
Brief Screening Items To Identify Spanish-Speaking Adults With Limited Health Literacy and Numeracy Skills
Brief Screening Items To Identify Spanish-Speaking Adults With Limited Health Literacy and Numeracy Skills
You might also like
- Espanol medico y sociedad: Un libro para estudiantes de espanol en el tercer ano de estudios (Revised Edition)From EverandEspanol medico y sociedad: Un libro para estudiantes de espanol en el tercer ano de estudios (Revised Edition)No ratings yet
- Evidence-Based Public HealthDocument312 pagesEvidence-Based Public Healthnaravichandran3662100% (2)
- Music Assessment Rubric - Class Participation-2Document1 pageMusic Assessment Rubric - Class Participation-2api-299407251100% (2)
- AAFI Homeschooling Manual S.Y. 2022 - 2023Document27 pagesAAFI Homeschooling Manual S.Y. 2022 - 2023Tine Watts Azucena GalvezNo ratings yet
- Culture and Nonverbal Expressions of Empathy in Clinical Settings - A Systematic ReviewDocument49 pagesCulture and Nonverbal Expressions of Empathy in Clinical Settings - A Systematic ReviewAlberto JaramilloNo ratings yet
- The Inclusive Learning and Teaching HandbookDocument37 pagesThe Inclusive Learning and Teaching Handbookapi-194946381No ratings yet
- PEG Equity Framework Overview Rev 11 1Document4 pagesPEG Equity Framework Overview Rev 11 1APSEquityNo ratings yet
- ¡Necesito Un Medico!, But No One Speaks Spanish: A Look at Medical Interpretation PolicyDocument61 pages¡Necesito Un Medico!, But No One Speaks Spanish: A Look at Medical Interpretation PolicyGiulia SoligoNo ratings yet
- BarbarowiczDocument17 pagesBarbarowiczasriadiNo ratings yet
- Validation of Questionnaire On The Spiritual Needs Assessment For Patients (SNAP) Questionnaire in Brazilian PortugueseDocument10 pagesValidation of Questionnaire On The Spiritual Needs Assessment For Patients (SNAP) Questionnaire in Brazilian PortugueseGiovanna BertolinoNo ratings yet
- Assessing Medical Interpreters 重要 完Document21 pagesAssessing Medical Interpreters 重要 完NathanaëlNo ratings yet
- Research Paper Final DraftDocument19 pagesResearch Paper Final Draftapi-532628235No ratings yet
- Addressing Language and Culture Differences in Health Care Settings 2 PDFDocument4 pagesAddressing Language and Culture Differences in Health Care Settings 2 PDFWandi HuseinNo ratings yet
- Ireland Trip Final Paper - Language BarriersDocument12 pagesIreland Trip Final Paper - Language BarriersKelsi FarrenNo ratings yet
- Jurnal - 2Document15 pagesJurnal - 2ristytegarNo ratings yet
- Tutor - Critical AppraisalDocument8 pagesTutor - Critical AppraisalPriyanka TanwarNo ratings yet
- University of California PostprintsDocument37 pagesUniversity of California PostprintsPilar Galiano CruzNo ratings yet
- BMC Health Services Research: Digging Deeper: Quality of Patient-Provider Communication Across Hispanic SubgroupsDocument8 pagesBMC Health Services Research: Digging Deeper: Quality of Patient-Provider Communication Across Hispanic SubgroupsTitan LinggastiwiNo ratings yet
- Literature Review End of Life CareDocument4 pagesLiterature Review End of Life Caregpxmlevkg100% (1)
- Le N Et Al 2016 GerodontologyDocument9 pagesLe N Et Al 2016 GerodontologyBrijesh MaskeyNo ratings yet
- CFM Article 2014Document8 pagesCFM Article 2014Anjali SinglaNo ratings yet
- Connor Et Al. 2013 Functional Health Literacy in SwitzerlandDocument6 pagesConnor Et Al. 2013 Functional Health Literacy in SwitzerlandKitti SzpodnyiNo ratings yet
- Research Open AccessDocument14 pagesResearch Open AccessRob21aNo ratings yet
- 72.full - PDF ComDocument9 pages72.full - PDF ComNoNo ratings yet
- American Sign Language Interpreters Perceptions of Barriers To Healthcare Communication in Deaf and Hard of Hearing PatientsDocument6 pagesAmerican Sign Language Interpreters Perceptions of Barriers To Healthcare Communication in Deaf and Hard of Hearing Patientsapi-671390452No ratings yet
- Problem Solving and Diabetes Self-Management: Investigation in A Large, Multiracial SampleDocument5 pagesProblem Solving and Diabetes Self-Management: Investigation in A Large, Multiracial SampleAndreea MadalinaNo ratings yet
- Mathur Et Al 2016 GerodontologyDocument8 pagesMathur Et Al 2016 GerodontologyBrijesh MaskeyNo ratings yet
- Carson Kane Final Draft Project 2Document6 pagesCarson Kane Final Draft Project 2api-667077908No ratings yet
- A Review of Literature On Access To Primary Health CareDocument5 pagesA Review of Literature On Access To Primary Health CareafmzsbzbczhtbdNo ratings yet
- Mental Health Literature ReviewDocument5 pagesMental Health Literature Reviewfat1kifywel3100% (1)
- Culture Language and The Doctor Patient Relation Ship PDFDocument10 pagesCulture Language and The Doctor Patient Relation Ship PDFWagiono SuparanNo ratings yet
- Brazilian Version of A Lifestyle QuestionnaireDocument7 pagesBrazilian Version of A Lifestyle QuestionnaireAntônio de LimaNo ratings yet
- CrujjjjjDocument8 pagesCrujjjjjAlexander QuemadaNo ratings yet
- Development and Validation of A Functional Health Literacy Instrument in The PhilippinesDocument10 pagesDevelopment and Validation of A Functional Health Literacy Instrument in The PhilippinesIJPHSNo ratings yet
- Example of Public Health Literature ReviewDocument4 pagesExample of Public Health Literature Reviewc5qxzdj7100% (1)
- Nursing Interventions For Malnourished Children and Their Parents JournalDocument8 pagesNursing Interventions For Malnourished Children and Their Parents JournalroulyrosdianiNo ratings yet
- Literature Review of Palliative Care End of Life and DementiaDocument5 pagesLiterature Review of Palliative Care End of Life and DementialixdpuvkgNo ratings yet
- Hiv Aids Research Paper PDFDocument9 pagesHiv Aids Research Paper PDFcan3z5gx100% (1)
- Education Plays A Greater Role Than Age in Cognitive Test Performance Among Participants of The Brazilian Longitudinal Study of Adult Health (ELSA-Brasil)Document9 pagesEducation Plays A Greater Role Than Age in Cognitive Test Performance Among Participants of The Brazilian Longitudinal Study of Adult Health (ELSA-Brasil)Aishwarya PuttaNo ratings yet
- Komunikasi Dokter-PasienDocument7 pagesKomunikasi Dokter-PasienmeyfitaNo ratings yet
- Prolonged Noncoding RNA TDRKHAS1 Promotes Digestive Tract Most Cancers Cell Proliferation As Well As Intrusion Through The ?catenin Stimulated WNT Signaling Pathftgjm PDFDocument2 pagesProlonged Noncoding RNA TDRKHAS1 Promotes Digestive Tract Most Cancers Cell Proliferation As Well As Intrusion Through The ?catenin Stimulated WNT Signaling Pathftgjm PDFnewsmodem0No ratings yet
- Functional Assessment of Cancer Therapy-Brain Questionnaire: Translation and Linguistic Adaptation To Brazilian PortugueseDocument6 pagesFunctional Assessment of Cancer Therapy-Brain Questionnaire: Translation and Linguistic Adaptation To Brazilian PortugueserudolfpeterssonNo ratings yet
- Adulto MayorDocument13 pagesAdulto MayorFernanda MontalvoNo ratings yet
- Effective Health Communication: Guidance For EmployersDocument11 pagesEffective Health Communication: Guidance For EmployersvelwisherNo ratings yet
- The Danish Translation of The Medicines-Related Quality of Life (Mrqol) Scale From The Patient PerspectiveDocument15 pagesThe Danish Translation of The Medicines-Related Quality of Life (Mrqol) Scale From The Patient PerspectiveFACORI Farmacéuticos de Costa RicaNo ratings yet
