
New York, N. Y.: Joseph Landa
New York, N. Y.: Joseph Landa
You might also like
- Blood Brain Barrier PDFDocument6 pagesBlood Brain Barrier PDFmanoj_rkl_07100% (1)
- Prosthetic Management of Soft Palate Defects: Presented byDocument57 pagesProsthetic Management of Soft Palate Defects: Presented byPiyush DongreNo ratings yet
- Chapter V - Human Anatomy: 7-Resources & Indexes Module 8-AbbreviationsDocument4 pagesChapter V - Human Anatomy: 7-Resources & Indexes Module 8-AbbreviationsIndranil SinhaNo ratings yet
- Anatomy & Physiology of SwallowingDocument6 pagesAnatomy & Physiology of Swallowingbagir_dm10No ratings yet
- Anatomy and Development of Oral Cavity and PharynxDocument14 pagesAnatomy and Development of Oral Cavity and PharynxGabriela MacoveanuNo ratings yet
- Oral Diseases - 2013 - Logemann - 231025 - 203119Document5 pagesOral Diseases - 2013 - Logemann - 231025 - 203119rpediatrica2023No ratings yet
- Physiology of LarynxDocument26 pagesPhysiology of Larynxmadhumitha srinivasNo ratings yet
- Anatomy Physio AnesthesiaDocument6 pagesAnatomy Physio AnesthesiaMarites L. DomingoNo ratings yet
- Management of The Patient With Laryngitis1Document14 pagesManagement of The Patient With Laryngitis1Alina AluculeseiNo ratings yet
- SwallowingDocument5 pagesSwallowingsamazicsNo ratings yet
- Anatomy and Physiology of PharynxDocument16 pagesAnatomy and Physiology of Pharynxaleeza nomanNo ratings yet
- Posterior Palatal SealDocument74 pagesPosterior Palatal SealAmit Bhargav50% (2)
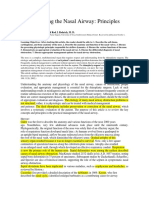
- Understanding The Nasal AirwayDocument21 pagesUnderstanding The Nasal AirwayGera AguilarNo ratings yet
- Laryngeal ManipulationDocument18 pagesLaryngeal ManipulationtaniaNo ratings yet
- Upper AirwayDocument37 pagesUpper AirwayWakilAhmad100% (1)
- Ear, Nose and ThroatDocument23 pagesEar, Nose and ThroatWizz Háķìm ĻêşòwNo ratings yet
- Aging Voice Presbyphocia - MARTINS ET AL 2013Document5 pagesAging Voice Presbyphocia - MARTINS ET AL 2013FonoaudiologiaNo ratings yet
- Upper Airway Anatomy and FunctionDocument86 pagesUpper Airway Anatomy and FunctionekaefkaNo ratings yet
- Ratnaike2002 Disfagia en Adulto MayorDocument13 pagesRatnaike2002 Disfagia en Adulto MayorAngelica Maria LizarazoNo ratings yet
- ANATOMY 18.04.18 Camille EleonoraDocument14 pagesANATOMY 18.04.18 Camille Eleonoraomer.buzagloNo ratings yet
- Erbil Polythecnic University Soran Technical Insititute Midwifery Dipartment First Stage (M)Document13 pagesErbil Polythecnic University Soran Technical Insititute Midwifery Dipartment First Stage (M)Kubra ĖdrisNo ratings yet
- Anatomy Final All Questions (New)Document175 pagesAnatomy Final All Questions (New)Sevval OzcelikNo ratings yet
- Clinical Anatomy, Physiology and Methods of Examination of The Pharynx. Acute and Chronic Tonsillitis and Their Complications. Hypertrophy of The Lymph Tissue of The PharynxDocument55 pagesClinical Anatomy, Physiology and Methods of Examination of The Pharynx. Acute and Chronic Tonsillitis and Their Complications. Hypertrophy of The Lymph Tissue of The PharynxNicolás Barrios MagnaNo ratings yet
- Laryngeal SeparationDocument27 pagesLaryngeal Separationhossamh3No ratings yet
- 1 Swallowing Disorders: Jeri A. LogemannDocument11 pages1 Swallowing Disorders: Jeri A. LogemannSamuel Felipe Avendaño SilvaNo ratings yet
- Pharynx NotesDocument8 pagesPharynx Notesm0rat0r1umNo ratings yet
