Download as pdf or txt
You might also like
- Renaissance Woman: Fat Loss, Muscle Growth & Performance Through Scientific EatingDocument20 pagesRenaissance Woman: Fat Loss, Muscle Growth & Performance Through Scientific EatingBenedict Ray Andhika33% (3)
- Buerger DiseaseDocument3 pagesBuerger DiseaseElmer DizonNo ratings yet
- Pat 2 Medsurg1Document20 pagesPat 2 Medsurg1api-300849832No ratings yet
- The Civil War - The Universe of War (Episode 5)Document5 pagesThe Civil War - The Universe of War (Episode 5)ShreyaNo ratings yet
- Bullying, Stalking and ExtortionDocument17 pagesBullying, Stalking and ExtortionJLafge83% (6)
- Venous Thromboembolism (VTE) - McMaster Pathophysiology ReviewDocument9 pagesVenous Thromboembolism (VTE) - McMaster Pathophysiology ReviewFadiyah UlfahNo ratings yet
- Cyclic Vomiting SyndromeDocument17 pagesCyclic Vomiting Syndromeminerva_stanciuNo ratings yet
- Description: Kawasaki Disease (Mucocutaneous Lymph Node Syndrome) Is A Form of VasculitisDocument4 pagesDescription: Kawasaki Disease (Mucocutaneous Lymph Node Syndrome) Is A Form of VasculitishamporkNo ratings yet
- PurpuraDocument7 pagesPurpuraMarie Joe AbainzaNo ratings yet
- Bartter SyndromeDocument3 pagesBartter SyndromeEnny Andriani100% (1)
- Case Study For Chronic Renal FailureDocument6 pagesCase Study For Chronic Renal FailureGabbii CincoNo ratings yet
- Chronic Obstructive Pulmonary Disease (COPD) and Bronchial AsthmaDocument16 pagesChronic Obstructive Pulmonary Disease (COPD) and Bronchial AsthmaAngel Joy CatalanNo ratings yet
- Idiopathic Thrombocytopenic Purpura: Overview With Report of A CaseDocument4 pagesIdiopathic Thrombocytopenic Purpura: Overview With Report of A CaseHernan GonzalezNo ratings yet
- Patent Ductus ArteriosusDocument3 pagesPatent Ductus ArteriosusMika SaldañaNo ratings yet
- Ventricular Septal DefectDocument18 pagesVentricular Septal DefectJessa Marie AgnesNo ratings yet
- GastroenteritisDocument24 pagesGastroenteritisMomogi ForeverhappyNo ratings yet
- Pott's Disease PDFDocument14 pagesPott's Disease PDFRaja RajanNo ratings yet
- BotulismDocument6 pagesBotulismAmir ShafiqNo ratings yet
- Kawasaki Disease LectureDocument25 pagesKawasaki Disease LectureAlif ZainalNo ratings yet
- Pregnancy HypertensionDocument30 pagesPregnancy HypertensionJon Gab PaquitNo ratings yet
- Acute Pyelonephritis Nursing Care PlansDocument2 pagesAcute Pyelonephritis Nursing Care PlansJoannah Marie Juloya Kiat-ong100% (1)
- 1 Fluid Volume Excess Chronic Renal Failure Nursing Care PlansDocument3 pages1 Fluid Volume Excess Chronic Renal Failure Nursing Care PlansMichael Baylon DueñasNo ratings yet
- Discharge Plan EndoDocument3 pagesDischarge Plan EndoCharlayne AnneNo ratings yet
- Chronic PyelonephritisDocument5 pagesChronic PyelonephritisIsak ShatikaNo ratings yet
- What Is The Difference Between A Pterygium and A Pinguecula?Document2 pagesWhat Is The Difference Between A Pterygium and A Pinguecula?Rizky AgustriaNo ratings yet
- Case Study 2Document4 pagesCase Study 2api-2451636590% (1)
- GastroenteritisDocument3 pagesGastroenteritisNicoleNo ratings yet
- Juvenile Idiopathic Arthritis GuidlineDocument11 pagesJuvenile Idiopathic Arthritis GuidlineAya Soraya100% (1)
- Hemolytic Uremic SyndromeDocument1 pageHemolytic Uremic SyndromeAndrea TeranNo ratings yet
