Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5834)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Critically Discuss The Public Health Approach To Population HealthDocument3 pagesCritically Discuss The Public Health Approach To Population HealthMDUDUZI SIBANDA100% (3)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (405)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Step 2 CK - NBME 7 Answers UncompleteDocument16 pagesStep 2 CK - NBME 7 Answers UncompleteDuke83% (12)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Normal Flora of HumanDocument54 pagesNormal Flora of Humankumari astha rupaliNo ratings yet
- Pco RcogDocument15 pagesPco RcogganotNo ratings yet
- FFP and Cryoprecipitate FinalDocument6 pagesFFP and Cryoprecipitate FinalganotNo ratings yet
- Amniotic Band SyndromeDocument5 pagesAmniotic Band SyndromeganotNo ratings yet
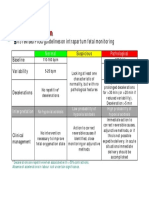
- CTG Classification PDFDocument1 pageCTG Classification PDFganotNo ratings yet
- Pharmacokinetics: - Not Bound To Plasma Proteins - Is Eliminated by The Kidneys and Liver - T1/2 5 MinutesDocument7 pagesPharmacokinetics: - Not Bound To Plasma Proteins - Is Eliminated by The Kidneys and Liver - T1/2 5 MinutesganotNo ratings yet
- Puberty Growth Spurt Age in Local Population - A StudyDocument6 pagesPuberty Growth Spurt Age in Local Population - A StudyganotNo ratings yet
- Second Messenger SystemsModDocument49 pagesSecond Messenger SystemsModganotNo ratings yet
- Cranial Fixation SystemsDocument12 pagesCranial Fixation SystemsMostafa YounisNo ratings yet
- Mosby's Comprehensive Review of Nursing For The NCLEX-RN® ExaminationDocument2 pagesMosby's Comprehensive Review of Nursing For The NCLEX-RN® ExaminationNursyNurseNo ratings yet
- Forensic Chem and Toxicology ReviewerDocument40 pagesForensic Chem and Toxicology ReviewerJohn Carl DomingoNo ratings yet
- Literature Review On CokeDocument6 pagesLiterature Review On Cokeafmzkbuvlmmhqq100% (1)
- Clinical Health Psychologists in The NHSDocument18 pagesClinical Health Psychologists in The NHSJayashri PatilNo ratings yet
- Clinical Service ManagementDocument5 pagesClinical Service ManagementdharatriNo ratings yet
- Tracheostomy Care and Suctioning Care ProcedureDocument12 pagesTracheostomy Care and Suctioning Care ProcedureMonna Llee Monte DimarananNo ratings yet
- Primary Malignant Tumors of The Spine: Gregory S. Mcloughlin Daniel M. Sciubba Jean-Paul WolinskyDocument12 pagesPrimary Malignant Tumors of The Spine: Gregory S. Mcloughlin Daniel M. Sciubba Jean-Paul Wolinskymetasoniko81No ratings yet
- Diabetes Awarenessin KG KapokDocument4 pagesDiabetes Awarenessin KG Kapokempus CatNo ratings yet
- Printable Article "Meet A Scientist Who Studies The Human MicrobiomeDocument2 pagesPrintable Article "Meet A Scientist Who Studies The Human MicrobiomeRick WuNo ratings yet
- Parto Prematuro ACOGDocument10 pagesParto Prematuro ACOGAngela_Maria_M_7864No ratings yet
- PharmacologyDocument1 pagePharmacologyایم ناولسٹNo ratings yet
- Lumbar Puncture: What You Should KnowDocument5 pagesLumbar Puncture: What You Should KnowQueen SiLogNo ratings yet
- Lecture-11 Breech PresentationDocument27 pagesLecture-11 Breech PresentationMadhu Sudhan PandeyaNo ratings yet
- "Ang Propesyon Na Aking Nais Pasukin": InfomercialDocument3 pages"Ang Propesyon Na Aking Nais Pasukin": InfomercialMaria Veronica BubanNo ratings yet
- Yale Brown Obsessive Compulsive Scale With Reference To The Last WeekDocument7 pagesYale Brown Obsessive Compulsive Scale With Reference To The Last WeekAnant KhotNo ratings yet
- Voloxal TabletsDocument9 pagesVoloxal Tabletselcapitano vegetaNo ratings yet
- Jeyakumar Dhileeban Rrroll 41Document34 pagesJeyakumar Dhileeban Rrroll 41Rupesh TamizhaNo ratings yet
- Laboratory Diagnosis of Cancer Morphologic MethodsDocument7 pagesLaboratory Diagnosis of Cancer Morphologic MethodsRafaih KhanNo ratings yet
- Human Body Modeling ANSYS Software PDFDocument53 pagesHuman Body Modeling ANSYS Software PDFSrashmi100% (1)
- ICBA NotesDocument60 pagesICBA NotesAndrew EldeiryNo ratings yet
- Drug and Therapeutics Committee: Session 10. Standard Treatment GuidelinesDocument22 pagesDrug and Therapeutics Committee: Session 10. Standard Treatment GuidelinesbaburamNo ratings yet
- Main EssayDocument7 pagesMain EssayKen UcheonyeNo ratings yet
- ARTHRITISDocument4 pagesARTHRITISJk FloresNo ratings yet
- Perez TMC-213 Module-2Document4 pagesPerez TMC-213 Module-2NISHA MIKLE MACULNo ratings yet
- JPM 13 00098Document15 pagesJPM 13 00098Maria Júlia ProtiNo ratings yet
- Health10 Q4 M7Document12 pagesHealth10 Q4 M7memnochmangubat1104No ratings yet