- Exercise7 (Histo) Digestive System EditedDocument8 pagesExercise7 (Histo) Digestive System EditedChristi Lorraine LayogNo ratings yet
- Upperairway Anatomy and FunctionDocument86 pagesUpperairway Anatomy and Functionifran kandouNo ratings yet
- Cephalometric Evaluation and Measurement of The Upper Airway PDFDocument13 pagesCephalometric Evaluation and Measurement of The Upper Airway PDFSoe San KyawNo ratings yet
- Upper Nasal AirwayDocument23 pagesUpper Nasal AirwayKapil ThakerNo ratings yet
- Goldsmith 2000Document24 pagesGoldsmith 2000valeperoneNo ratings yet
- Pap 0106Document31 pagesPap 0106Bogdan PraščevićNo ratings yet
- A Complete Three-Dimensional Reconstruction of The Myoanatomy of Loricifera: Comparative Morphology of An Adult and A Higgins Larva StageDocument21 pagesA Complete Three-Dimensional Reconstruction of The Myoanatomy of Loricifera: Comparative Morphology of An Adult and A Higgins Larva StageReizascs100% (1)
- Dysphagia in Lateral Medullary Syndrome ObjavljenDocument10 pagesDysphagia in Lateral Medullary Syndrome ObjavljenMala MirnaNo ratings yet
- 18.19 the-role-of-the-supraglottic-area-in-voice-production-2161-119X.S1-001Document7 pages18.19 the-role-of-the-supraglottic-area-in-voice-production-2161-119X.S1-001Diana Carolina Cerón EstradaNo ratings yet
- Vose-Humbert2019 Article HiddenInPlainSightADescriptiveDocument9 pagesVose-Humbert2019 Article HiddenInPlainSightADescriptiveAnna AgenteNo ratings yet
- Apnea de Sueño-ResumenDocument6 pagesApnea de Sueño-ResumenmhidvenNo ratings yet
- Respiratory SystemDocument8 pagesRespiratory SystemAlther LorenNo ratings yet
- Chapter 9: Anatomy and Physiology of The Salivary Glands O. H. ShaheenDocument18 pagesChapter 9: Anatomy and Physiology of The Salivary Glands O. H. ShaheenGirish SubashNo ratings yet
- The Nasal Septum PDFDocument18 pagesThe Nasal Septum PDFalit100% (1)
- Digestive System Part 1Document10 pagesDigestive System Part 1bazingaNo ratings yet
- 11 PharynxDocument8 pages11 PharynxNur Ain Faezah RoslanNo ratings yet
- Nils Gunnar Toremalm: Chapter 120: Physiology TracheaDocument14 pagesNils Gunnar Toremalm: Chapter 120: Physiology TracheaSteven WilsonNo ratings yet
- Treatise on the Anatomy and Physiology of the Mucous Membranes: With Illustrative Pathological ObservationsFrom EverandTreatise on the Anatomy and Physiology of the Mucous Membranes: With Illustrative Pathological ObservationsNo ratings yet
- Respiratory SystemDocument12 pagesRespiratory SystemshreyacrkNo ratings yet
- Biol 122L Exercise 11Document10 pagesBiol 122L Exercise 11Shaira Jean SollanoNo ratings yet
- Anatomy of The Pharynx: Dr. Oscar Djauhari, Sp. THT-KLDocument18 pagesAnatomy of The Pharynx: Dr. Oscar Djauhari, Sp. THT-KLrizkauliaherNo ratings yet
- Nasopharynx SB AnatomyDocument6 pagesNasopharynx SB AnatomykyawzwarmgNo ratings yet
- Silverman 1971Document19 pagesSilverman 1971Krupali JainNo ratings yet
- Airway Management in The Adult - Miller's Anesthesia 2009Document38 pagesAirway Management in The Adult - Miller's Anesthesia 2009UrgenciasCol FoamNo ratings yet
- Mastication and Swallowing L4Document28 pagesMastication and Swallowing L4Siphelele MkhatshwaNo ratings yet
- Benumof Anatomia Via AereaDocument11 pagesBenumof Anatomia Via AereaMaria RicardoNo ratings yet
