
B Veda Et Al 2015 Endodontic Topics
B Veda Et Al 2015 Endodontic Topics
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5822)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- PDF Bobcat s175 s185 Service Repair Manual SN 525011001 525111001 525211001 525311001 and AboveDocument933 pagesPDF Bobcat s175 s185 Service Repair Manual SN 525011001 525111001 525211001 525311001 and AboveChristian Cepeda86% (7)
- Mcq. SurgeryDocument132 pagesMcq. Surgeryمنتظر اللاميNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Final Types of TourismDocument4 pagesFinal Types of TourismErika Mae CavanNo ratings yet
- A Heartbreaking Work of Staggering Genius LessonplanDocument229 pagesA Heartbreaking Work of Staggering Genius LessonplanMahmoud El SheikhNo ratings yet
- Yoga 530Document90 pagesYoga 530Juan LatorreNo ratings yet
- Gas LawsDocument16 pagesGas LawsKakoli RoyNo ratings yet
- Vaginal Discharge in DogsDocument5 pagesVaginal Discharge in DogsDarmawan Prastyo100% (1)
- No Homework PolicyDocument2 pagesNo Homework PolicyKyla BetchaydaNo ratings yet
- Desoldering Tool: Designed For Lead FreeDocument2 pagesDesoldering Tool: Designed For Lead FreeMarco Antonio Ortiz RomeroNo ratings yet
- A Tale of Two CountriesDocument10 pagesA Tale of Two CountriesSandra BoteroNo ratings yet
- Bar97specs Part2Document47 pagesBar97specs Part2N J Vargas SampayoNo ratings yet
- MultiTherm OG-1® Tech DataDocument2 pagesMultiTherm OG-1® Tech DataSteranskoNo ratings yet
- Process, People, and Conflict Management in OrganizationsDocument6 pagesProcess, People, and Conflict Management in OrganizationsMeldy IamNo ratings yet
- Funda Lec MidtermsDocument13 pagesFunda Lec MidtermsCharisse CaydanNo ratings yet
- Chemical Equilibrium Part 2Document26 pagesChemical Equilibrium Part 2adityayadav18julyNo ratings yet
- Biography of John Mordecai Gottman 1Document4 pagesBiography of John Mordecai Gottman 1kalitkalitNo ratings yet
- KOMAKINO1 - 43643 - 1493201559720 - Kammprofile-TechData-ENKAMMPROFILE GASKETDocument4 pagesKOMAKINO1 - 43643 - 1493201559720 - Kammprofile-TechData-ENKAMMPROFILE GASKETguojun sunNo ratings yet
- Hawthorne ExperimentsDocument14 pagesHawthorne ExperimentsShalini SharmaNo ratings yet
- CED-PQP-5225-F01 Rev.0 Sieve AnalysisDocument4 pagesCED-PQP-5225-F01 Rev.0 Sieve AnalysisSslan seelanNo ratings yet
- S60 Cylinder Kit Failure Analysis MethodDocument10 pagesS60 Cylinder Kit Failure Analysis MethodKepler452bNo ratings yet
- 48 Weeks To Total M-Powerment!Document18 pages48 Weeks To Total M-Powerment!sundevil2010usa4605No ratings yet
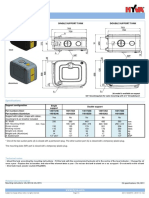
- Hyva Oil Tank: Single Support Tank Double Support TankDocument4 pagesHyva Oil Tank: Single Support Tank Double Support TankPutera Bumi NusantaraNo ratings yet
- The English Opening: Grandmaster Repertoire 3Document10 pagesThe English Opening: Grandmaster Repertoire 3lietotajs71No ratings yet
- Wallmat Supply Chain Analysis PDFDocument44 pagesWallmat Supply Chain Analysis PDFProsenjit RoyNo ratings yet
- Vitamins & Minerals: Name: - DateDocument1 pageVitamins & Minerals: Name: - DateWiktoria StahlNo ratings yet
- Azo Dyes and Their ApplicationsDocument6 pagesAzo Dyes and Their ApplicationsMUhammad AsifNo ratings yet
- Snowball SamplingDocument3 pagesSnowball SamplingHamza ChNo ratings yet
- For Abm Only Bmat 2ND Quarter ActivitiesDocument24 pagesFor Abm Only Bmat 2ND Quarter ActivitiesjohnNo ratings yet
- Prosecutor v. FurundzijaDocument1 pageProsecutor v. Furundzijacrlstinaaa100% (1)
- #Tutorial 3 - Fossil Fule Steam Generators TroubleshootingDocument5 pages#Tutorial 3 - Fossil Fule Steam Generators Troubleshootingmohamed EldesokyNo ratings yet






































































Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5822)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- PDF Bobcat s175 s185 Service Repair Manual SN 525011001 525111001 525211001 525311001 and AboveDocument933 pagesPDF Bobcat s175 s185 Service Repair Manual SN 525011001 525111001 525211001 525311001 and AboveChristian Cepeda86% (7)
- Mcq. SurgeryDocument132 pagesMcq. Surgeryمنتظر اللاميNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Final Types of TourismDocument4 pagesFinal Types of TourismErika Mae CavanNo ratings yet
- A Heartbreaking Work of Staggering Genius LessonplanDocument229 pagesA Heartbreaking Work of Staggering Genius LessonplanMahmoud El SheikhNo ratings yet
- Yoga 530Document90 pagesYoga 530Juan LatorreNo ratings yet
- Gas LawsDocument16 pagesGas LawsKakoli RoyNo ratings yet
- Vaginal Discharge in DogsDocument5 pagesVaginal Discharge in DogsDarmawan Prastyo100% (1)
- No Homework PolicyDocument2 pagesNo Homework PolicyKyla BetchaydaNo ratings yet
- Desoldering Tool: Designed For Lead FreeDocument2 pagesDesoldering Tool: Designed For Lead FreeMarco Antonio Ortiz RomeroNo ratings yet
- A Tale of Two CountriesDocument10 pagesA Tale of Two CountriesSandra BoteroNo ratings yet
- Bar97specs Part2Document47 pagesBar97specs Part2N J Vargas SampayoNo ratings yet
- MultiTherm OG-1® Tech DataDocument2 pagesMultiTherm OG-1® Tech DataSteranskoNo ratings yet
- Process, People, and Conflict Management in OrganizationsDocument6 pagesProcess, People, and Conflict Management in OrganizationsMeldy IamNo ratings yet
- Funda Lec MidtermsDocument13 pagesFunda Lec MidtermsCharisse CaydanNo ratings yet
- Chemical Equilibrium Part 2Document26 pagesChemical Equilibrium Part 2adityayadav18julyNo ratings yet
- Biography of John Mordecai Gottman 1Document4 pagesBiography of John Mordecai Gottman 1kalitkalitNo ratings yet
- KOMAKINO1 - 43643 - 1493201559720 - Kammprofile-TechData-ENKAMMPROFILE GASKETDocument4 pagesKOMAKINO1 - 43643 - 1493201559720 - Kammprofile-TechData-ENKAMMPROFILE GASKETguojun sunNo ratings yet
- Hawthorne ExperimentsDocument14 pagesHawthorne ExperimentsShalini SharmaNo ratings yet
- CED-PQP-5225-F01 Rev.0 Sieve AnalysisDocument4 pagesCED-PQP-5225-F01 Rev.0 Sieve AnalysisSslan seelanNo ratings yet
- S60 Cylinder Kit Failure Analysis MethodDocument10 pagesS60 Cylinder Kit Failure Analysis MethodKepler452bNo ratings yet
- 48 Weeks To Total M-Powerment!Document18 pages48 Weeks To Total M-Powerment!sundevil2010usa4605No ratings yet
- Hyva Oil Tank: Single Support Tank Double Support TankDocument4 pagesHyva Oil Tank: Single Support Tank Double Support TankPutera Bumi NusantaraNo ratings yet
- The English Opening: Grandmaster Repertoire 3Document10 pagesThe English Opening: Grandmaster Repertoire 3lietotajs71No ratings yet
- Wallmat Supply Chain Analysis PDFDocument44 pagesWallmat Supply Chain Analysis PDFProsenjit RoyNo ratings yet
- Vitamins & Minerals: Name: - DateDocument1 pageVitamins & Minerals: Name: - DateWiktoria StahlNo ratings yet
- Azo Dyes and Their ApplicationsDocument6 pagesAzo Dyes and Their ApplicationsMUhammad AsifNo ratings yet
- Snowball SamplingDocument3 pagesSnowball SamplingHamza ChNo ratings yet
- For Abm Only Bmat 2ND Quarter ActivitiesDocument24 pagesFor Abm Only Bmat 2ND Quarter ActivitiesjohnNo ratings yet
- Prosecutor v. FurundzijaDocument1 pageProsecutor v. Furundzijacrlstinaaa100% (1)
- #Tutorial 3 - Fossil Fule Steam Generators TroubleshootingDocument5 pages#Tutorial 3 - Fossil Fule Steam Generators Troubleshootingmohamed EldesokyNo ratings yet