- Hispanic Youth in Pregnancy Prevention Programs Research: An Analysis of The Research LiteratureDocument27 pagesHispanic Youth in Pregnancy Prevention Programs Research: An Analysis of The Research LiteratureUrbanYouthJusticeNo ratings yet
- Speros-Healthliteracyarticlejan 3448 PDFDocument8 pagesSperos-Healthliteracyarticlejan 3448 PDFSeptyadi David Eka Aryungga100% (1)
- Oral Health LiteracyDocument20 pagesOral Health Literacyapi-257281959No ratings yet
- The Impact of Perinatal HIV Infection On Older School-Aged Children's and Adolescents' Receptive Language and Word Recognition SkillsDocument9 pagesThe Impact of Perinatal HIV Infection On Older School-Aged Children's and Adolescents' Receptive Language and Word Recognition SkillsAndrew MoriartyNo ratings yet
- Health Literacy Among Older Adults A Systematic Literature ReviewDocument4 pagesHealth Literacy Among Older Adults A Systematic Literature ReviewcmaqqsrifNo ratings yet
- 2010 Article 1507Document7 pages2010 Article 1507Aisyah GirindraNo ratings yet
- Carson Kane EssayDocument8 pagesCarson Kane Essayapi-667077908No ratings yet
- Literature Review Example Mental HealthDocument4 pagesLiterature Review Example Mental Healthea6mkqw2100% (1)
- Stroke Article 1Document10 pagesStroke Article 1api-292843843No ratings yet
- Jced 11 E1143Document8 pagesJced 11 E1143rugeaelzwea2No ratings yet
- 2013 Development and Psychometric Testing of The Hemophilia Well-Being Index IJBM 20, 609-617Document9 pages2013 Development and Psychometric Testing of The Hemophilia Well-Being Index IJBM 20, 609-617Miguel OchoaNo ratings yet
- Chapter 2 Reviewsof Related Literatureand Related Studies TopicalDocument14 pagesChapter 2 Reviewsof Related Literatureand Related Studies Topicalr76914751No ratings yet
- Oral Care Literature ReviewDocument7 pagesOral Care Literature Reviewafmzfsqopfanlw100% (1)
- Public Health Dissertation ExamplesDocument4 pagesPublic Health Dissertation ExamplesWhereToBuyWritingPaperCanada100% (1)
- Of Health Literacy For Spanish-Speaking Adults en Chile, para MedirDocument7 pagesOf Health Literacy For Spanish-Speaking Adults en Chile, para MedirLuis Luengo MachucaNo ratings yet
- The Minnesota Living With Heart Failure QuestionnaDocument11 pagesThe Minnesota Living With Heart Failure Questionnamgarcía_62490No ratings yet
- Culture, Language, and The Doctor-Patient Relationship: Escholarship@UmmsDocument10 pagesCulture, Language, and The Doctor-Patient Relationship: Escholarship@UmmsBUAHIN JANNANo ratings yet
- Dissertation Clinical TrialsDocument5 pagesDissertation Clinical TrialsCanSomeoneWriteMyPaperForMeSingapore100% (1)
- Bob Marley - No Woman No CryDocument4 pagesBob Marley - No Woman No CryRob21aNo ratings yet
- Impacto Health Literacy Nos OutcomesDocument11 pagesImpacto Health Literacy Nos OutcomesRob21aNo ratings yet
- Boss Ve-20 ManualDocument144 pagesBoss Ve-20 ManualCarlo Mauricio González Parra100% (1)
- Public Health and Online Misinformation: Challenges and RecommendationsDocument19 pagesPublic Health and Online Misinformation: Challenges and RecommendationsRob21aNo ratings yet
- Research Open AccessDocument14 pagesResearch Open AccessRob21aNo ratings yet
- PSR-SX700: Category Style Name Category Style Name Category Style Name Category Style NameDocument2 pagesPSR-SX700: Category Style Name Category Style Name Category Style Name Category Style NameRob21aNo ratings yet
- Oral Health PromotionDocument29 pagesOral Health PromotionRob21aNo ratings yet
- Lit Review CS and Medical EducationDocument14 pagesLit Review CS and Medical EducationRob21aNo ratings yet
- Health Literacy ConcurrentDocument5 pagesHealth Literacy ConcurrentRob21aNo ratings yet
- International Journal of Nursing Studies: Tze-Fang Wang, Chiu-Mieh Huang, Chyuan Chou, Shu YuDocument7 pagesInternational Journal of Nursing Studies: Tze-Fang Wang, Chiu-Mieh Huang, Chyuan Chou, Shu YuRob21aNo ratings yet
- Self-Empowerment in Health PromotionDocument7 pagesSelf-Empowerment in Health PromotionRob21aNo ratings yet
- Wiley Milbank Memorial FundDocument22 pagesWiley Milbank Memorial FundRob21aNo ratings yet
- Level 3 Cost Accounting - SyllabusDocument17 pagesLevel 3 Cost Accounting - SyllabusChan Siew ChongNo ratings yet
- PE General Lesson Plan Template: Central FocusDocument7 pagesPE General Lesson Plan Template: Central Focusapi-396137633No ratings yet
- Self-Study Report Part-IiDocument21 pagesSelf-Study Report Part-IiSajja SrinivasNo ratings yet
- 2016 NCAE Orientation School LevelDocument28 pages2016 NCAE Orientation School LevelClaudette G. PolicarpioNo ratings yet
- Science Unit PlannerDocument13 pagesScience Unit Plannerapi-324855292No ratings yet
- Typhoon PARDocument5 pagesTyphoon PARreynaldo banaria jrNo ratings yet
- TT&SC Chapter2 M3.3 FlorendoDocument2 pagesTT&SC Chapter2 M3.3 FlorendoEfren Garcia FlorendoNo ratings yet
- A Review of Digital Literacy AssessmentDocument31 pagesA Review of Digital Literacy AssessmentDeasy IrawatiNo ratings yet
- Assignment 3 Syllabus BrowniDocument10 pagesAssignment 3 Syllabus Browniapi-258058489No ratings yet
- EntryPracRPNDocument20 pagesEntryPracRPNBiju ChackoNo ratings yet
- Writing Samples B2Document48 pagesWriting Samples B2nota32100% (4)
- Seatwork 2 BTVTED 2ADocument67 pagesSeatwork 2 BTVTED 2ACharlton Benedict BernabeNo ratings yet
- Task 4b Math Learning SegementsDocument2 pagesTask 4b Math Learning Segementsapi-283217268No ratings yet
- P1 - Professional Accountant Practice and RevisiDocument449 pagesP1 - Professional Accountant Practice and Revisiarmaan100% (2)
- Maryam Assignment 2Document22 pagesMaryam Assignment 2hammad asgharNo ratings yet
- Reflection 3 Life Cycle of A PumpkinDocument4 pagesReflection 3 Life Cycle of A Pumpkinapi-177768681No ratings yet
- APU-APIIT Ethics Approval Process - Introduction and GuidanceDocument7 pagesAPU-APIIT Ethics Approval Process - Introduction and GuidanceVernon LohNo ratings yet
- 2015 PSSA Item and Scoring Sampler Science Grade 8Document36 pages2015 PSSA Item and Scoring Sampler Science Grade 8Chase FloydNo ratings yet
- 12 SMAW W 1 - Types of Welding PositionsDocument10 pages12 SMAW W 1 - Types of Welding PositionsNelPalalonNo ratings yet
- IEEE Wireless Communication Engineering Technologies Certification Candidate's Handbook 2018Document53 pagesIEEE Wireless Communication Engineering Technologies Certification Candidate's Handbook 2018jeanneptuneNo ratings yet
- Annexure-147. (Ling - UG - Revised)Document33 pagesAnnexure-147. (Ling - UG - Revised)pranjal sharmaNo ratings yet
- Module in PBADocument3 pagesModule in PBAAcire NonacNo ratings yet
- Primary Election Unit PlanDocument4 pagesPrimary Election Unit Planapi-249957841No ratings yet
- MPU For Certificate (Level 3) : Summary of Information On Each ModuleDocument3 pagesMPU For Certificate (Level 3) : Summary of Information On Each ModuleWilliam AnthonyNo ratings yet
- Section FourDocument13 pagesSection Fourapi-532404528No ratings yet
- Pitch Lesson PlanDocument6 pagesPitch Lesson Planapi-318222702No ratings yet




































































































Singh et al.