- Chapter 10 - Respiratory System - 2020 - The Zebrafish in Biomedical ResearchDocument5 pagesChapter 10 - Respiratory System - 2020 - The Zebrafish in Biomedical ResearchNicolas BaronNo ratings yet
- Human Digestive System, The System Used in TheDocument10 pagesHuman Digestive System, The System Used in Theعلي رسن رداد حمد ANo ratings yet
- Chapter 13 Surgical Managment of Salivary Gland DiseaseDocument35 pagesChapter 13 Surgical Managment of Salivary Gland DiseaseMohammed Qasim Al-WataryNo ratings yet
- Management of The Patient With Laryngitis: James Paul Dworkin P D& Robert J. Stachler MDDocument40 pagesManagement of The Patient With Laryngitis: James Paul Dworkin P D& Robert J. Stachler MDoneagustinNo ratings yet
- Fig. 1 - The Esophagus (Front and Right)Document23 pagesFig. 1 - The Esophagus (Front and Right)Ella JonesNo ratings yet
- 3 PharyngologyDocument86 pages3 PharyngologyWai Kwong Chiu100% (1)
- An Overview of Presbyphagia: Tinjauan PustakaDocument8 pagesAn Overview of Presbyphagia: Tinjauan PustakaMuhammad FarhanNo ratings yet
- Piazza 2010Document11 pagesPiazza 2010Israel BlancoNo ratings yet
- CHSJ 40 3 200Document5 pagesCHSJ 40 3 200Idelia GunawanNo ratings yet
- Twin BlockDocument5 pagesTwin BlockIdelia GunawanNo ratings yet
- Prevalensi MalocclusionDocument5 pagesPrevalensi MalocclusionIdelia GunawanNo ratings yet
- Down SyndromeDocument3 pagesDown SyndromeIdelia GunawanNo ratings yet
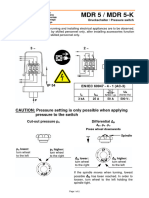
- Pressure Switch MDR5Document4 pagesPressure Switch MDR5Fidelis NdanoNo ratings yet
- Solar MPPT PresentationDocument21 pagesSolar MPPT PresentationPravat SatpathyNo ratings yet
- Uses of RefractoryDocument20 pagesUses of RefractoryRicha Tripathi100% (2)
- Training Report of IoclDocument68 pagesTraining Report of IoclAnupam SrivastavNo ratings yet
- Interviw With Martin DavisDocument12 pagesInterviw With Martin DavisraktimddkNo ratings yet
- Smart Dallas RoadmapDocument45 pagesSmart Dallas RoadmapAshish MohanNo ratings yet
- 415V CALCULATING SHEET AND SETTING LIST FOR EQUIPMENT PROTECTION OF CHP WAGON TIPPER AND ESP (Supplement For Zero Sequence Current Relay)Document25 pages415V CALCULATING SHEET AND SETTING LIST FOR EQUIPMENT PROTECTION OF CHP WAGON TIPPER AND ESP (Supplement For Zero Sequence Current Relay)Amaresh NayakNo ratings yet
- The Stall Chart - Varying Flow Secondary - Constant Inlet Temperature - Constant Outlet TemperatureDocument8 pagesThe Stall Chart - Varying Flow Secondary - Constant Inlet Temperature - Constant Outlet TemperatureSandra FerrellNo ratings yet
- Neptune Planet Experiment, Ariny Amos (Astronomer) - 1Document1,139 pagesNeptune Planet Experiment, Ariny Amos (Astronomer) - 1Dr. Amos ArinyNo ratings yet
- Appendix 11 Design FMEA ChecklistDocument16 pagesAppendix 11 Design FMEA ChecklistDearRed FrankNo ratings yet
- MCO 3 (30/3-3/4/2020) Reinforcement Chapter 2 Part A: Objective QuestionsDocument5 pagesMCO 3 (30/3-3/4/2020) Reinforcement Chapter 2 Part A: Objective QuestionsZalini AbdullahNo ratings yet
- Unit 2 Psychophysics: Threshold, Signal Detection Theory: StructureDocument10 pagesUnit 2 Psychophysics: Threshold, Signal Detection Theory: StructuresanoopsrajNo ratings yet
- Extreme Cold Weather (ECW) ClothingDocument7 pagesExtreme Cold Weather (ECW) ClothingSnowshadowNo ratings yet
- Chapter 4 - Structural Imperfections Kingery Introducción A Los Materiales CerámicosDocument27 pagesChapter 4 - Structural Imperfections Kingery Introducción A Los Materiales CerámicosLaura BárbaroNo ratings yet
