Download as pdf or txt
You might also like
- Nremt Skills SheetsDocument19 pagesNremt Skills Sheetsakinda bevann SpencerNo ratings yet
- Ibogaine Treatment Manual - by Howard Lotsof and Boaz WachtelDocument35 pagesIbogaine Treatment Manual - by Howard Lotsof and Boaz Wachtelboaz_wachtel100% (3)
- Case Novo Nordisk PDFDocument43 pagesCase Novo Nordisk PDFArnab AzadNo ratings yet
- Mds Orthodontics: Final Exam Question BankDocument39 pagesMds Orthodontics: Final Exam Question Bankdrzana78No ratings yet
- Prioritization of Nursing ProblemsDocument1 pagePrioritization of Nursing ProblemsAbigail Lonogan100% (2)
- Chapter 13 Quiz For Health Psychology 328 McgillDocument3 pagesChapter 13 Quiz For Health Psychology 328 McgillOlivia CoutoNo ratings yet
- Atkins DietDocument10 pagesAtkins Dietfenny100% (1)
- AmebiasisDocument40 pagesAmebiasisAhlam AliNo ratings yet
- AmebiasisDocument23 pagesAmebiasisFaraxmahadNo ratings yet
- AmebiasisDocument23 pagesAmebiasisPriskila JesicaNo ratings yet
- Parasitology: Entamoeba HistolyticaDocument9 pagesParasitology: Entamoeba Histolyticaعلي حسين عودة العلياويNo ratings yet
- Topic 3 - Intestinal and Urogenital ProtozoaDocument76 pagesTopic 3 - Intestinal and Urogenital Protozoamostafadiab074No ratings yet
- Amoebiasis 150919181910 Lva1 App6892 PDFDocument40 pagesAmoebiasis 150919181910 Lva1 App6892 PDFMayank AhirwarNo ratings yet
- GI Protozoal & Infections Caused by HelminthsDocument39 pagesGI Protozoal & Infections Caused by HelminthsSHIHAB UDDIN KAZINo ratings yet
- Lesson 3 Amoebiasis: Entamoeba HistolyticaDocument7 pagesLesson 3 Amoebiasis: Entamoeba HistolyticaAstrid FausziaNo ratings yet
- Thypoid - RPUDocument22 pagesThypoid - RPUERONADIAULFAH SUGITONo ratings yet
- Amebiasis or Amoebic Dysentery Is A Parasitic Intestinal Infection Caused by Any of The Amoebas of The Entamoeba GroupDocument8 pagesAmebiasis or Amoebic Dysentery Is A Parasitic Intestinal Infection Caused by Any of The Amoebas of The Entamoeba GroupibrahimNo ratings yet
- Zoo143 Clinical Parasitology Topic: Parasites of Clinical SignificanceDocument13 pagesZoo143 Clinical Parasitology Topic: Parasites of Clinical SignificanceChristian Martell LiwagNo ratings yet
- Amebiasis Ana GiardiasisDocument11 pagesAmebiasis Ana Giardiasisosamafoud7710No ratings yet
- The Ameba ReportingDocument49 pagesThe Ameba ReportingALLISON PAMITTANNo ratings yet
- Dipiro 8 ParasitDocument12 pagesDipiro 8 ParasitErik Firman RusdiantoNo ratings yet
- Giardia Lamblia: The CystDocument30 pagesGiardia Lamblia: The CysterinastevianaNo ratings yet
- Amaebic Dysentery by Alishba-1Document7 pagesAmaebic Dysentery by Alishba-1Sharif SonaNo ratings yet
- Lecture Parasites in Immunocompromised PatientDocument50 pagesLecture Parasites in Immunocompromised PatientalgutNo ratings yet
- Lec 39. Parasitol Protozoa of SI, Protozoa, Nematodes LIDocument51 pagesLec 39. Parasitol Protozoa of SI, Protozoa, Nematodes LIkareemosama9916No ratings yet
- Amoebiasis ..ParasitologyDocument7 pagesAmoebiasis ..ParasitologyBenard NyaumaNo ratings yet
- Kuliah Cestode & Trematode (Hand-Out)Document13 pagesKuliah Cestode & Trematode (Hand-Out)made yogaNo ratings yet
- Tropical Infections and InfestationsDocument53 pagesTropical Infections and Infestationssamiksha meshramNo ratings yet
- Amaebiasis / Manyoka Aneraza / IsiqathoDocument138 pagesAmaebiasis / Manyoka Aneraza / Isiqatholex tecNo ratings yet
- Amebiasis and Giardiasis-FinalDocument25 pagesAmebiasis and Giardiasis-FinalDaniel AtiehNo ratings yet
- AMOEBIASISDocument4 pagesAMOEBIASISBryan MasikaNo ratings yet
- Disease Caused by Protozoa: GiardiasisDocument8 pagesDisease Caused by Protozoa: GiardiasisMudit MisraNo ratings yet
- GastroDocument77 pagesGastroMarielle RamosNo ratings yet
- Prevention and Control of Amoebic DysenteryDocument16 pagesPrevention and Control of Amoebic DysenteryPakSci MissionNo ratings yet
- ProtozoologiaDocument67 pagesProtozoologiaaaraujoj8861No ratings yet