BMC Health Services Research (2015) 15:374
DOI 10.1186/s12913-015-1046-2
RESEARCH ARTICLE
Open Access
Brief screening items to identify spanish-speaking
adults with limited health literacy and numeracy skills
Rashmi Singh1, Laura Scott Coyne2 and Lorraine S. Wallace3*
Abstract
Background: Limited health literacy (HL) and numeracy have been shown to be associated with a wide array of
poor health-related outcomes, knowledge, and behaviors. The purpose of this study was to evaluate the clinical
utility of brief HL and numeracy screening items in identifying Spanish-speaking adults HL and numeracy skills.
Methods: We studied convenience samples of native Spanish-speaking adults in Columbus, Ohio. A trained
research assistant administered sociodemographic items, HL and numeracy screening items, Short Assessment of
Health Literacy (SAHL), and Newest Vital Sign (NVS) to participants in Spanish.
Results: Participants (n = 151) averaged 36.8 11.0 years of age and 54.7 % were female. Average SAHL score was
15.7 2.8 (range = 4 to 18), while the average NVS score was 1.7 1.5 (range = 0 to 6). How confident are you
filling out medical forms by yourself? performed best in detecting limited NVS scores (AUROC = 0.66; 95 %
confidence interval [CI] = 0.570.75), limited/marginal NVS scores (AUROC = 0.75; 95 % CI = 0.650.84), and
inadequate SAHL scores (AUROC = 0.69; 95 % CI = 0.580.79).
Conclusion: A single HL screening item is useful for quickly estimating HL and numeracy skills in native
Spanish-speaking adults.
Keywords: Health literacy, Numeracy, Spanish-speaking, Validation studies
Background
Hispanics are one of the fastest-growing minority groups
in the United States, as well as a group considered to be
at particularly high risk for problems associated with low
health literacy (HL) and numeracy [1]. A growing body
of literature documents the strong association of limited
HL and numeracy with a wide array of poor healthrelated outcomes, knowledge, and behaviors [2]. Among
Spanish-speaking adults in the United States specifically,
those with limited HL and/or numeracy have shown to
have difficulty understanding and acting upon emergency department discharge instructions [3], are less
likely to adequately dose pediatric medications correctly
[4], are at increased risk of seeking care at emergency
departments and urgent care centers in response to their
childrens asthma exacerbations [5], and are less likely to
receive routine mammography [6].
* Correspondence: Lorraine.Wallace@osumc.edu
3
Department of Family Medicine, The Ohio State University, 2231 North High
Street, Columbus, OH 43210, USA
Full list of author information is available at the end of the article
While valid and reliable HL assessment tools such as
the Rapid Estimate of Adult Literacy in Medicine [7],
Test of Functional Health Literacy in Adults [8], Health
Literacy Skills Instrument [9], Health Literacy Assessment using Talking Touchscreen Technology (Health
LiTT) [10], and Health Literacy Management Tool
(HeLMS) [11] are available for predominantly research
purposes, time constraints often limited their use in busy
clinical settings. Recognizing that it is often difficult for
clinicians to identify patients at risk of limited HL based
the conversation exchange during clinical encounters
[1214], shorter HL assessment tools such as the Short
Assessment of Health Literacy (SAHL) [15], Newest
Vital Sign (NVS) [16], and Communicative, Functional,
Critical Health Literacy scales [17, 18] could, potentially,
be useful in busy clinical settings to gauge a patients HL
skills. The NVSwhich can be administered in less than
three minutes [19, 20]is perhaps one of the most feasible HL assessment tools for use in routine clinical
practice.
2015 Singh et al. Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0
International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and
reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to
the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver
(http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
Singh et al. BMC Health Services Research (2015) 15:374
Among English-speaking populations, studies have
revealed mixed results regarding whether patients feel
comfortable or not disclosing their limited HL to health
care providers [2124]. For instance, in studies were the
REALM [21, 23] and TOFHLA [22] were administered,
patients with limited HL reported a tremendous amount
of shame in sharing their results with their health care
providers. However, VanGeest and colleagues [24]
found that among those completing the NVS, nearly
all patientsregardless of NVS scorereported that
screening did not cause them to feel shameful and recommended HL screening in routine clinical practice.
Brief one sentence HL and numeracy screening items
have been developed and tested, against various formal HL
assessment tools, to quickly assess patients HL and numeracy skills in busy clinical settings [2528]. While brief HL
and numeracy screening items have shown promise in predicting English-speaking adults HL and numeracy abilities
[2528], less is known regarding the utility of equivalent
Spanish-language HL screening items. For instance, Sarkar
and colleagues found established HL screening items to be
effective in discriminating between those with adequate
versus inadequate/marginal HL, as measured by TOHLHA
(administered in both English and Spanish) scores, in samples of both English and Spanish speaking diabetes patients
aged 55 years in San Francisco, California [29]. Similarly,
Cordasco et al. [30] found an established HL screening item
(How confident are you filling out medical forms by yourself? [25]) and self-reported educational attainment of less
than 6 years to be predictive of S-(Spanish)TOFHLA scores
among elderly (65 years of age), monolingual diabetic
Spanish speakers residing in Los Angeles, California.
Since Spanish speakers tend to be at greater risk for
limited HL and numeracy [1], a need exists to further test
the predictive value of HL and numeracy screening items
across various, diverse populations throughout the United
States. To our knowledge, just two studies, conducted by
Sarkar et al. [29] and Cordasco et al. [30], have explored
use of HL screening items in predicting TOFHLA
scores among Spanish speakers. While both these studies
[29, 30] provide evidence as to the usefulness of HL
screening items among Spanish speakers, their study populations were limited to older (55 years of age) adults
with established chronic disease (type 2 diabetes) residing
in California. Therefore, to address gap in the literature,
the purpose of this study was to evaluate the utility of brief
HL and numeracy screening items in predicting NVS and
SAHL scores among a sample of Spanish-speaking adults
residing in a large, Midwestern city in the United States.
Methods
Study design and recruitment procedures
This study employed a cross-sectional design where a
convenience sample of subjects completed a structured
Page 2 of 7
one-on-one interview, in Spanish, with a trained, bilingual (fluent in both English and Spanish) research assistant (RA). During the summers of 2012 and 2013, a total
of 151 native Spanish-speaking adults from two community sites in Columbus, Ohio, United States participated
in this study. The first community site was a primary
care clinic that provided free of charge medical care to
Spanish speaking patients. The second community site
was a classroom setting where Spanish speaking adults
were offered English as-a-second language instruction.
In accordance to the Helsinki Declaration, The Ohio
State University Biomedical Institutional Review Board
approved all research and informed consent procedures
employed in this study.
Depending upon community site visited, a RA
approached potential study participants in either the
waiting area of the primary care clinic or a small
meeting room at the English as-a-second language facility. The RA explained the purpose of the study, informed the participant that his/her responses would
be anonymous, and that he/she would receive a $5
supermarket gift card for partaking in the study. To
be eligible to partake in the study, participants had
to be 18 years of age and speak Spanish as their
first (primary) language. Potential participants who
appeared acutely ill, had diminished decision-making
capacity, and/or had poor visual acuity were excluded.
