Download as pdf or txt
You might also like
- CDCS &CITF Mixed Paper - 2020Document8 pagesCDCS &CITF Mixed Paper - 2020Phương Anh100% (3)
- Cmgt400 v7 Wk2 Penetration Testing Plan TemplateDocument5 pagesCmgt400 v7 Wk2 Penetration Testing Plan TemplateVasyaNo ratings yet
- Analytics ExerciseDocument2 pagesAnalytics ExerciseritujaNo ratings yet
- The Big List of Star Wars NPC Names - RPG ReadyDocument5 pagesThe Big List of Star Wars NPC Names - RPG ReadyMichael LorenzNo ratings yet
- Health Analytics PWCDocument40 pagesHealth Analytics PWCsandeep_prasad17No ratings yet
- Administrative Healthcare Data: A Guide to Its Origin, Content, and Application Using SASFrom EverandAdministrative Healthcare Data: A Guide to Its Origin, Content, and Application Using SASRating: 4.5 out of 5 stars4.5/5 (2)
- Guidelines Conducting Stakeholder AnalysisDocument42 pagesGuidelines Conducting Stakeholder AnalysisDavid Sigalingging100% (1)
- Delay Defeats EquityDocument5 pagesDelay Defeats EquityMercy NamboNo ratings yet
- Comments On The Consultation Paper On Unified Health InterfaceDocument10 pagesComments On The Consultation Paper On Unified Health InterfacedirectthemailNo ratings yet
- Credentialing SpecialistDocument11 pagesCredentialing SpecialistMichael Variacion100% (1)
- Healthcare Cost and Utilization ProjectDocument10 pagesHealthcare Cost and Utilization Projectnoah676No ratings yet
- Guidance Device MDDSDocument9 pagesGuidance Device MDDSjerushaw.sinapiNo ratings yet
- HIMSS EHR Reporting Program RFI Comment LetterDocument9 pagesHIMSS EHR Reporting Program RFI Comment LetterSpit FireNo ratings yet
- Electronic Submissions: Federalregister - Gov/d/2023-03513, and On Govinfo - GovDocument8 pagesElectronic Submissions: Federalregister - Gov/d/2023-03513, and On Govinfo - GovAne DcNo ratings yet
- Medical Device Data Systems, Medical Image Storage Device, and Medical Image Communications Devices (MDDS)Document9 pagesMedical Device Data Systems, Medical Image Storage Device, and Medical Image Communications Devices (MDDS)Qi LiuNo ratings yet
- Design Considerations and Pre Market Submission Recommendations For Interoperable Medical Devices - Guidance For Industry and Food and Drug Administration StaffDocument21 pagesDesign Considerations and Pre Market Submission Recommendations For Interoperable Medical Devices - Guidance For Industry and Food and Drug Administration StaffQuality JiveNo ratings yet
- Paper To National Information Governance Board For Health and Social Care 22 September 2011 Paper ADocument8 pagesPaper To National Information Governance Board For Health and Social Care 22 September 2011 Paper AHelp Me InvestigateNo ratings yet
- 2014 Readiness Checklist FinalDocument30 pages2014 Readiness Checklist Final123_ebooksNo ratings yet
- Ford - Personal HealthDocument12 pagesFord - Personal HealthMaria Elisa Valentim Pickler NicolinoNo ratings yet
- BPHC HRSA-23-025 (H8H) FY 2023 Ending HIV Epidemic - FinalDocument44 pagesBPHC HRSA-23-025 (H8H) FY 2023 Ending HIV Epidemic - FinalTuhin DeyNo ratings yet
- Federalregister - Gov/d/2022-03227, and On Govinfo - GovDocument52 pagesFederalregister - Gov/d/2022-03227, and On Govinfo - GovDonald R. NelsonNo ratings yet
- Draft Guidance For Industry and Food and Drug Administration StaffDocument29 pagesDraft Guidance For Industry and Food and Drug Administration StaffStanleyChungNo ratings yet
- Medicare Fee-For-Service Provider Utilization & Payment Data Physician and Other Practitioners Dataset: A Methodological OverviewDocument9 pagesMedicare Fee-For-Service Provider Utilization & Payment Data Physician and Other Practitioners Dataset: A Methodological Overviewprerak shethNo ratings yet
- Resource Handout Medicaid Medical Record Documentation Resource HandoutDocument3 pagesResource Handout Medicaid Medical Record Documentation Resource HandoutRam KumarNo ratings yet
- Health and Human ServicesDocument57 pagesHealth and Human Servicesperry spiropoulosNo ratings yet
- Homeopathic Product Regulation: Evaluating The Food and Drug Administration's Regulatory Framework After A Quarter-Century Public HearingDocument7 pagesHomeopathic Product Regulation: Evaluating The Food and Drug Administration's Regulatory Framework After A Quarter-Century Public Hearingkazyhabib.dgdaNo ratings yet