- Chronic Kidney Disease (CKD) : Diabetes High Blood Pressure Responsible For Up To Two-Thirds GlomerulonephritisDocument6 pagesChronic Kidney Disease (CKD) : Diabetes High Blood Pressure Responsible For Up To Two-Thirds GlomerulonephritisKyle Ü D. CunanersNo ratings yet
- Zoledronic AcidDocument7 pagesZoledronic AcidbabiNo ratings yet
- Reye SyndromeDocument10 pagesReye SyndromeDanil KhairulNo ratings yet
- Tetanus - AnatomyDocument7 pagesTetanus - AnatomyJoro27No ratings yet
- GoutDocument26 pagesGoutRifki AlfikriNo ratings yet
- Hanta Vi Ru S Inf Ection SDocument20 pagesHanta Vi Ru S Inf Ection Stummalapalli venkateswara rao100% (3)
- Hipotensi PDFDocument6 pagesHipotensi PDFimahNo ratings yet
- ALL Pulmonary Leukostasis2Document6 pagesALL Pulmonary Leukostasis2Pratita Jati PermatasariNo ratings yet
- Av Fistula CreationDocument3 pagesAv Fistula CreationJianNo ratings yet
- Management of Patients With Intestinal and Rectal DisordersDocument33 pagesManagement of Patients With Intestinal and Rectal DisordersDoneva Lyn MedinaNo ratings yet
- Glomerulonephritis 10Document5 pagesGlomerulonephritis 10Eden Jay Calija AgoyNo ratings yet
- Lupus NephritisDocument15 pagesLupus NephritisVilza maharaniNo ratings yet
- Hyporeninemic HypoaldosteronismDocument12 pagesHyporeninemic HypoaldosteronismCésar Augusto Sánchez SolisNo ratings yet
- Alport SyndromeDocument7 pagesAlport SyndromeNTA UGC-NET100% (1)
- Blood Dyscrasia SDocument24 pagesBlood Dyscrasia SMasha FloreaNo ratings yet
- Pathophysiology of Portal HYPERTENSION PDFDocument11 pagesPathophysiology of Portal HYPERTENSION PDFCamilo VidalNo ratings yet
- Guada A. Dumapit RN, ManDocument18 pagesGuada A. Dumapit RN, ManAnne B. BuenvenidaNo ratings yet
- THROMBOPHLEBITISDocument50 pagesTHROMBOPHLEBITISmers puno100% (3)
- Acute GlomerulonephritisDocument14 pagesAcute GlomerulonephritisAnonymous D976HVjqcgNo ratings yet
- Pediatric Patent Ductus ArteriosusDocument12 pagesPediatric Patent Ductus Arteriosusabirami_murugesuNo ratings yet
- Mallory Weiss SyndromeDocument10 pagesMallory Weiss SyndromeGuilherme CaneverNo ratings yet
- Hiv in PregnancyDocument13 pagesHiv in Pregnancyapi-533578725No ratings yet
- Pamantasan NG Cabuyao College of Health Allied Sciences College of NursingDocument43 pagesPamantasan NG Cabuyao College of Health Allied Sciences College of NursingSofea MustaffaNo ratings yet
- AppendicitiesDocument58 pagesAppendicitiesGAURAV50% (2)
- Disturbances in The Pumping Mechanism of The HeartDocument1 pageDisturbances in The Pumping Mechanism of The HeartNicole Genevie MallariNo ratings yet
- BPHDocument81 pagesBPHFlo Neri BerondoNo ratings yet
- 10 1056@NEJMcpc1913468 PDFDocument10 pages10 1056@NEJMcpc1913468 PDFAbdelkader HociniNo ratings yet
- Carbetocin For The Prevention of Postpartum Hemorrhage A Systematic ReviewDocument7 pagesCarbetocin For The Prevention of Postpartum Hemorrhage A Systematic ReviewOscar Gregorio Coronado MacdanielNo ratings yet
- Gastric Outlet Obstruction, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandGastric Outlet Obstruction, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Cyanosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandCyanosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsRating: 5 out of 5 stars5/5 (1)
- Dengue TreamentDocument2 pagesDengue TreamentKevin ChanNo ratings yet
- Admission Criteria Dengue FeverDocument23 pagesAdmission Criteria Dengue FeverMuhammad Luthfi TaufikNo ratings yet