Both RAs were medical students and made the determination as to whether a participant was well enough
to partake in the study. However, just one participant,
over the course of both summers, was deemed too
acutely ill to partake in the study. At all sites combined, approximately 86 % of adults approached to
partake in the study agreed to do so. The most commonly cited reason for refusing to participate in the
study was lack of interest.
Structured interview process and instrumentation
Those agreeing to participate in the study were taken to
a private area (i.e., empty clinical examination or classroom) to complete a 10 to 15 min one-on-one interview.
Upon receiving verbal consent from each participant,
the RA began the one-on-one structured interview in
Spanish. To begin the interview, the RA administered 5
sociodemographic items (sex, age, formal educational
attainment, and self-reported health status) from the
2010 Spanish-language version of the Center for Disease
Control and Preventions Behavioral Risk Factor Surveillance Survey [31].
Second, the RA administered 3 HL and 3 numeracy
screening items to each participant. The HL screening
items and response options were initially developed and
validated in English by Chew and colleagues [25] and
then translated into Spanish by Sarkar et al. [29]. As
Singh et al. BMC Health Services Research (2015) 15:374
shown in Table 1, we used the Spanish version of these
HL items and response options, in our study, that were
developed by Sarkar et al. [29]. The numeracy screening
items and response options developed by Woloshin et
al. [32] and Fagerlin et al. [33] were translated from
English to Spanish for our study. Specifically, the second
author and along with a native Spanish speaker collectively translated the numeracy items and corresponding
response options into Spanish.
Third, the RA administered the 18-item SAHL [15] to
each participant. The SAHL is a validated HL tool assessing Spanish-speaking adults ability to read and comprehend basic medical terms. Individual SAHL items are
presented to the interviewee in flashcard format. The
stem is printed at the top of the card in boldface while
two associated wordskey and distractorappear at
the bottom of the card. The participant is asked to
identify which word is associated with the stem word.
As an example, one card presented had the stem word
pregnancy [embarazo] with the two associated words
birth [parto] and childhood [niez]. Each participant
then had to distinguish whether birth or childhood was
more closely related to the stem word pregnancy. Per
established SAHL scoring guidelines, those scoring 14
were categorized as having inadequate HL.
To conclude the interview, the RA administered the
NVS to each participant. The, NVS, consisting of 6 questions, includes a combination of reading comprehension
Page 3 of 7
and manipulation of numerical data to interpret content
presented within an ice cream container nutrition label
[16]. The valid and reliable Spanish language version of
the NVS, including questions and the accompanying ice
cream nutrition label, were presented to participants. As
an example, one NVS question asks, If you eat all the ice
cream in the container, how many calories will you have
consumed,? [Si usted se come todo el helado en el envase,
cuntas caloras habr consumido?] requiring participants to locate nutritional information on the label and
apply basic math skills. Based on established NVS scoring
thresholds, participants were classified as having limited
(NVS = 01), marginal (NVS = 23), or adequate (NVS =
46) HL/numeracy skills. The NVS has been validated in
previous studies [3436].
Statistical analysis
Data were analyzed using the Statistical Package for the
Social Sciences (SPSS+ 20.0, Chicago, IL). A priori, statistical significance was set at p < 0.05. Descriptive statistics
(means, standard deviations, frequencies, percentages)
were conducted to depict sociodemographic and HL and
numeracy characteristics of the study sample.
Spearmans rank correlation coefficient was used to
estimate the relationship between NVS and SAHL
scores. Next, using both NVS and SAHL scores as reference
standards, we computed area under the ROC (AUROC)
curves for individual HL and numeracy screening items.
Table 1 English to spanish language translation of established health literacy and numeracy screening items and response options
English Language
Spanish Language
How often do you have problems learning about your medical condition
because of difficulty understanding written information?17
Qu tan seguido tiene problemas aprendiendo sobre su condicin
mdica porque es difcil entender informacin escrita?
Always Often Occasionally Sometimes Never
Siempre Con mucha frecuencia A veces De vez en cuando Nunca
How confident are you filling out medical forms by yourself? 17
Qu tan seguro(a) se siente al llenar formas usted solo(a)?
Extremely Quite a bit Somewhat A little bit Not at all
Completamente seguro(a) Bastante seguro(a) Algo seguro(a) Un poco
seguro(a) Para nada
How often do you have someone help you read hospital materials? 17
Qu tan seguido tiene usted, un familiar, un amigo, un empleado del
hospital o la clnica u otra persona que le ayude a leer materiales del
hospital?
Always Often Occasionally Sometimes Never
Siempre Con mucha frecuencia A veces De vez en cuando Nunca
In general, how easy or hard do you find it to understand medical
statistics?25
En general, qu tan fcil o difcil es para usted entender estadsticas
sobre temas mdicos?
Very easy Easy Hard Very hard
Muy fcil Fcil Difcil Muy difcil
How much do you agree or disagree with the following statement? In
general, I feel uncomfortable with health information that has a lot of
numbers and statistics.26
Cunto est usted de acuerdo o en desacuerdo con la siguiente
afirmacin? En general, no encuentro clara la informacin sobre salud
cuando tiene muchos nmeros y estadsticas.
Strongly agree Somewhat agree Somewhat disagree Strongly disagree
Totalmente de acuerdo Algo de acuerdo Algo en desacuerdo
Totalmente en desacuerdo
How much do you agree or disagree with the following statement? In
general, I depend on numbers and statistics to help me make decisions
about my health. 26
Cunto est usted de acuerdo o en desacuerdo con la siguiente
afirmacin? En general, me baso en nmeros y estadsticas para tomar
decisiones acerca del mi salud.
Strongly agree Somewhat agree Somewhat disagree Strongly disagree
Totalmente de acuerdo Algo de acuerdo Algo en desacuerdo
Totalmente en desacuerdo
Singh et al. BMC Health Services Research (2015) 15:374
Page 4 of 7
Table 2 Sociodemographic characteristics of study participants
(n = 151)
Sociodemographic
Characteristics
Mean Standard
Deviation or Frequency
Percent (%)
Age in Years
36.8 11.0
Male
69
45.7
Female
82
54.3
< High School
124
82.2
High School
27
17.8
26
17.2
Sex
Educational Attainment
Self-rated Health Status
Poor/Fair
Good
48
31.8
Very Good/Excellent
77
51.0
AUROCs allowed us to compare the predictive ability of
individual screening questions in estimating limited/
marginal NVS scores or inadequate SAHL scores. An ideal
question has an AUROC of 1.0, while an AUROC 0.5 indicates a screening item that provides no useful information.
Results
The overall sociodemographic characteristics of our
sample are described in Table 2. Distribution of SAHL
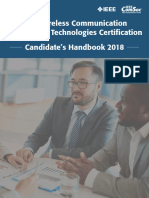
and NVS scores is presented in Figs. 1 and 2, respectively.
Overall, participants averaged 15.7 2.8 correct responses
on the SAHL with 22.4 % classified as having inadequate
HL (SAHL 14). Participants averaged 1.70 1.54 correct
NVS responses with the majority (60.5 %) classified as
having limited numeracy (NVS score = 0 or 1). Overall,
NVS and SAHL scores were weakly correlated with one
another (rho = 0.39; P < 0.01) [37].
AUROCs for individual HL and numeracy screening
items in identifying participants with limited/marginal
NVS scores and/or inadequate SAHL scores are shown
in Table 3. Across both reference standards, the HL
screening item, How confident are you filling out
medical forms by yourself?, performed best in detecting
limited NVS scores (AUROC = 0.75; 95 % CI = 0.650.84),
limited/marginal NVS scores (AUROC = 0.66; 95 % confidence interval [CI] = 0.570.75), and inadequate SAHL
scores (AUROC = 0.69; 95 % CI = 0.580.79). The numeracy screening item, In general, how easy or hard do you
find it to understand medical statistics,? was best in
detecting limited NVS scores (AUROC = 0.71; 95 % CI =
0.600.83) but only moderately well in detecting limited/
marginal NVS scores (AUROC = 0.61; 95 % CI = 0.51
0.70) and inadequate SAHL scores (AUROC = 0.59; 95 %
CI = 0.480.70). For the remaining HL and numeracy
screening items, AUROC scores ranged from 0.27
(How often do you have problems learning about your
medical condition because of difficulty understanding
written information?, in detecting limited numeracy) to
0.50 (How often do you have someone help you read
hospital materials, in detecting inadequate HL).