- Conduit Trunking Capacity Chart RM TechnicalDocument1 pageConduit Trunking Capacity Chart RM TechnicalPrabir BhowmikNo ratings yet
- CL 55-60 AnDocument14 pagesCL 55-60 AnFrida KahloNo ratings yet
- 2017 District Superintendent ReportDocument12 pages2017 District Superintendent ReportRob Steinbrook100% (1)
- Initial Newborn AssessmentDocument14 pagesInitial Newborn Assessmentaclark831No ratings yet
- Fashion Through The Decades PowerpointDocument11 pagesFashion Through The Decades PowerpointNigar khanNo ratings yet
- Mesología BERQUEDocument6 pagesMesología BERQUEPanchita PonisioNo ratings yet
- Research Report - Aakanksha MistryDocument19 pagesResearch Report - Aakanksha MistryAakanksha MistryNo ratings yet
- 2015 - Soil Mechanics II - Final - enDocument7 pages2015 - Soil Mechanics II - Final - enjohn cambixNo ratings yet
- Accepted Manuscript: Diabetes & Metabolic Syndrome: Clinical Research & ReviewsDocument43 pagesAccepted Manuscript: Diabetes & Metabolic Syndrome: Clinical Research & ReviewsYanet FrancoNo ratings yet
- How To Start A Candle BusinessDocument49 pagesHow To Start A Candle BusinessJessica Rodrigo100% (1)
- Logg 4000Document7 pagesLogg 4000Stjepan FrljicNo ratings yet
- Tax Invoice/Bill of Supply/Cash Memo: (Original For Recipient)Document1 pageTax Invoice/Bill of Supply/Cash Memo: (Original For Recipient)Ch PrasadNo ratings yet
- Huawei FusionSolar Smart PV SolutionDocument32 pagesHuawei FusionSolar Smart PV SolutionJOGmzNo ratings yet
- Capacity PlanDocument1 pageCapacity PlanbishnuNo ratings yet
- Biology Q & A Booklet: (English Medium)Document76 pagesBiology Q & A Booklet: (English Medium)La EscenaNo ratings yet



























































































Download as pdf or txt
You might also like
- Blood Brain Barrier PDFDocument6 pagesBlood Brain Barrier PDFmanoj_rkl_07100% (1)
- Prosthetic Management of Soft Palate Defects: Presented byDocument57 pagesProsthetic Management of Soft Palate Defects: Presented byPiyush DongreNo ratings yet
- Chapter V - Human Anatomy: 7-Resources & Indexes Module 8-AbbreviationsDocument4 pagesChapter V - Human Anatomy: 7-Resources & Indexes Module 8-AbbreviationsIndranil SinhaNo ratings yet
- Anatomy & Physiology of SwallowingDocument6 pagesAnatomy & Physiology of Swallowingbagir_dm10No ratings yet
- Anatomy and Development of Oral Cavity and PharynxDocument14 pagesAnatomy and Development of Oral Cavity and PharynxGabriela MacoveanuNo ratings yet
- Oral Diseases - 2013 - Logemann - 231025 - 203119Document5 pagesOral Diseases - 2013 - Logemann - 231025 - 203119rpediatrica2023No ratings yet
- Physiology of LarynxDocument26 pagesPhysiology of Larynxmadhumitha srinivasNo ratings yet
- Anatomy Physio AnesthesiaDocument6 pagesAnatomy Physio AnesthesiaMarites L. DomingoNo ratings yet
- Management of The Patient With Laryngitis1Document14 pagesManagement of The Patient With Laryngitis1Alina AluculeseiNo ratings yet
- SwallowingDocument5 pagesSwallowingsamazicsNo ratings yet
- Anatomy and Physiology of PharynxDocument16 pagesAnatomy and Physiology of Pharynxaleeza nomanNo ratings yet
- Posterior Palatal SealDocument74 pagesPosterior Palatal SealAmit Bhargav50% (2)
- Understanding The Nasal AirwayDocument21 pagesUnderstanding The Nasal AirwayGera AguilarNo ratings yet
