Download as doc, pdf, or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5822)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Practical Research 1 Summative TestDocument3 pagesPractical Research 1 Summative Testjovy dulay93% (28)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Bruno Groening 1957-10-05 Talk I Know That It Is Very Difficult 1 ColDocument57 pagesBruno Groening 1957-10-05 Talk I Know That It Is Very Difficult 1 Colarturobandini1975100% (1)
- Intratympanic Membrane Congenital CholesteatomaDocument3 pagesIntratympanic Membrane Congenital CholesteatomajaneNo ratings yet
- Radiology Icm IiDocument8 pagesRadiology Icm IijaneNo ratings yet
- NIH Public Access: Delayed Antimicrobial Therapy Increases Mortality and Organ Dysfunction Duration in Pediatric SepsisDocument23 pagesNIH Public Access: Delayed Antimicrobial Therapy Increases Mortality and Organ Dysfunction Duration in Pediatric SepsisjaneNo ratings yet
- Medical Leadership Competency Framework: Landscape of HealthcareDocument15 pagesMedical Leadership Competency Framework: Landscape of HealthcarejaneNo ratings yet
- Lymphokines & Cytokines: Immunology & DiseaseDocument34 pagesLymphokines & Cytokines: Immunology & DiseasejaneNo ratings yet
- Antidepressants AntidepressantsDocument38 pagesAntidepressants AntidepressantsjaneNo ratings yet
- Itching, Redness of The SkinDocument21 pagesItching, Redness of The SkinjaneNo ratings yet
- Substance Abuse Among Health Professionals: August 15, 2014Document25 pagesSubstance Abuse Among Health Professionals: August 15, 2014janeNo ratings yet
- By: Dr. Engelberta Sp. KJDocument14 pagesBy: Dr. Engelberta Sp. KJjaneNo ratings yet
- Mechanisms of Antibiotic Resistance in BacteriaDocument41 pagesMechanisms of Antibiotic Resistance in BacteriajaneNo ratings yet
- JawsDocument78 pagesJawsjaneNo ratings yet
- To Physiology, Homeostasis, and Body Temperature: V. Sutarmo SetiadjiDocument20 pagesTo Physiology, Homeostasis, and Body Temperature: V. Sutarmo SetiadjijaneNo ratings yet
- Mechanisms of Antibiotic Resistance in BacteriaDocument40 pagesMechanisms of Antibiotic Resistance in BacteriajaneNo ratings yet
- Transient Loss of Consciousness: History TakingDocument4 pagesTransient Loss of Consciousness: History TakingjaneNo ratings yet
- LibraryDocument1 pageLibraryjaneNo ratings yet
- COMMUNICATION With Other ProfessionalsDocument12 pagesCOMMUNICATION With Other ProfessionalsjaneNo ratings yet
- STM Cels Lcture 1Document44 pagesSTM Cels Lcture 1janeNo ratings yet
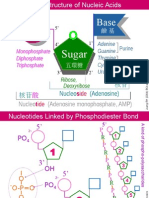
- NA01 StructureDocument5 pagesNA01 StructurejaneNo ratings yet
- Managerial Psychology in Action AssignmentDocument3 pagesManagerial Psychology in Action Assignmentpooja shutradharNo ratings yet
- Chapter One To Five Pde WorkDocument30 pagesChapter One To Five Pde WorkSMART ROBITONo ratings yet
- GKB1053 Kemahiran Belajar: Abdul Jasheer JayaseelanDocument12 pagesGKB1053 Kemahiran Belajar: Abdul Jasheer JayaseelanPei Rui KoiNo ratings yet
- Literature Review Example in PsychologyDocument5 pagesLiterature Review Example in Psychologyafmzbufoeifoof100% (1)
- CBE6100 Strategy Formulation Exam PaperDocument1 pageCBE6100 Strategy Formulation Exam PaperArber I. GashiNo ratings yet
- A History of Women Philosophers Vol. IV - Mary Ellen WaitheDocument503 pagesA History of Women Philosophers Vol. IV - Mary Ellen WaitheEdisonReatiquiNo ratings yet
- XLRI Asynchronous Interview GuideDocument3 pagesXLRI Asynchronous Interview GuideAprilNo ratings yet
- Theory in The PracticeDocument49 pagesTheory in The Practiceton copy Service100% (1)
- COT Watch MaterialDocument6 pagesCOT Watch MaterialRay PatriarcaNo ratings yet
- Learning Evidence: Listening: Name Account Date Choose A L, and Write The Following Information. Web: TopicDocument3 pagesLearning Evidence: Listening: Name Account Date Choose A L, and Write The Following Information. Web: TopicBelen HinojosaNo ratings yet
- KARANDINOU, Anastasia. Invisible TectonicsDocument4 pagesKARANDINOU, Anastasia. Invisible TectonicsbsceciliaNo ratings yet
- Remedial Instruction in EnglishDocument9 pagesRemedial Instruction in EnglishShar Nur JeanNo ratings yet
- The Power of Visual Communication Apr17Document18 pagesThe Power of Visual Communication Apr17yojiyanNo ratings yet
- Social Learning Theory: Albert BanduraDocument20 pagesSocial Learning Theory: Albert BandurahNo ratings yet
- REIKI Level I Ebook - PDF 2Document46 pagesREIKI Level I Ebook - PDF 2Alisha AllisonNo ratings yet
- ADEC - Abu Mousa Al Ashaari Private School 2016-2017Document18 pagesADEC - Abu Mousa Al Ashaari Private School 2016-2017Edarabia.comNo ratings yet
- Every Individual Has A Unique Spiritual JourneyDocument2 pagesEvery Individual Has A Unique Spiritual JourneycheyeenNo ratings yet
- Family Planning by G A Parwez Published by Idara Tulu-E-IslamDocument44 pagesFamily Planning by G A Parwez Published by Idara Tulu-E-Islamadil100% (1)
- Sat Study GuideDocument287 pagesSat Study GuideDieorLiveFreeNo ratings yet
- Kundalini BookDocument140 pagesKundalini BookManjunath Yattinagudd100% (5)
- HR Resume SampleDocument3 pagesHR Resume SamplebalakrishnaNo ratings yet
- Narrative Therapies With Children and Adolescents - PDF - Page - 31 - 82Document52 pagesNarrative Therapies With Children and Adolescents - PDF - Page - 31 - 82Diego Reyes Barría100% (1)
- Essentials of Modern Business Statistics (7e) : Anderson, Sweeney, Williams, Camm, CochranDocument57 pagesEssentials of Modern Business Statistics (7e) : Anderson, Sweeney, Williams, Camm, CochranIdate PatrickNo ratings yet
- Hyperactivity and Impulsivity in Children - ADHD Symptom TestDocument9 pagesHyperactivity and Impulsivity in Children - ADHD Symptom TestMustafa AlmasoudiNo ratings yet
- Lesson 6-General Notion of InferenceDocument2 pagesLesson 6-General Notion of Inferencejeanivev magonciaNo ratings yet
- Iep Team MemberDocument2 pagesIep Team Memberapi-284091048No ratings yet
- Chapter 5Document21 pagesChapter 5Methusheila Moral100% (1)
- Organizational Conflict: - A Process ThatDocument13 pagesOrganizational Conflict: - A Process ThatDoina BejanNo ratings yet