Discussion
This study examined utility of brief HL and numeracy
screening items in predicting NVS and SAHL scores
among a sample of Spanish-speaking adults residing
in a large, Midwestern city in the United States.
Overall, participants in this study had lower numeracy
as compared to general HL skills as measured by the
NVS and SAHL, respectfully. The most important
finding from our study was that two screening items
(How confident are you filling out forms by yourself? and In general, how easy or hard do you find
it to understand medical statistics?) were both strong
predictors of overall NVS and SAHL scores.
Fig. 1 Distribution of participants Short Assessment of Health Literacy (SAHL) scores across established scoring thresholds
Singh et al. BMC Health Services Research (2015) 15:374
Page 5 of 7
Fig. 2 Distribution of Participants Newest Vital Sign (NVS) scores across established scoring thresholds
Our findings extend the results of prior studies in
which the confident with forms item was the best predictor of identifying patients at risk of inadequate HL
[2530, 38]. In contrast to Sarkar et al. [29], who found
that all of Chews [25] screening items performed well in
Spanish speakers, the confident with forms item was a
much better predictor of NVS and SAHL scores in our
study population. However, our results mirror those of
Cordasco et al. [30], who found the confident with
forms item to be the best predictor of inadequate
TOFHLA scores in their population of monolingual
Spanish speakers in Los Angeles, California. The combined findings of our study and Sarkars, and Cordascos
studies provide strong evidence for the benefit of using a
single Spanish HL screening item to estimate a participants HL and/or numeracy skills.
In comparison to earlier studies in English-speaking
populations [2530, 38], Chews [25] brief HL screening
items had lower AUROCs among our Spanish-speaking
population. In part, this may be due to participants interpretation of the items as referring to forms and
materials written in English, not Spanish. Thus, participant responses may reflect difficulties in reading and
interpreting materials in English, rather than their ability
to read and respond to materials written in their native
language. Future work, could perhaps, specify that written material and forms refer to those in the participants
native (Spanish) language.
Unlike Sarkar et al. [29] and Cordasco et al. [30] who
used the TOFHLA as their reference standard, we used
the NVS and SAHL as reference standards. It is interesting to note that while nearly 60.5 % of our Spanish
speaking population had limited HL (using SAHL scores
as the reference) and 84.2 % had limited/marginal based
on NVS scores, only 22.4 % were categorized as having
inadequate HL based on SAHL scores. Our findings are
similar to those reported by Ramirez-Zohfeld and colleagues [39] in that categorization of participants into
levels of literacy is likely to vary across HL assessment
tool employed.
The overall proportion of low NVS scores could reflect
a combination of both low numeracy-related skills and/
Table 3 Area Under the Receiving Operating Curves (AUROC) for Health Literacy (HL) and Numeracy Screening Items Using Newest
Vital Sign (NVS) and Short Assessment of Health Literacy (SAHL) standards
Health Literacy and Numeracy Screening Item
Limited
Limited/Marginal Inadequate Health
Numeracy (NVS) Numeracy (NVS) Literacy (SAHL)
How often do you have problems learning about your medical condition
because of difficulty understanding written information?
0.27 (0.160.37)
0.46 (0.370.56)
0.47 (0.360.56)
How confident are you filling out medical forms by yourself?
0.75 (0.650.84)
0.66 (0.570.75)
0.69 (0.580.79)
How often do you have someone help you read hospital materials?
0.42 (0.270.57)
0.47 (0.370.56)
0.50 (0.400.60)
In general, how easy or hard do you find it to understand medical statistics?
0.71 (0.600.83)
0.61 (0.510.70)
0.59 (0.480.70)
How much do you agree or disagree with the following statement? In general, I feel
uncomfortable with health information that has a lot of numbers and statistics.
0.44 (0.320.57)
0.49 (0.400.59)
0.47 (0.360.59)
How much do you agree or disagree with the following statement? In general,
I depend on numbers and statistics to help me make decisions about my health.
0.44 (0.320.57)
0.49 (0.390.58)
0.40 (0.300.50)
Numeracy and HL levels based on NVS scores (limited = 0 or 1; marginal = 2 or 3) and SAHL scores (inadequate 14). AUROCs calculated with 95 %
confidence intervals
Singh et al. BMC Health Services Research (2015) 15:374
or unfamiliarity with nutrition labels among Spanish
speakers. Many of the participants tested were unsure of
how to read and interpret the ice cream nutrition label provided. Thus, NVS scores may not provide good discrimination of numeracy skill levels among Spanish speakers.
Future investigations should examine and compare the validity of different HL/numeracy assessment tools in Spanishspeaking and other diverse populations. Additionally, research is needed to explore whether gender differences exist
in self-report of health literacy. For example, among a
large sample of Taiwanese adults, Lee et al. [40] found that
womens responses to HL screening items reflected their
actual HL scores (as assessed by the Mandarin Health
Literacy Scale), whereas men tended to over-report their
actual HL skills. Further study is warranted to see if these
findings emerge in Spanish-speaking populations as well.
Our study findings should be considered in light of several potential limitations. First, participants in this study
were sampled in a single Midwestern city in the United
States drawn largely from free clinics where patients are
often uninsured and/or have modest incomes. As a result,
our findings may not be representative of other more
geographically and/or socioeconomically diverse settings.
Second, we were unable to stratify participants into more
detailed categories of educational attainment due to differences in schooling and descriptions used to describe the
educational systems in Spanish-speaking countries. Third,
our findings reflect the criterion validity of the HL and
numeracy screening items against both the NVS and
SAHL. Fourth, as with all observational studies that rely
on self-reports, response bias remains a possibility.
Conclusions
Brief one sentence HL and numeracy screening items have
utility in screening for limited HL and numeracy in
Spanish-speaking adults. The confident with forms item
discriminates well amongst Spanish-speaking adults with
varying HL and numeracy skills. This single question can
be easily administered in a variety of clinical settings and
eliminate the need for more formal and lengthy HL and/or
numeracy assessments.
Competing interests
The authors declare that they have no competing interests.
Authors contributions
RS: participated in the development and implementation of methods and
manuscript preparation, LC: participated in the development and
implementation of methods and manuscript preparation, and LW: conceived
of the study design, developed the methods, performed the statistical analysis,
drafted the original manuscript, and drafted the revised manuscript and
responses to peer reviewers. All authors read and approved the final manuscript.
Author details
1
The Ohio State University, Wexner College of Medicine, Columbus, OH
43210, USA. 2University of Kentucky, Lexington, KY 40506, USA. 3Department
of Family Medicine, The Ohio State University, 2231 North High Street,
Columbus, OH 43210, USA.
Page 6 of 7
Received: 21 February 2015 Accepted: 7 September 2015
References
1. Kutner M, Greenberg E, Jin Y, Paulsen, C. The health literacy of Americas Adults:
results from the 2003 National Assessment of Adult Literacy: National Center for
Education Statistics. Washington, DC: US Department of Education; 2006.
2. Dewalt DA, Berkman ND, Sheridan S, Lohr KN, Pignone MP. Literacy and
health outcomes: A systematic review of the literature. J Gen Intern Med.
2004;19:122839.
3. Smith PC, Brice JH, Lee J. The relationship between functional health
literacy and adherence to emergency department discharge instructions
among Spanish-speaking patients. J Natl Med Assoc. 2012;104:5217.
4. Samuels-Kalow ME, Stack AM, Porter SC. Parental language and dosing
errors after discharge from the pediatric emergency department.
Pediatr Emerg Care. 2013;29:9827.
5. Rosas-Salazar C, Ramratnam SK, Brehm JM, Han YY, Acosta-Prez E, Alvarez M,
et al. Parental numeracy and asthma exacerbations in Puerto Rican children.
Chest. 2013;144:928.