- Laryngeal ManipulationDocument18 pagesLaryngeal ManipulationtaniaNo ratings yet
- Upper AirwayDocument37 pagesUpper AirwayWakilAhmad100% (1)
- Ear, Nose and ThroatDocument23 pagesEar, Nose and ThroatWizz Háķìm ĻêşòwNo ratings yet
- Aging Voice Presbyphocia - MARTINS ET AL 2013Document5 pagesAging Voice Presbyphocia - MARTINS ET AL 2013FonoaudiologiaNo ratings yet
- Upper Airway Anatomy and FunctionDocument86 pagesUpper Airway Anatomy and FunctionekaefkaNo ratings yet
- Ratnaike2002 Disfagia en Adulto MayorDocument13 pagesRatnaike2002 Disfagia en Adulto MayorAngelica Maria LizarazoNo ratings yet
- ANATOMY 18.04.18 Camille EleonoraDocument14 pagesANATOMY 18.04.18 Camille Eleonoraomer.buzagloNo ratings yet
- Erbil Polythecnic University Soran Technical Insititute Midwifery Dipartment First Stage (M)Document13 pagesErbil Polythecnic University Soran Technical Insititute Midwifery Dipartment First Stage (M)Kubra ĖdrisNo ratings yet
- Anatomy Final All Questions (New)Document175 pagesAnatomy Final All Questions (New)Sevval OzcelikNo ratings yet
- Clinical Anatomy, Physiology and Methods of Examination of The Pharynx. Acute and Chronic Tonsillitis and Their Complications. Hypertrophy of The Lymph Tissue of The PharynxDocument55 pagesClinical Anatomy, Physiology and Methods of Examination of The Pharynx. Acute and Chronic Tonsillitis and Their Complications. Hypertrophy of The Lymph Tissue of The PharynxNicolás Barrios MagnaNo ratings yet
- Laryngeal SeparationDocument27 pagesLaryngeal Separationhossamh3No ratings yet
- 1 Swallowing Disorders: Jeri A. LogemannDocument11 pages1 Swallowing Disorders: Jeri A. LogemannSamuel Felipe Avendaño SilvaNo ratings yet
- Pharynx NotesDocument8 pagesPharynx Notesm0rat0r1umNo ratings yet
- Exercise7 (Histo) Digestive System EditedDocument8 pagesExercise7 (Histo) Digestive System EditedChristi Lorraine LayogNo ratings yet
- Upperairway Anatomy and FunctionDocument86 pagesUpperairway Anatomy and Functionifran kandouNo ratings yet
- Cephalometric Evaluation and Measurement of The Upper Airway PDFDocument13 pagesCephalometric Evaluation and Measurement of The Upper Airway PDFSoe San KyawNo ratings yet
- Upper Nasal AirwayDocument23 pagesUpper Nasal AirwayKapil ThakerNo ratings yet
- Goldsmith 2000Document24 pagesGoldsmith 2000valeperoneNo ratings yet
- Pap 0106Document31 pagesPap 0106Bogdan PraščevićNo ratings yet
- A Complete Three-Dimensional Reconstruction of The Myoanatomy of Loricifera: Comparative Morphology of An Adult and A Higgins Larva StageDocument21 pagesA Complete Three-Dimensional Reconstruction of The Myoanatomy of Loricifera: Comparative Morphology of An Adult and A Higgins Larva StageReizascs100% (1)
- Dysphagia in Lateral Medullary Syndrome ObjavljenDocument10 pagesDysphagia in Lateral Medullary Syndrome ObjavljenMala MirnaNo ratings yet
- 18.19 the-role-of-the-supraglottic-area-in-voice-production-2161-119X.S1-001Document7 pages18.19 the-role-of-the-supraglottic-area-in-voice-production-2161-119X.S1-001Diana Carolina Cerón EstradaNo ratings yet
- Vose-Humbert2019 Article HiddenInPlainSightADescriptiveDocument9 pagesVose-Humbert2019 Article HiddenInPlainSightADescriptiveAnna AgenteNo ratings yet
- Apnea de Sueño-ResumenDocument6 pagesApnea de Sueño-ResumenmhidvenNo ratings yet
- Respiratory SystemDocument8 pagesRespiratory SystemAlther LorenNo ratings yet
