo ratings yet
- Research Article: Effectiveness of Mouth Washes On Streptococci in Plaque Around Orthodontic AppliancesDocument5 pagesResearch Article: Effectiveness of Mouth Washes On Streptococci in Plaque Around Orthodontic AppliancesEzza RiezaNo ratings yet
- In the name of God: Dr.Mahtab Nouri لاوس و یدنب عمج مھدفھ هسلجDocument21 pagesIn the name of God: Dr.Mahtab Nouri لاوس و یدنب عمج مھدفھ هسلجEzza RiezaNo ratings yet
- 1-The Etiology of Orthodontic ProblemsDocument47 pages1-The Etiology of Orthodontic ProblemsEzza RiezaNo ratings yet
- Periapical GranulomaDocument6 pagesPeriapical GranulomaEzza RiezaNo ratings yet
- Radicular Cyst: A Case Report: Harshitha KR, Varsha VK, Deepa. CDocument3 pagesRadicular Cyst: A Case Report: Harshitha KR, Varsha VK, Deepa. CEzza RiezaNo ratings yet
- Management of Infected Radicular Cyst by Surgical Approach: Case ReportDocument2 pagesManagement of Infected Radicular Cyst by Surgical Approach: Case ReportEzza RiezaNo ratings yet
- TP. 2 REVISION PTE SIMPLE - Grammar ExcercisesDocument3 pagesTP. 2 REVISION PTE SIMPLE - Grammar ExcercisesgabyNo ratings yet
- Final DraftDocument37 pagesFinal DraftMorareng MariettaNo ratings yet
- Perioperative Nursing Cesarean SectionDocument13 pagesPerioperative Nursing Cesarean Sectionmark OrpillaNo ratings yet
- Set3 PDFDocument36 pagesSet3 PDFvishwas100% (1)
- RHU Situanional ReportDocument8 pagesRHU Situanional ReportErnest AtonNo ratings yet
- Prolapse Lumbar DiscDocument40 pagesProlapse Lumbar DiscAlfred BantigueNo ratings yet
- 6 Halides (My Lecture) - HandoutDocument12 pages6 Halides (My Lecture) - HandoutStanliNo ratings yet
- PC3SH21YFZBFDocument15 pagesPC3SH21YFZBFkrimoNo ratings yet
- Layering With Colored PencilsDocument2 pagesLayering With Colored PencilsfrankcarabanoNo ratings yet
- Unit IV-Alternative Laboratory ExerciseDocument11 pagesUnit IV-Alternative Laboratory ExerciseFloralde RyanNo ratings yet
- Activated Carbon From BambooDocument19 pagesActivated Carbon From BambooErik WeeksNo ratings yet
- Quiet Healing Center Auroville PDFDocument7 pagesQuiet Healing Center Auroville PDFananya k sNo ratings yet
- Electrical Inspectorate (11-15)Document5 pagesElectrical Inspectorate (11-15)Aravind NkNo ratings yet
- Review of Agriculture Robotics: Practicality and FeasibilityDocument6 pagesReview of Agriculture Robotics: Practicality and Feasibilityaldy faleraNo ratings yet
- Definition of Terms Mine SurveyingDocument2 pagesDefinition of Terms Mine Surveyingaquariuspj25100% (3)
- Liabilities and EquityDocument23 pagesLiabilities and Equityadmiral spongebobNo ratings yet
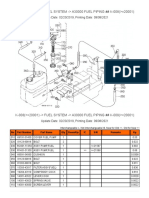
- K-008 ( 20001) - Fuel System - A30000 Fuel Piping ## K-008 ( 20001)Document2 pagesK-008 ( 20001) - Fuel System - A30000 Fuel Piping ## K-008 ( 20001)Martin LindbergNo ratings yet
- Prime MX FIRA 6250 2018Document4 pagesPrime MX FIRA 6250 2018hodlab designcoNo ratings yet
- LL. B. I Term: Paper - LB - 103 - Law of TortsDocument10 pagesLL. B. I Term: Paper - LB - 103 - Law of TortsFaisal ShahzadNo ratings yet
- Improving Fast-Food Restaurants' Method of Operation: Automated Drive-Through Ordering SystemDocument12 pagesImproving Fast-Food Restaurants' Method of Operation: Automated Drive-Through Ordering SystemAllin John FranciscoNo ratings yet
- Build 443Document5 pagesBuild 443mh_tadayonNo ratings yet
- LV Panel ReportDocument71 pagesLV Panel ReportMudassirNo ratings yet
- D154-85 (2009) Standard Guide For Testing VarnishesDocument4 pagesD154-85 (2009) Standard Guide For Testing VarnishesRonny100% (1)
- Weathering and Organic Processes Form Soil.: What Makes Soils Different?Document8 pagesWeathering and Organic Processes Form Soil.: What Makes Soils Different?Precious BalgunaNo ratings yet
- Annex 3 - 5-Revised EMFDocument3 pagesAnnex 3 - 5-Revised EMFVholts Villa VitugNo ratings yet
- Chapter - 10: Reaching The Age of AdolescenceDocument11 pagesChapter - 10: Reaching The Age of AdolescenceDestroy YtNo ratings yet
- Ron Arwin Nathaniel G. Palmares 10 - PAscal EngDocument7 pagesRon Arwin Nathaniel G. Palmares 10 - PAscal Engron arwin nathaniel palmaresNo ratings yet
- Soil Moisture Monitoring - One-SheeterDocument2 pagesSoil Moisture Monitoring - One-SheeterSorin BurleaNo ratings yet
- Perkins Spares 80,100Document10 pagesPerkins Spares 80,100ramsey222No ratings yet
- BiochemistryDocument68 pagesBiochemistry20AR018 HARIHARA SUBRAMANIANNo ratings yet