- Data Knowledge ManagementDocument8 pagesData Knowledge Managementapi-488097590No ratings yet
- Capstone 2021 Paper Chi Nguyen FinaleditDocument19 pagesCapstone 2021 Paper Chi Nguyen Finaleditapi-487551161No ratings yet
- ED 2021 SCC 0093 0002 - Attachment - 1Document9 pagesED 2021 SCC 0093 0002 - Attachment - 1Atif JaveadNo ratings yet
- Hospital Compare Downloadable Database Data Dictionary: System Requirements SpecificationDocument88 pagesHospital Compare Downloadable Database Data Dictionary: System Requirements SpecificationMNo ratings yet
- Epi and Eval ResourcesDocument5 pagesEpi and Eval ResourceswaitNo ratings yet
- Billing Code: 4120-01-PDocument2,709 pagesBilling Code: 4120-01-PlaharkndNo ratings yet
- Nih Rfa 00183Document18 pagesNih Rfa 00183LiopNo ratings yet
- Manajemen Nyeri Dengan OpioidDocument4 pagesManajemen Nyeri Dengan Opioidscan resepNo ratings yet
- Manajemen Nyeri Dengan OpioidDocument4 pagesManajemen Nyeri Dengan Opioidscan resepNo ratings yet
- Guide To Colorado Grants, FY 2011Document83 pagesGuide To Colorado Grants, FY 2011ninmc20No ratings yet
- User Needs and Requirements Analysis For Big Data Healthcare ApplicationsDocument5 pagesUser Needs and Requirements Analysis For Big Data Healthcare Applicationsপ্রজ্ঞা লাবনীNo ratings yet
- Official Lecture#4 - Overview of Health InformaticsDocument3 pagesOfficial Lecture#4 - Overview of Health InformaticsLYKA ANTONETTE ABREGANANo ratings yet
- WHO - HMN HIS Tools To Support GFR10 - Template For Costing The HIS GapDocument202 pagesWHO - HMN HIS Tools To Support GFR10 - Template For Costing The HIS GapHarumNo ratings yet
- Nationwide DUADocument4 pagesNationwide DUAJohn SmithNo ratings yet
- HIMSS E-Health SIG White Paper: Access, Efficiency, Effectiveness, and Quality Improve The Health Status of PatientsDocument23 pagesHIMSS E-Health SIG White Paper: Access, Efficiency, Effectiveness, and Quality Improve The Health Status of PatientsSyed NasrullahNo ratings yet
- Hexa Research IncDocument5 pagesHexa Research Incapi-293819200100% (1)
- U.S. Food & Drug: Administration 10903 New Hampshire Avenue Silver Spring, MD 20993Document14 pagesU.S. Food & Drug: Administration 10903 New Hampshire Avenue Silver Spring, MD 20993bchunn2No ratings yet
- Alien TechnologyDocument11 pagesAlien TechnologySharvari TaklikarNo ratings yet
- EHRS BlueprintDocument390 pagesEHRS BlueprintJohanthan SputkaovNo ratings yet
- HL7 Meaningful Use - White PaperDocument5 pagesHL7 Meaningful Use - White Paperarijit00No ratings yet
- This Document Is Scheduled To Be Published in The Federal Register On 04/30/2014 and Available Online atDocument7 pagesThis Document Is Scheduled To Be Published in The Federal Register On 04/30/2014 and Available Online atpathanfor786No ratings yet
- Big Data Analytics in Healthcare - Promise and PotentialDocument10 pagesBig Data Analytics in Healthcare - Promise and PotentialMohd Otibi100% (1)
- PDF Cphims Review Guide Preparing For Success in Healthcare Information and Management Systems 3Rd Edition Healthcare Information and Management Systems Society Himss Ebook Full ChapterDocument54 pagesPDF Cphims Review Guide Preparing For Success in Healthcare Information and Management Systems 3Rd Edition Healthcare Information and Management Systems Society Himss Ebook Full Chapterjose.bailey983100% (3)
- 45978285dft 0 0Document14 pages45978285dft 0 0d unpredictibleNo ratings yet
- U.S. Food & Drug: Administration 10903 New Hampshire Avenue Silver Spring, MD 20993Document12 pagesU.S. Food & Drug: Administration 10903 New Hampshire Avenue Silver Spring, MD 20993bchunn2No ratings yet
- Briefing Memo HITECHDocument5 pagesBriefing Memo HITECHBrian AhierNo ratings yet
- The Open Data Platform - Improving Healthcare With AnalyticsDocument6 pagesThe Open Data Platform - Improving Healthcare With Analyticshuber.mcNo ratings yet
- NGA - RedactedDocument5 pagesNGA - Redactedanon_948979604No ratings yet
- HMISDocument18 pagesHMISFredrick IshengomaNo ratings yet