- Diarrhea in Kittens and Young Cats - WSAVA2011 - VINDocument4 pagesDiarrhea in Kittens and Young Cats - WSAVA2011 - VINkukuhamru19No ratings yet
- 04 Lec - Giardiasis & TrichmoniasisDocument25 pages04 Lec - Giardiasis & Trichmoniasisمصطفي خندقاويNo ratings yet
- Medical Parasitology: HNS 212: Introduction To Medical ProtozoologyDocument132 pagesMedical Parasitology: HNS 212: Introduction To Medical ProtozoologyJOSEPH NDERITUNo ratings yet
- Neutrophils: GastritisDocument16 pagesNeutrophils: GastritisUuhhNo ratings yet
- Para2021-3 2Document29 pagesPara2021-3 2Koko HashamNo ratings yet
- Infectious DiseaseDocument200 pagesInfectious DiseaseSyed Faayez KaziNo ratings yet
- A Me Bias IsDocument5 pagesA Me Bias IsRavinder NainawatNo ratings yet
- Part-2-ParasitologyDocument33 pagesPart-2-ParasitologyAli AhmedNo ratings yet
- A Case Study On AmeobiasisDocument34 pagesA Case Study On AmeobiasisKhemz Dalde LimNo ratings yet
- Project 101Document70 pagesProject 101Joanne Bernadette AguilarNo ratings yet
- Common Intestinal ParasitesDocument16 pagesCommon Intestinal ParasitesbaliuwNo ratings yet
- Epidemiology of Infectious Disease Amebiasis: University of Fallujah College of Medicine Community MedicineDocument7 pagesEpidemiology of Infectious Disease Amebiasis: University of Fallujah College of Medicine Community MedicineMohamed HamoodNo ratings yet
- Balantidium Coli: Compiled by PB Wadigamangawa School of MLT, PeradeniyaDocument45 pagesBalantidium Coli: Compiled by PB Wadigamangawa School of MLT, Peradeniyawadige4668No ratings yet
- Classification of Human ParasitesDocument45 pagesClassification of Human ParasitesApple Jenn TempladoNo ratings yet
- Git T13 2024Document17 pagesGit T13 2024myarjddbzNo ratings yet
- Entamoeba HistolyticaDocument16 pagesEntamoeba Histolyticaشموخي عزتيNo ratings yet
- 17 FfsfafDocument78 pages17 FfsfafAndres Zambrano ArteagaNo ratings yet
- Microbiology 1Document57 pagesMicrobiology 1Kyla RamonesNo ratings yet
- RP RPDocument6 pagesRP RPEliezah RodriguezNo ratings yet
- Systemic Infections From GiDocument10 pagesSystemic Infections From GiJake MillerNo ratings yet
- Clinical Microbiology MrcsDocument17 pagesClinical Microbiology MrcsDeen MohammadNo ratings yet
- Protozoan Infections Part 2Document19 pagesProtozoan Infections Part 2Medicine SWUNo ratings yet
- Skenario 2 GastroDocument31 pagesSkenario 2 GastroChendy EndriansaNo ratings yet
- A Comphrensive Review On AmoebiasisDocument6 pagesA Comphrensive Review On AmoebiasisInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Flagellated Protozoan Parasite Giardiasis Epithelium Ventral Binary Fission Gastro-Intestinal Tract Lumen Trophozoites AnaerobesDocument6 pagesFlagellated Protozoan Parasite Giardiasis Epithelium Ventral Binary Fission Gastro-Intestinal Tract Lumen Trophozoites AnaerobesLavander MeggieNo ratings yet
- Lab-Ameb Comparisons 6-10-08Document71 pagesLab-Ameb Comparisons 6-10-08JOSEPH NDERITUNo ratings yet
- Gastroenteritis: Saima Alam AfridiDocument23 pagesGastroenteritis: Saima Alam AfridiMahnoor ParvezNo ratings yet
- Salmonella Infections: (Salmonelloses)Document56 pagesSalmonella Infections: (Salmonelloses)andualemNo ratings yet
- ProtozoaDocument28 pagesProtozoaephraimkquansahNo ratings yet
- Medical ProtozoologyDocument6 pagesMedical ProtozoologyRaymund MontoyaNo ratings yet
- Bronchial Asthma: Dr. Randula Samarasinghe Consultant PhysicianDocument32 pagesBronchial Asthma: Dr. Randula Samarasinghe Consultant PhysiciansivaNo ratings yet
- Chronic Obstructive Pulmonary DiseaseDocument29 pagesChronic Obstructive Pulmonary DiseasesivaNo ratings yet
- Bronchiactasis: Dr. Randula SamarasingheDocument12 pagesBronchiactasis: Dr. Randula SamarasinghesivaNo ratings yet
- Pneumonia: by DR Randula Samarasinghe Consultant PhysicianDocument34 pagesPneumonia: by DR Randula Samarasinghe Consultant PhysiciansivaNo ratings yet
- Anaemia in PregnancyDocument76 pagesAnaemia in PregnancysivaNo ratings yet