- Chapter 9: Anatomy and Physiology of The Salivary Glands O. H. ShaheenDocument18 pagesChapter 9: Anatomy and Physiology of The Salivary Glands O. H. ShaheenGirish SubashNo ratings yet
- The Nasal Septum PDFDocument18 pagesThe Nasal Septum PDFalit100% (1)
- Digestive System Part 1Document10 pagesDigestive System Part 1bazingaNo ratings yet
- 11 PharynxDocument8 pages11 PharynxNur Ain Faezah RoslanNo ratings yet
- Nils Gunnar Toremalm: Chapter 120: Physiology TracheaDocument14 pagesNils Gunnar Toremalm: Chapter 120: Physiology TracheaSteven WilsonNo ratings yet
- Treatise on the Anatomy and Physiology of the Mucous Membranes: With Illustrative Pathological ObservationsFrom EverandTreatise on the Anatomy and Physiology of the Mucous Membranes: With Illustrative Pathological ObservationsNo ratings yet
- Respiratory SystemDocument12 pagesRespiratory SystemshreyacrkNo ratings yet
- Biol 122L Exercise 11Document10 pagesBiol 122L Exercise 11Shaira Jean SollanoNo ratings yet
- Anatomy of The Pharynx: Dr. Oscar Djauhari, Sp. THT-KLDocument18 pagesAnatomy of The Pharynx: Dr. Oscar Djauhari, Sp. THT-KLrizkauliaherNo ratings yet
- Nasopharynx SB AnatomyDocument6 pagesNasopharynx SB AnatomykyawzwarmgNo ratings yet
- Silverman 1971Document19 pagesSilverman 1971Krupali JainNo ratings yet
- Airway Management in The Adult - Miller's Anesthesia 2009Document38 pagesAirway Management in The Adult - Miller's Anesthesia 2009UrgenciasCol FoamNo ratings yet
- Mastication and Swallowing L4Document28 pagesMastication and Swallowing L4Siphelele MkhatshwaNo ratings yet
- Benumof Anatomia Via AereaDocument11 pagesBenumof Anatomia Via AereaMaria RicardoNo ratings yet
- Chapter 10 - Respiratory System - 2020 - The Zebrafish in Biomedical ResearchDocument5 pagesChapter 10 - Respiratory System - 2020 - The Zebrafish in Biomedical ResearchNicolas BaronNo ratings yet
- Human Digestive System, The System Used in TheDocument10 pagesHuman Digestive System, The System Used in Theعلي رسن رداد حمد ANo ratings yet
- Chapter 13 Surgical Managment of Salivary Gland DiseaseDocument35 pagesChapter 13 Surgical Managment of Salivary Gland DiseaseMohammed Qasim Al-WataryNo ratings yet
- Management of The Patient With Laryngitis: James Paul Dworkin P D& Robert J. Stachler MDDocument40 pagesManagement of The Patient With Laryngitis: James Paul Dworkin P D& Robert J. Stachler MDoneagustinNo ratings yet
- Fig. 1 - The Esophagus (Front and Right)Document23 pagesFig. 1 - The Esophagus (Front and Right)Ella JonesNo ratings yet
- 3 PharyngologyDocument86 pages3 PharyngologyWai Kwong Chiu100% (1)
- An Overview of Presbyphagia: Tinjauan PustakaDocument8 pagesAn Overview of Presbyphagia: Tinjauan PustakaMuhammad FarhanNo ratings yet
- Piazza 2010Document11 pagesPiazza 2010Israel BlancoNo ratings yet
- CHSJ 40 3 200Document5 pagesCHSJ 40 3 200Idelia GunawanNo ratings yet
- Twin BlockDocument5 pagesTwin BlockIdelia GunawanNo ratings yet
- Prevalensi MalocclusionDocument5 pagesPrevalensi MalocclusionIdelia GunawanNo ratings yet
- Down SyndromeDocument3 pagesDown SyndromeIdelia GunawanNo ratings yet
- Pressure Switch MDR5Document4 pagesPressure Switch MDR5Fidelis NdanoNo ratings yet
- Solar MPPT PresentationDocument21 pagesSolar MPPT PresentationPravat SatpathyNo ratings yet
- Uses of RefractoryDocument20 pagesUses of RefractoryRicha Tripathi100% (2)
- Training Report of IoclDocument68 pagesTraining Report of IoclAnupam SrivastavNo ratings yet