- Telehealth Information Sheet For Psychologists: Created by Jonathan Perle, PHD, Abpp - March 16, 2020Document5 pagesTelehealth Information Sheet For Psychologists: Created by Jonathan Perle, PHD, Abpp - March 16, 2020Clau Sali100% (2)
- Utah Clicks/Universal Application System - 2006 CSG Innovations Award WinnerDocument4 pagesUtah Clicks/Universal Application System - 2006 CSG Innovations Award Winnerbvoit1895No ratings yet
- Federal Register - Sunscreen Drug Products For Over-the-Counter Human UseDocument138 pagesFederal Register - Sunscreen Drug Products For Over-the-Counter Human UseOzan SubaşıNo ratings yet
- Discussion Topics - FDA Public Workshop - 2014may2 - OCC - FINALDocument2 pagesDiscussion Topics - FDA Public Workshop - 2014may2 - OCC - FINALscm implNo ratings yet
- 3h CompDocument4 pages3h CompCzara DyNo ratings yet
- HEDIS Paper 20220804 v3-1 PDFDocument14 pagesHEDIS Paper 20220804 v3-1 PDFsumits07No ratings yet
- MOU Template Final 2021Document2 pagesMOU Template Final 2021Rifqi RizaldiNo ratings yet
- 2009 UdsreportingmanualDocument108 pages2009 Udsreportingmanualrtfm216No ratings yet
- EBRD Technical and Financial Proposal FormsDocument9 pagesEBRD Technical and Financial Proposal Formsaspany loisNo ratings yet
- Grand Hyatt 3 SepDocument2 pagesGrand Hyatt 3 Seprehan rohanNo ratings yet
- North Tank Farm and Loading Arms Facilities (Pkg.4) Contract No: 6600029560 Petrofac Job No: JI-2018Document2 pagesNorth Tank Farm and Loading Arms Facilities (Pkg.4) Contract No: 6600029560 Petrofac Job No: JI-2018ratheeshNo ratings yet
- JawiDocument4 pagesJawiZoey GeeNo ratings yet
- Indian Capital Market: Current Scenario & Road Ahead: Prof Mahesh Kumar Amity Business SchoolDocument44 pagesIndian Capital Market: Current Scenario & Road Ahead: Prof Mahesh Kumar Amity Business SchoolasifanisNo ratings yet
- Final - Civil Service Code, Regulations and Rules - Administrative ManualDocument169 pagesFinal - Civil Service Code, Regulations and Rules - Administrative ManualSowdatu Abdullah-SandyNo ratings yet
- Part 2 - Basic Info On Polywaves and Structure LabelsDocument10 pagesPart 2 - Basic Info On Polywaves and Structure LabelsKing LeonidasNo ratings yet
- The Measurement of Income, Prices, and UnemploymentDocument18 pagesThe Measurement of Income, Prices, and UnemploymentEri BuwonoNo ratings yet
- Downtime and PM Order Integration With SAP PPDS - SAP BlogsDocument9 pagesDowntime and PM Order Integration With SAP PPDS - SAP BlogsVigneshNo ratings yet
- Bangladesh Telecommunication Industry-A Comprehensive Review 2019Document14 pagesBangladesh Telecommunication Industry-A Comprehensive Review 2019fullerineNo ratings yet
- Cases Crim Climaco To MejiaDocument9 pagesCases Crim Climaco To MejiaEd PadNo ratings yet
- Tacloban City: Licensure Examination For CIVIL ENGINEERSDocument5 pagesTacloban City: Licensure Examination For CIVIL ENGINEERSPhilBoardResultsNo ratings yet
- UT Daily Market Update 280911Document5 pagesUT Daily Market Update 280911jemliang_85No ratings yet
- Canlas vs. NapicoDocument4 pagesCanlas vs. NapicoTerry FordNo ratings yet
- Shi'i Sunni DivideDocument4 pagesShi'i Sunni DividealburoojNo ratings yet
- DM50-DM60 1Document2 pagesDM50-DM60 1RoxanaNo ratings yet
- Anatomy of A Market Bottom - CLSADocument21 pagesAnatomy of A Market Bottom - CLSASaeed JafferyNo ratings yet
- Legal Aspect of Nursing ProfessionDocument85 pagesLegal Aspect of Nursing ProfessionAnjo Pasiolco Canicosa50% (2)
- Letters of John and Abigail Adams Assignment 20132014Document8 pagesLetters of John and Abigail Adams Assignment 20132014api-235000986No ratings yet
- Fraud, Abuse, and Financial Conflicts of InterestDocument4 pagesFraud, Abuse, and Financial Conflicts of InterestKORA HamzathNo ratings yet
- St. Nicholas Day Student Version ColorDocument2 pagesSt. Nicholas Day Student Version ColorFilipkoNo ratings yet
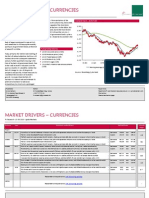
- Market Drivers - Currencies: Today's Comment Today's Chart - EUR/USDDocument5 pagesMarket Drivers - Currencies: Today's Comment Today's Chart - EUR/USDMiir ViirNo ratings yet
- Numericals RajputDocument3 pagesNumericals RajputantonoxfordNo ratings yet
- Appellant's BriefDocument13 pagesAppellant's BriefJojo Navarro100% (1)
- Fiscal PolicyDocument29 pagesFiscal Policyjay100% (1)