Download as pdf or txt
You might also like
- MurderousGhosts MCbookDocument20 pagesMurderousGhosts MCbookJ MNo ratings yet
- Victims of CrimeDocument11 pagesVictims of Crimesuela35No ratings yet
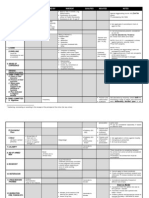
- Aggravating Circumstances TableDocument4 pagesAggravating Circumstances TableNeil Mayor100% (1)
- Dallas Police Department Reports: Offense Record For Public ReleaseDocument2 pagesDallas Police Department Reports: Offense Record For Public ReleaseAnonymous ovJgHANo ratings yet
- Psychological Disorder Movie Review - Saving Private RyanDocument4 pagesPsychological Disorder Movie Review - Saving Private RyanBeccaShanksNo ratings yet
- Lecture 2 - Causation (1) - 1Document38 pagesLecture 2 - Causation (1) - 1AyaanNo ratings yet
- Uma Intervenção Clínica Realizada Por Enfermeiros para Tratar Da Violência Por Parceiro Íntimo Entre Mulheres de Baixa Renda Na Cidade Do MéxicoDocument12 pagesUma Intervenção Clínica Realizada Por Enfermeiros para Tratar Da Violência Por Parceiro Íntimo Entre Mulheres de Baixa Renda Na Cidade Do MéxicoLorrany Prado QuirinoNo ratings yet
- BAREMDocument9 pagesBAREMbaremayubaNo ratings yet
- AYUBADocument11 pagesAYUBAbaremayubaNo ratings yet
- 222222222Document7 pages222222222Sadaf AliNo ratings yet
- BMC Health Services Research: Choice of Healthcare Provider Following Reform in VietnamDocument9 pagesBMC Health Services Research: Choice of Healthcare Provider Following Reform in VietnamjlventiganNo ratings yet
- Primary Health Care Services Utilization in Gombe Metropolis, Gombe State NigeriaDocument9 pagesPrimary Health Care Services Utilization in Gombe Metropolis, Gombe State NigeriaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- JournalDocument13 pagesJournalCharlaine Gripal SudlaNo ratings yet
- JHJHJJHDocument14 pagesJHJHJJHnur arifahNo ratings yet
- Hancart Communications 2003-Fev2009Document10 pagesHancart Communications 2003-Fev2009pascalehp100% (2)
- 2013 - NCDs Access - S AFrica - Ibanez-GonzalesDocument6 pages2013 - NCDs Access - S AFrica - Ibanez-Gonzalesdedihsuandi1495No ratings yet
- ACSM Review - PakistanDocument8 pagesACSM Review - PakistanK SNo ratings yet
- Primary Health Care Essay 2011Document7 pagesPrimary Health Care Essay 2011David Kingston0% (1)
- First Recourse For Care-Seeking and Associated FacDocument14 pagesFirst Recourse For Care-Seeking and Associated FacChristian MolimaNo ratings yet
- Why Physicians and Nurses Ask (Or Don 'T) About Partner Violence: A Qualitative AnalysisDocument12 pagesWhy Physicians and Nurses Ask (Or Don 'T) About Partner Violence: A Qualitative Analysisionut pandelescuNo ratings yet
- DarenoDocument14 pagesDarenoguohong huNo ratings yet
- Björkman Svensson 2008Document36 pagesBjörkman Svensson 2008NPNo ratings yet
- Publish 2011Document41 pagesPublish 2011hsrimediaNo ratings yet
- Obsos 2Document13 pagesObsos 2Iin Sakinah DewiNo ratings yet
- Apc 2016 0213Document11 pagesApc 2016 0213Amos AprekuNo ratings yet
- Improving The Healthcare Response To Domestic Violence and Abuse in UK Primary Care: Interrupted Time Series Evaluation of A System-Level Training and Support ProgrammeDocument10 pagesImproving The Healthcare Response To Domestic Violence and Abuse in UK Primary Care: Interrupted Time Series Evaluation of A System-Level Training and Support ProgrammePatrick SanchezNo ratings yet
- Home-Based Care: A Need Assessment of People Living With HIV Infection in Bandung, IndonesiaDocument9 pagesHome-Based Care: A Need Assessment of People Living With HIV Infection in Bandung, IndonesiaLiza Marie Cayetano AdarneNo ratings yet
- JURNAL McuDocument9 pagesJURNAL McusilviaNo ratings yet
- Women Offender Transition and Reentry: Gender Responsive Approaches To Transitioning Women Offenders From Prison To The CommunityDocument44 pagesWomen Offender Transition and Reentry: Gender Responsive Approaches To Transitioning Women Offenders From Prison To The CommunityPaola GualterosNo ratings yet
- Rbap-Hhd-2013-Bhutan-Advocacy-Framework 1Document28 pagesRbap-Hhd-2013-Bhutan-Advocacy-Framework 1api-325234393No ratings yet
- World Health Organization: by Wendy BraunDocument8 pagesWorld Health Organization: by Wendy BraunAnonymous AvbmJ5JTNo ratings yet
- Bmri2019 4717485Document9 pagesBmri2019 4717485Kusumadewi WidiarsaNo ratings yet
- Essential ArticleDocument16 pagesEssential Articleapi-708352337No ratings yet