6. Pagn JA, Brown CJ, Asch DA, Armstrong K, Bastida E, Guerra C.
Health literacy and breast cancer screening among Mexican American
women in South Texas. J Cancer Educ. 2012;27:1327.
7. Davis TC, Long SW, Jackson RH, Mayeaux EJ, George RB, Murphy PW, et al.
Rapid estimate of adult literacy in medicine: a shortened screening
instrument. Fam Med. 1993;25:3915.
8. Parker RM, Baker DW, Williams MV, Nurss JR. The test of functional health
literacy in adults: a new instrument for measuring patients literacy skills.
J Gen Intern Med. 1995;10:53741.
9. Bann CM, McCormack LA, Berkman ND, Squiers LB. The health literacy skills
instrument: a 10-item short form. J Health Commun. 2012;17 Suppl 3:191202.
10. Hahn EA, Choi SW, Griffith JW, Yost KJ, Baker DW. Health literacy assessment
using talking touchscreen technology (Health LiTT): A new item response
theory-based measure of health literacy. J Health Commun. 2011;16 Suppl
3:15062.
11. Jordan JE, Buchbinder R, Briggs, AM, Elsworth GR, Busija L, Batterham R,
et al. The Health Literacy Management Scale (HeLMS): A measure of an
individuals capacity to seek, understand and use health information within
the healthcare setting. Patient Educ Couns. 2013;91:22835.
12. Bass PF, Wilson JF, Griffith CH, Barnett DR. Residents ability to identify
patients with poor literacy skills. Acad Med. 2002;77:103941.
13. Lindau ST, Tomori C, Lyons T, Langseth L, Bennett CL, Garcia P. The
association of health literacy with cervical cancer prevention knowledge
and health behaviors in a multiethnic cohort of women. Am J Obstet
Gynecol. 2002;186:93843.
14. Rogers ES, Wallace LS, Weiss BD. Misperceptions of medical understanding
in low-literacy patients: implications for cancer prevention. Cancer Control.
2006;13:2259.
15. Lee SY, Stucky BD, Lee JY, Rozier RG, Bender DE. Short assessment of health
literacy-Spanish and English: a comparable test of health literacy for Spanish
and English speakers. Health Serv Res. 2010;45:110520.
16. Weiss BD, Mays MZ, Martz W, Castro KM, DeWalt DA, Pignone MP, et al.
Quick assessment of literacy in primary care: the newest vital sign.
Ann Fam Med. 2005;3:51422.
17. Ishikawa N, Nomura K, Sato M, Yano E. Developing a measure of
communicative and critical health literacy: a pilot study of Japanese office
workers. Health Promot Int. 2008;23:26971.
18. Ishikawa N, Takeuchi T, Yano E. Measuring functional, communicative, and
critical health literacy among diabetic patients. Diabetes Care. 2008;31:8749.
19. Johnson K, Weiss BD. How long does it take to assess literacy skills in
clinical practice? J Am Board Fam Med. 2008;21:2114.
20. WelchVL, VanGeest JB, Caskey R. Time, costs, and clinical utilization of
screening for health literacy in primary care: A case study using the
Newest Vital Sign (NVS) instrument. J Am Board Fam Med. 2011;24:2819.
21. Baker DW, Parker RM, Williams MV, Pitkin K, Parikh NS, Coates W, et al.
The health care experience of patients with low literacy. Arch Fam Med.
1996;5:32934.
22. Parikh NS, Parker RM, Nurss JR, Baker DW, Williams MV. Shame and health
literacy: the unspoken connection. Patient Educ Couns. 1996;27:339.
23. Wolf MS, Williams MV, Parker RM, Parikh NS, Nowlan AW, Baker DW.
Patients shame and attitudes toward discussing the results of literacy
screening. J Health Comm. 2007;12:72132.
Singh et al. BMC Health Services Research (2015) 15:374
Page 7 of 7
24. VanGeest JB, Welch VL, Weiner SJ. Patients perceptions of screening for
healthliteracy: reactions to the Newest Vital Sign. J Health Comm.
2010;15:40212.
25. Chew LD, Bradley KA, Boyko EJ. Brief questions to identify patients with
inadequate health literacy. Fam Med. 2004;36:58894.
26. Wallace LS, Rogers ES, Roskos SE, Holiday DB, Weiss BD. Screening items to
identify patients with limited health literacy skills. J Gen Intern Med.
2006;21:8747.
27. Al Sayah F, Majumdar SR, Egede LE, Johnson JA. Measurement properties
and comparative performance of health literacy screening questions in a
predominantly low income African American population with diabetes.
Patient Educ Couns. 2014;97:8895.
28. Schwartz KL, Bartoces M, Campbell-Voytal K, West P, Monsur J, Sartor A,
et al. Estimating health literacy in family medicine clinics in metropolitan
Detroit: a MetroNet study. J Am Board Fam Med. 2013;26:56670.
29. Sarkar U, Schillinger D, Lpez A, Sudore R. Validation of self-reported health
literacy questions among diverse English and Spanish-speaking populations.
J Gen Intern Med. 2011;26:26571.
30. Cordasco KM, Homeier DC, Franco I, Wang PC, Sarkisian CA. Health literacy
screening of geriatric monolingual Spanish-speaking patients using singleitem literacy screening questions and education. Health Educ J.
2012;71:597605.
31. Behavioral Risk Factor Surveillance Survey2010 Spanish Questionnaire.
http://www.cdc.gov/brfss/annual_data/pdf-ques/q2010span.pdf Accessed
July 21, 2014.
32. Woloshin S, Schwartz LM, Welch HG. Patients and medical statistics.
Interest, confidence, and ability. J Gen Intern Med. 2005;20:9961000.
33. Fagerlin A, Zikmund-Fisher BJ, Ubel PA, Jankovic A, Derry HA, Smith DM.
Measuring numeracy without a math test: development of the Subjective
Numeracy Scale. Med Decis Making. 2007;27:67280.
34. Osborn CY, Weiss BD, Davis TC, Skripkauskas S, Rodrigue C, Bass PF, et al.
Measuring adult literacy in health care: performance of the newest vital
sign. Am J Health Behav. 2007;31 Suppl 1:S3646.
35. Patel PJ, Joel S, Rovena G, Pedireddy S, Saad S, Rachmale R, et al.
Testing the utility of the newest vital sign (NVS) health literacy assessment
tool in older African-American patients. Patient Educ Couns. 2011;85:5057.
36. Shah LC, West P, Bremmeyr K, Savoy-Moore RT. Health literacy instrument in
family medicine: the Newest Vital Sign ease of use and correlates.
J Am Board Fam Med. 2010;23:195203.
37. Stats Tudor. Spearmans correlation. http://www.statstutor.ac.uk/resources/
uploaded/spearmans.pdf Accessed July 30, 2015.
38. Stagliano V, Wallace LS. Brief health literacy screening items predict Newest
Vital Sign scores. J Am Board Fam Med. 2013;26:55865.
39. Ramirez-Zohfeld V, Rademaker AW, Dolan NC, Ferreira MR, Eder MM, Liu D,
et al. Comparing the performance of the S-TOFHLA and NVS among and
between English and Spanish speakers. J Health Comm. 2015;6:17.
40. Lee SY, Tsai TI, Tsai YW. Accuracy in self-reported health literacy screening:
A difference between men and women in Taiwan. BMJ Open.
2013;3(11):e002928.