- Interviw With Martin DavisDocument12 pagesInterviw With Martin DavisraktimddkNo ratings yet
- Smart Dallas RoadmapDocument45 pagesSmart Dallas RoadmapAshish MohanNo ratings yet
- 415V CALCULATING SHEET AND SETTING LIST FOR EQUIPMENT PROTECTION OF CHP WAGON TIPPER AND ESP (Supplement For Zero Sequence Current Relay)Document25 pages415V CALCULATING SHEET AND SETTING LIST FOR EQUIPMENT PROTECTION OF CHP WAGON TIPPER AND ESP (Supplement For Zero Sequence Current Relay)Amaresh NayakNo ratings yet
- The Stall Chart - Varying Flow Secondary - Constant Inlet Temperature - Constant Outlet TemperatureDocument8 pagesThe Stall Chart - Varying Flow Secondary - Constant Inlet Temperature - Constant Outlet TemperatureSandra FerrellNo ratings yet
- Neptune Planet Experiment, Ariny Amos (Astronomer) - 1Document1,139 pagesNeptune Planet Experiment, Ariny Amos (Astronomer) - 1Dr. Amos ArinyNo ratings yet
- Appendix 11 Design FMEA ChecklistDocument16 pagesAppendix 11 Design FMEA ChecklistDearRed FrankNo ratings yet
- MCO 3 (30/3-3/4/2020) Reinforcement Chapter 2 Part A: Objective QuestionsDocument5 pagesMCO 3 (30/3-3/4/2020) Reinforcement Chapter 2 Part A: Objective QuestionsZalini AbdullahNo ratings yet
- Unit 2 Psychophysics: Threshold, Signal Detection Theory: StructureDocument10 pagesUnit 2 Psychophysics: Threshold, Signal Detection Theory: StructuresanoopsrajNo ratings yet
- Extreme Cold Weather (ECW) ClothingDocument7 pagesExtreme Cold Weather (ECW) ClothingSnowshadowNo ratings yet
- Chapter 4 - Structural Imperfections Kingery Introducción A Los Materiales CerámicosDocument27 pagesChapter 4 - Structural Imperfections Kingery Introducción A Los Materiales CerámicosLaura BárbaroNo ratings yet
- Conduit Trunking Capacity Chart RM TechnicalDocument1 pageConduit Trunking Capacity Chart RM TechnicalPrabir BhowmikNo ratings yet
- CL 55-60 AnDocument14 pagesCL 55-60 AnFrida KahloNo ratings yet
- 2017 District Superintendent ReportDocument12 pages2017 District Superintendent ReportRob Steinbrook100% (1)
- Initial Newborn AssessmentDocument14 pagesInitial Newborn Assessmentaclark831No ratings yet
- Fashion Through The Decades PowerpointDocument11 pagesFashion Through The Decades PowerpointNigar khanNo ratings yet
- Mesología BERQUEDocument6 pagesMesología BERQUEPanchita PonisioNo ratings yet
- Research Report - Aakanksha MistryDocument19 pagesResearch Report - Aakanksha MistryAakanksha MistryNo ratings yet
- 2015 - Soil Mechanics II - Final - enDocument7 pages2015 - Soil Mechanics II - Final - enjohn cambixNo ratings yet
- Accepted Manuscript: Diabetes & Metabolic Syndrome: Clinical Research & ReviewsDocument43 pagesAccepted Manuscript: Diabetes & Metabolic Syndrome: Clinical Research & ReviewsYanet FrancoNo ratings yet
- How To Start A Candle BusinessDocument49 pagesHow To Start A Candle BusinessJessica Rodrigo100% (1)
- Logg 4000Document7 pagesLogg 4000Stjepan FrljicNo ratings yet
- Tax Invoice/Bill of Supply/Cash Memo: (Original For Recipient)Document1 pageTax Invoice/Bill of Supply/Cash Memo: (Original For Recipient)Ch PrasadNo ratings yet
- Huawei FusionSolar Smart PV SolutionDocument32 pagesHuawei FusionSolar Smart PV SolutionJOGmzNo ratings yet
- Capacity PlanDocument1 pageCapacity PlanbishnuNo ratings yet
- Biology Q & A Booklet: (English Medium)Document76 pagesBiology Q & A Booklet: (English Medium)La EscenaNo ratings yet