- Dengue Case Management Card 125085 12x6 Zcard DengueDocument2 pagesDengue Case Management Card 125085 12x6 Zcard DenguejmbobitNo ratings yet
- BLOOD AND BLOOD PPT PresentationDocument34 pagesBLOOD AND BLOOD PPT PresentationmarataningutukuNo ratings yet
- Iii Iihiiiiiiiiiiii 111111: Does User-Oriented Gas Turbine Research Pay Off?Document7 pagesIii Iihiiiiiiiiiiii 111111: Does User-Oriented Gas Turbine Research Pay Off?Morteza YazdizadehNo ratings yet
- GIS Based Analysis On Walkability of Commercial Streets at Continuing Growth Stages - EditedDocument11 pagesGIS Based Analysis On Walkability of Commercial Streets at Continuing Growth Stages - EditedemmanuelNo ratings yet
- SOPDocument3 pagesSOPShreya BonteNo ratings yet
- ECON7002: Unemployment and InflationDocument65 pagesECON7002: Unemployment and InflationNima MoaddeliNo ratings yet
- PDFDocument86 pagesPDFAnonymous GuMUWwGMNo ratings yet
- Intrnship Report On WapdaDocument106 pagesIntrnship Report On WapdaNarain MenghwarNo ratings yet
- Bac 1624 - ObeDocument4 pagesBac 1624 - ObeAmiee Laa PulokNo ratings yet
- Tunis Stock ExchangeDocument54 pagesTunis Stock ExchangeAnonymous AoDxR5Rp4JNo ratings yet
- 'Deus Caritas Est' - Pope Benedict and 'God Is Love'Document5 pages'Deus Caritas Est' - Pope Benedict and 'God Is Love'Kym JonesNo ratings yet
- Veterinary MicrobiologyDocument206 pagesVeterinary MicrobiologyHomosapienNo ratings yet
- Belgian Carrier PigeonDocument145 pagesBelgian Carrier PigeonstepathcNo ratings yet
- Dedication Certificate John Clyde D. Cristobal: This Certifies ThatDocument1 pageDedication Certificate John Clyde D. Cristobal: This Certifies ThatAGSAOAY JASON F.No ratings yet
- Sports Competence ResearchDocument11 pagesSports Competence ResearchHanna Relator DolorNo ratings yet
- The Quiescent Benefits and Drawbacks of Coffee IntakeDocument6 pagesThe Quiescent Benefits and Drawbacks of Coffee IntakeVikram Singh ChauhanNo ratings yet
- Furosemide DSDocument2 pagesFurosemide DSjhanrey0810_18768No ratings yet
- OutDocument318 pagesOutBet HalNo ratings yet
- Bilingualism Problems in NigeriaDocument9 pagesBilingualism Problems in NigeriaBasil OvuNo ratings yet
- Print - Udyam Registration CertificateDocument2 pagesPrint - Udyam Registration CertificatesahityaasthaNo ratings yet
- Desmand Whitson Resume 1PDFDocument2 pagesDesmand Whitson Resume 1PDFRed RaptureNo ratings yet
- Study Session8Document1 pageStudy Session8MOSESNo ratings yet
- Teacher Newsletter TemplateDocument1 pageTeacher Newsletter TemplateHart LJNo ratings yet
- Human Rights in IslamDocument22 pagesHuman Rights in IslamNoor AliNo ratings yet
- Chapter - 04 - Lecture Mod PDFDocument72 pagesChapter - 04 - Lecture Mod PDFtahirNo ratings yet
- Operational Framework of Community Organizing ProcessDocument18 pagesOperational Framework of Community Organizing ProcessJan Paul Salud LugtuNo ratings yet
- Palaycheck System Based Rice Cultivation in The PhilippinesDocument125 pagesPalaycheck System Based Rice Cultivation in The PhilippinesRizalito BenitoNo ratings yet
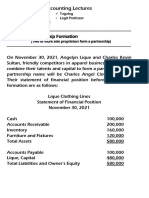
- 8 Lec 03 - Partnership Formation With BusinessDocument2 pages8 Lec 03 - Partnership Formation With BusinessNathalie GetinoNo ratings yet
- AUDCISE Unit 3 Worksheets Agner, Jam Althea ODocument3 pagesAUDCISE Unit 3 Worksheets Agner, Jam Althea OdfsdNo ratings yet