Submit your next manuscript to BioMed Central
and take full advantage of:
Convenient online submission
Thorough peer review
No space constraints or color gure charges
Immediate publication on acceptance
Inclusion in PubMed, CAS, Scopus and Google Scholar
Research which is freely available for redistribution
Submit your manuscript at
www.biomedcentral.com/submit
You might also like
- Espanol medico y sociedad: Un libro para estudiantes de espanol en el tercer ano de estudios (Revised Edition)From EverandEspanol medico y sociedad: Un libro para estudiantes de espanol en el tercer ano de estudios (Revised Edition)No ratings yet
- Evidence-Based Public HealthDocument312 pagesEvidence-Based Public Healthnaravichandran3662100% (2)
- Music Assessment Rubric - Class Participation-2Document1 pageMusic Assessment Rubric - Class Participation-2api-299407251100% (2)
- AAFI Homeschooling Manual S.Y. 2022 - 2023Document27 pagesAAFI Homeschooling Manual S.Y. 2022 - 2023Tine Watts Azucena GalvezNo ratings yet
- Culture and Nonverbal Expressions of Empathy in Clinical Settings - A Systematic ReviewDocument49 pagesCulture and Nonverbal Expressions of Empathy in Clinical Settings - A Systematic ReviewAlberto JaramilloNo ratings yet
- The Inclusive Learning and Teaching HandbookDocument37 pagesThe Inclusive Learning and Teaching Handbookapi-194946381No ratings yet
- PEG Equity Framework Overview Rev 11 1Document4 pagesPEG Equity Framework Overview Rev 11 1APSEquityNo ratings yet
- ¡Necesito Un Medico!, But No One Speaks Spanish: A Look at Medical Interpretation PolicyDocument61 pages¡Necesito Un Medico!, But No One Speaks Spanish: A Look at Medical Interpretation PolicyGiulia SoligoNo ratings yet
- BarbarowiczDocument17 pagesBarbarowiczasriadiNo ratings yet
- Validation of Questionnaire On The Spiritual Needs Assessment For Patients (SNAP) Questionnaire in Brazilian PortugueseDocument10 pagesValidation of Questionnaire On The Spiritual Needs Assessment For Patients (SNAP) Questionnaire in Brazilian PortugueseGiovanna BertolinoNo ratings yet
- Assessing Medical Interpreters 重要 完Document21 pagesAssessing Medical Interpreters 重要 完NathanaëlNo ratings yet
- Research Paper Final DraftDocument19 pagesResearch Paper Final Draftapi-532628235No ratings yet
- Addressing Language and Culture Differences in Health Care Settings 2 PDFDocument4 pagesAddressing Language and Culture Differences in Health Care Settings 2 PDFWandi HuseinNo ratings yet
- Ireland Trip Final Paper - Language BarriersDocument12 pagesIreland Trip Final Paper - Language BarriersKelsi FarrenNo ratings yet
- Jurnal - 2Document15 pagesJurnal - 2ristytegarNo ratings yet
- Tutor - Critical AppraisalDocument8 pagesTutor - Critical AppraisalPriyanka TanwarNo ratings yet
- University of California PostprintsDocument37 pagesUniversity of California PostprintsPilar Galiano CruzNo ratings yet
- BMC Health Services Research: Digging Deeper: Quality of Patient-Provider Communication Across Hispanic SubgroupsDocument8 pagesBMC Health Services Research: Digging Deeper: Quality of Patient-Provider Communication Across Hispanic SubgroupsTitan LinggastiwiNo ratings yet
- Literature Review End of Life CareDocument4 pagesLiterature Review End of Life Caregpxmlevkg100% (1)
- Le N Et Al 2016 GerodontologyDocument9 pagesLe N Et Al 2016 GerodontologyBrijesh MaskeyNo ratings yet
- CFM Article 2014Document8 pagesCFM Article 2014Anjali SinglaNo ratings yet
- Connor Et Al. 2013 Functional Health Literacy in SwitzerlandDocument6 pagesConnor Et Al. 2013 Functional Health Literacy in SwitzerlandKitti SzpodnyiNo ratings yet
- Research Open AccessDocument14 pagesResearch Open AccessRob21aNo ratings yet
- 72.full - PDF ComDocument9 pages72.full - PDF ComNoNo ratings yet
- American Sign Language Interpreters Perceptions of Barriers To Healthcare Communication in Deaf and Hard of Hearing PatientsDocument6 pagesAmerican Sign Language Interpreters Perceptions of Barriers To Healthcare Communication in Deaf and Hard of Hearing Patientsapi-671390452No ratings yet
- Problem Solving and Diabetes Self-Management: Investigation in A Large, Multiracial SampleDocument5 pagesProblem Solving and Diabetes Self-Management: Investigation in A Large, Multiracial SampleAndreea MadalinaNo ratings yet
- Mathur Et Al 2016 GerodontologyDocument8 pagesMathur Et Al 2016 GerodontologyBrijesh MaskeyNo ratings yet
- Carson Kane Final Draft Project 2Document6 pagesCarson Kane Final Draft Project 2api-667077908No ratings yet
- A Review of Literature On Access To Primary Health CareDocument5 pagesA Review of Literature On Access To Primary Health CareafmzsbzbczhtbdNo ratings yet
- Mental Health Literature ReviewDocument5 pagesMental Health Literature Reviewfat1kifywel3100% (1)
- Culture Language and The Doctor Patient Relation Ship PDFDocument10 pagesCulture Language and The Doctor Patient Relation Ship PDFWagiono SuparanNo ratings yet
- Brazilian Version of A Lifestyle QuestionnaireDocument7 pagesBrazilian Version of A Lifestyle QuestionnaireAntônio de LimaNo ratings yet
- CrujjjjjDocument8 pagesCrujjjjjAlexander QuemadaNo ratings yet
- Development and Validation of A Functional Health Literacy Instrument in The PhilippinesDocument10 pagesDevelopment and Validation of A Functional Health Literacy Instrument in The PhilippinesIJPHSNo ratings yet
- Example of Public Health Literature ReviewDocument4 pagesExample of Public Health Literature Reviewc5qxzdj7100% (1)
- Nursing Interventions For Malnourished Children and Their Parents JournalDocument8 pagesNursing Interventions For Malnourished Children and Their Parents JournalroulyrosdianiNo ratings yet
- Literature Review of Palliative Care End of Life and DementiaDocument5 pagesLiterature Review of Palliative Care End of Life and DementialixdpuvkgNo ratings yet
- Hiv Aids Research Paper PDFDocument9 pagesHiv Aids Research Paper PDFcan3z5gx100% (1)
- Education Plays A Greater Role Than Age in Cognitive Test Performance Among Participants of The Brazilian Longitudinal Study of Adult Health (ELSA-Brasil)Document9 pagesEducation Plays A Greater Role Than Age in Cognitive Test Performance Among Participants of The Brazilian Longitudinal Study of Adult Health (ELSA-Brasil)Aishwarya PuttaNo ratings yet
- Komunikasi Dokter-PasienDocument7 pagesKomunikasi Dokter-PasienmeyfitaNo ratings yet
- Prolonged Noncoding RNA TDRKHAS1 Promotes Digestive Tract Most Cancers Cell Proliferation As Well As Intrusion Through The ?catenin Stimulated WNT Signaling Pathftgjm PDFDocument2 pagesProlonged Noncoding RNA TDRKHAS1 Promotes Digestive Tract Most Cancers Cell Proliferation As Well As Intrusion Through The ?catenin Stimulated WNT Signaling Pathftgjm PDFnewsmodem0No ratings yet
- Functional Assessment of Cancer Therapy-Brain Questionnaire: Translation and Linguistic Adaptation To Brazilian PortugueseDocument6 pagesFunctional Assessment of Cancer Therapy-Brain Questionnaire: Translation and Linguistic Adaptation To Brazilian PortugueserudolfpeterssonNo ratings yet
- Adulto MayorDocument13 pagesAdulto MayorFernanda MontalvoNo ratings yet
- Effective Health Communication: Guidance For EmployersDocument11 pagesEffective Health Communication: Guidance For EmployersvelwisherNo ratings yet