- Primary Amenorrhoea 2Document42 pagesPrimary Amenorrhoea 2sivaNo ratings yet
- Urinary Tract Infection in ChildrenDocument38 pagesUrinary Tract Infection in ChildrensivaNo ratings yet
- Taking A Paediatric History and ExaminationDocument57 pagesTaking A Paediatric History and ExaminationsivaNo ratings yet
- DVT ProphylaxisDocument30 pagesDVT ProphylaxissivaNo ratings yet
- Trichomnas Vaginalis 4. Toxoplasma Gondii: Tutorial 6/ Practical 6Document1 pageTrichomnas Vaginalis 4. Toxoplasma Gondii: Tutorial 6/ Practical 6sivaNo ratings yet
- Therapeutics - Tianjin - Lecture Contents - 3Document4 pagesTherapeutics - Tianjin - Lecture Contents - 3sivaNo ratings yet
- Tutorial Q S On Hepatitis VirusesDocument1 pageTutorial Q S On Hepatitis VirusessivaNo ratings yet
- Tutorial Q S On Herpes VirusesDocument2 pagesTutorial Q S On Herpes VirusessivaNo ratings yet
- Tutorial Questions ON HIV: Reference: Handout On Management of HCW Potentially Exposed To HBV, HCV or HivDocument1 pageTutorial Questions ON HIV: Reference: Handout On Management of HCW Potentially Exposed To HBV, HCV or HivsivaNo ratings yet
- International Sports Science Conference 2014Document99 pagesInternational Sports Science Conference 2014talktoyeshaNo ratings yet
- Cocaine PresentationDocument20 pagesCocaine Presentationapi-315185726No ratings yet
- Platelet Rich Plasma in OrthopaedicsDocument269 pagesPlatelet Rich Plasma in OrthopaedicsBelinda Azhari SiswantoNo ratings yet
- How Augmented Reality Helps in Improving Healthcare Sector: Blackwell, M, F MorganDocument47 pagesHow Augmented Reality Helps in Improving Healthcare Sector: Blackwell, M, F MorganAhmer SaeedNo ratings yet
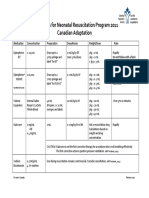
- Medications For Neonatal Resuscitation Program 2011 Canadian AdaptationDocument1 pageMedications For Neonatal Resuscitation Program 2011 Canadian AdaptationrubymayNo ratings yet
- Tools GAS Practical GuideDocument14 pagesTools GAS Practical GuideclaraNo ratings yet
- "How Does Art Therapy Affect The StudentsDocument63 pages"How Does Art Therapy Affect The StudentsMiguel VienesNo ratings yet
- The Standards of Psychiatric NursingDocument51 pagesThe Standards of Psychiatric NursingBonnie Bennet100% (2)
- Burns - Lewis Flashcards - QuizletDocument31 pagesBurns - Lewis Flashcards - QuizletNursyNurseNo ratings yet
- Workinstruction COMFOURDocument60 pagesWorkinstruction COMFOURsimbia88No ratings yet
- Livro - Acido LáticoDocument670 pagesLivro - Acido LáticoLuciana CoelhoNo ratings yet
- Encyclopedia of Folk Medicine: Old World and New World TraditionsDocument4 pagesEncyclopedia of Folk Medicine: Old World and New World TraditionsDrflora Eg100% (1)
- Vital Pulp Therapy 1Document6 pagesVital Pulp Therapy 1Mostafa Afifi Ali100% (1)
- Unit 2 Final DraftDocument2 pagesUnit 2 Final Draftapi-252269185No ratings yet
- Atm 04 08 160Document9 pagesAtm 04 08 160manalNo ratings yet
- Counselling Psychology Thesis ExamplesDocument6 pagesCounselling Psychology Thesis Exampleskimberlythomasarlington100% (1)
- Types of CPRDocument12 pagesTypes of CPRSaid OmaryNo ratings yet
- West Bengal Clinical Establishments (Registration and Regulation) Act, 2010Document27 pagesWest Bengal Clinical Establishments (Registration and Regulation) Act, 2010Latest Laws TeamNo ratings yet
- Milk AdulterationDocument2 pagesMilk AdulterationAbubakker SiddiqNo ratings yet
- A Blatner A Historical Chronology of Group Psychotherapy and PsychodramaDocument6 pagesA Blatner A Historical Chronology of Group Psychotherapy and PsychodramastellasplendersNo ratings yet
- Age Greater Than 60 Y/o Hereditary Precipitating Factors: Hypertension Increase Protein and Fat IntakeDocument3 pagesAge Greater Than 60 Y/o Hereditary Precipitating Factors: Hypertension Increase Protein and Fat Intakenursing concept mapsNo ratings yet
- ESICDocument23 pagesESICHarini Saripella100% (1)
- Management of Neonatal Hypothermia 3.0 PDFDocument14 pagesManagement of Neonatal Hypothermia 3.0 PDFNajwa binti MohdNo ratings yet