- The Danish Translation of The Medicines-Related Quality of Life (Mrqol) Scale From The Patient PerspectiveDocument15 pagesThe Danish Translation of The Medicines-Related Quality of Life (Mrqol) Scale From The Patient PerspectiveFACORI Farmacéuticos de Costa RicaNo ratings yet
- Hispanic Youth in Pregnancy Prevention Programs Research: An Analysis of The Research LiteratureDocument27 pagesHispanic Youth in Pregnancy Prevention Programs Research: An Analysis of The Research LiteratureUrbanYouthJusticeNo ratings yet
- Speros-Healthliteracyarticlejan 3448 PDFDocument8 pagesSperos-Healthliteracyarticlejan 3448 PDFSeptyadi David Eka Aryungga100% (1)
- Oral Health LiteracyDocument20 pagesOral Health Literacyapi-257281959No ratings yet
- The Impact of Perinatal HIV Infection On Older School-Aged Children's and Adolescents' Receptive Language and Word Recognition SkillsDocument9 pagesThe Impact of Perinatal HIV Infection On Older School-Aged Children's and Adolescents' Receptive Language and Word Recognition SkillsAndrew MoriartyNo ratings yet
- Health Literacy Among Older Adults A Systematic Literature ReviewDocument4 pagesHealth Literacy Among Older Adults A Systematic Literature ReviewcmaqqsrifNo ratings yet
- 2010 Article 1507Document7 pages2010 Article 1507Aisyah GirindraNo ratings yet
- Carson Kane EssayDocument8 pagesCarson Kane Essayapi-667077908No ratings yet
- Literature Review Example Mental HealthDocument4 pagesLiterature Review Example Mental Healthea6mkqw2100% (1)
- Stroke Article 1Document10 pagesStroke Article 1api-292843843No ratings yet
- Jced 11 E1143Document8 pagesJced 11 E1143rugeaelzwea2No ratings yet
- 2013 Development and Psychometric Testing of The Hemophilia Well-Being Index IJBM 20, 609-617Document9 pages2013 Development and Psychometric Testing of The Hemophilia Well-Being Index IJBM 20, 609-617Miguel OchoaNo ratings yet
- Chapter 2 Reviewsof Related Literatureand Related Studies TopicalDocument14 pagesChapter 2 Reviewsof Related Literatureand Related Studies Topicalr76914751No ratings yet
- Oral Care Literature ReviewDocument7 pagesOral Care Literature Reviewafmzfsqopfanlw100% (1)
- Public Health Dissertation ExamplesDocument4 pagesPublic Health Dissertation ExamplesWhereToBuyWritingPaperCanada100% (1)
- Of Health Literacy For Spanish-Speaking Adults en Chile, para MedirDocument7 pagesOf Health Literacy For Spanish-Speaking Adults en Chile, para MedirLuis Luengo MachucaNo ratings yet
- The Minnesota Living With Heart Failure QuestionnaDocument11 pagesThe Minnesota Living With Heart Failure Questionnamgarcía_62490No ratings yet
- Culture, Language, and The Doctor-Patient Relationship: Escholarship@UmmsDocument10 pagesCulture, Language, and The Doctor-Patient Relationship: Escholarship@UmmsBUAHIN JANNANo ratings yet
- Dissertation Clinical TrialsDocument5 pagesDissertation Clinical TrialsCanSomeoneWriteMyPaperForMeSingapore100% (1)
- Bob Marley - No Woman No CryDocument4 pagesBob Marley - No Woman No CryRob21aNo ratings yet
- Impacto Health Literacy Nos OutcomesDocument11 pagesImpacto Health Literacy Nos OutcomesRob21aNo ratings yet
- Boss Ve-20 ManualDocument144 pagesBoss Ve-20 ManualCarlo Mauricio González Parra100% (1)
- Public Health and Online Misinformation: Challenges and RecommendationsDocument19 pagesPublic Health and Online Misinformation: Challenges and RecommendationsRob21aNo ratings yet
- Research Open AccessDocument14 pagesResearch Open AccessRob21aNo ratings yet
- PSR-SX700: Category Style Name Category Style Name Category Style Name Category Style NameDocument2 pagesPSR-SX700: Category Style Name Category Style Name Category Style Name Category Style NameRob21aNo ratings yet
- Oral Health PromotionDocument29 pagesOral Health PromotionRob21aNo ratings yet
- Lit Review CS and Medical EducationDocument14 pagesLit Review CS and Medical EducationRob21aNo ratings yet
- Health Literacy ConcurrentDocument5 pagesHealth Literacy ConcurrentRob21aNo ratings yet
- International Journal of Nursing Studies: Tze-Fang Wang, Chiu-Mieh Huang, Chyuan Chou, Shu YuDocument7 pagesInternational Journal of Nursing Studies: Tze-Fang Wang, Chiu-Mieh Huang, Chyuan Chou, Shu YuRob21aNo ratings yet
- Self-Empowerment in Health PromotionDocument7 pagesSelf-Empowerment in Health PromotionRob21aNo ratings yet
- Wiley Milbank Memorial FundDocument22 pagesWiley Milbank Memorial FundRob21aNo ratings yet
- Level 3 Cost Accounting - SyllabusDocument17 pagesLevel 3 Cost Accounting - SyllabusChan Siew ChongNo ratings yet
- PE General Lesson Plan Template: Central FocusDocument7 pagesPE General Lesson Plan Template: Central Focusapi-396137633No ratings yet
- Self-Study Report Part-IiDocument21 pagesSelf-Study Report Part-IiSajja SrinivasNo ratings yet
- 2016 NCAE Orientation School LevelDocument28 pages2016 NCAE Orientation School LevelClaudette G. PolicarpioNo ratings yet
- Science Unit PlannerDocument13 pagesScience Unit Plannerapi-324855292No ratings yet
- Typhoon PARDocument5 pagesTyphoon PARreynaldo banaria jrNo ratings yet
- TT&SC Chapter2 M3.3 FlorendoDocument2 pagesTT&SC Chapter2 M3.3 FlorendoEfren Garcia FlorendoNo ratings yet
- A Review of Digital Literacy AssessmentDocument31 pagesA Review of Digital Literacy AssessmentDeasy IrawatiNo ratings yet
- Assignment 3 Syllabus BrowniDocument10 pagesAssignment 3 Syllabus Browniapi-258058489No ratings yet
- EntryPracRPNDocument20 pagesEntryPracRPNBiju ChackoNo ratings yet
- Writing Samples B2Document48 pagesWriting Samples B2nota32100% (4)
- Seatwork 2 BTVTED 2ADocument67 pagesSeatwork 2 BTVTED 2ACharlton Benedict BernabeNo ratings yet
- Task 4b Math Learning SegementsDocument2 pagesTask 4b Math Learning Segementsapi-283217268No ratings yet
- P1 - Professional Accountant Practice and RevisiDocument449 pagesP1 - Professional Accountant Practice and Revisiarmaan100% (2)
- Maryam Assignment 2Document22 pagesMaryam Assignment 2hammad asgharNo ratings yet
- Reflection 3 Life Cycle of A PumpkinDocument4 pagesReflection 3 Life Cycle of A Pumpkinapi-177768681No ratings yet
- APU-APIIT Ethics Approval Process - Introduction and GuidanceDocument7 pagesAPU-APIIT Ethics Approval Process - Introduction and GuidanceVernon LohNo ratings yet
- 2015 PSSA Item and Scoring Sampler Science Grade 8Document36 pages2015 PSSA Item and Scoring Sampler Science Grade 8Chase FloydNo ratings yet
- 12 SMAW W 1 - Types of Welding PositionsDocument10 pages12 SMAW W 1 - Types of Welding PositionsNelPalalonNo ratings yet
- IEEE Wireless Communication Engineering Technologies Certification Candidate's Handbook 2018Document53 pagesIEEE Wireless Communication Engineering Technologies Certification Candidate's Handbook 2018jeanneptuneNo ratings yet
- Annexure-147. (Ling - UG - Revised)Document33 pagesAnnexure-147. (Ling - UG - Revised)pranjal sharmaNo ratings yet
- Module in PBADocument3 pagesModule in PBAAcire NonacNo ratings yet
- Primary Election Unit PlanDocument4 pagesPrimary Election Unit Planapi-249957841No ratings yet
- MPU For Certificate (Level 3) : Summary of Information On Each ModuleDocument3 pagesMPU For Certificate (Level 3) : Summary of Information On Each ModuleWilliam AnthonyNo ratings yet
- Section FourDocument13 pagesSection Fourapi-532404528No ratings yet
- Pitch Lesson PlanDocument6 pagesPitch Lesson Planapi-318222702No ratings yet