- A Pilot Study of Mobile Telephone Message Interventions With Suicide Attempters in ChinaDocument4 pagesA Pilot Study of Mobile Telephone Message Interventions With Suicide Attempters in ChinaFunkifizeNo ratings yet
- Maternal 1Document10 pagesMaternal 1Inty Defly NandNo ratings yet
- The Scope and Impact of Mobile HealthDocument12 pagesThe Scope and Impact of Mobile Healthdrestadyumna ChilspiderNo ratings yet
- Male Circumcision Peer Effects and Risk Compensation - ALLDocument68 pagesMale Circumcision Peer Effects and Risk Compensation - ALLmandcrutNo ratings yet
- Term Paper For FumiDocument10 pagesTerm Paper For Fumiajiboyetitilayo64No ratings yet
- SantosSalas2019 SocialDisparitiesDocument12 pagesSantosSalas2019 SocialDisparitiesAdriana VargasNo ratings yet
- His 5Document167 pagesHis 5Anjum100% (5)
- Workplace Violence Against Nurses in The Gambia: Mixed Methods DesignDocument11 pagesWorkplace Violence Against Nurses in The Gambia: Mixed Methods DesignFaidhil NersNo ratings yet
- Targetted Intervention Program For Sex Work ProfessionalsDocument14 pagesTargetted Intervention Program For Sex Work ProfessionalsJuree HojaiNo ratings yet
- Bjrkman PowerPeopleEvidence 2009Document36 pagesBjrkman PowerPeopleEvidence 2009maria jose vegaNo ratings yet
- Research RelatedDocument28 pagesResearch Relatedkrystelle jade labineNo ratings yet
- Jurnal 4 HivDocument14 pagesJurnal 4 HivSabrina RahmaNo ratings yet
- Tulloch2015 Article PatientAndCommunityExperiencesDocument9 pagesTulloch2015 Article PatientAndCommunityExperiencesNamira Firdha KNo ratings yet
- Factors promoting resilience among breast cancer patientsDocument12 pagesFactors promoting resilience among breast cancer patientsffzefanyaNo ratings yet
- Factors Influencing Self-Management of Adults Living With HIV On Antiretroviral Therapy in Northwest Ethiopia: A Cross-Sectional StudyDocument11 pagesFactors Influencing Self-Management of Adults Living With HIV On Antiretroviral Therapy in Northwest Ethiopia: A Cross-Sectional Studyvero060112.vcNo ratings yet
- Jurnal 2Document16 pagesJurnal 2Edwin Pasha Jr.No ratings yet
- Ieh201 1Document8 pagesIeh201 1Myless MukendiNo ratings yet
- Meta 2Document14 pagesMeta 2S2-IKM ULMNo ratings yet
- هنادىDocument10 pagesهنادىhanady shehataNo ratings yet
- Nurses' Perceptions of Barriers and Supportive Behaviors in End-Of-Life Care in The Intensive Care Unit: A Cross-Sectional StudyDocument10 pagesNurses' Perceptions of Barriers and Supportive Behaviors in End-Of-Life Care in The Intensive Care Unit: A Cross-Sectional Studycarolina riveraNo ratings yet
- Healthcare Choices in Mumbai Slums A Cross-SectionDocument21 pagesHealthcare Choices in Mumbai Slums A Cross-SectionIshwarya RaghuNo ratings yet
- Iran, Educational Interventions 2021Document11 pagesIran, Educational Interventions 2021JEEJANo ratings yet
- The Use of Reproductive Healthcare at Commune Health Stations in A Changing Health System in VietnamDocument9 pagesThe Use of Reproductive Healthcare at Commune Health Stations in A Changing Health System in VietnamjlventiganNo ratings yet
- Trends of Violence Against Healthcare by ShaheerDocument9 pagesTrends of Violence Against Healthcare by ShaheerShaheer zia100% (1)
- Drug-Related StigmaDocument8 pagesDrug-Related StigmamabelaNo ratings yet
- BMJGH 2017 000327Document7 pagesBMJGH 2017 000327MustafaNo ratings yet
- Paper 1Document10 pagesPaper 1lsnzgiNo ratings yet
- Web-Based Harm Reduction Intervention For Chemsex in Men Who Have Sex With Men: Randomized Controlled TrialDocument14 pagesWeb-Based Harm Reduction Intervention For Chemsex in Men Who Have Sex With Men: Randomized Controlled TrialEdmond ChoiNo ratings yet
- Prevention and Health Education How Recent Advances in TheDocument4 pagesPrevention and Health Education How Recent Advances in TheNataLya MendilaNo ratings yet
- Stigmatised DDocument11 pagesStigmatised Darfa ahmadNo ratings yet
- Components Practices and Benefits of Home Based Care of Hiv and Aids Patients in Kenya Butula Local Communitys PerspectiveDocument9 pagesComponents Practices and Benefits of Home Based Care of Hiv and Aids Patients in Kenya Butula Local Communitys PerspectiveJane Wa MugogoNo ratings yet
- Improving Malaria Knowledge and Practices in Rural Myanmar Through A Village Health Worker Intervention: A Cross-Sectional StudyDocument5 pagesImproving Malaria Knowledge and Practices in Rural Myanmar Through A Village Health Worker Intervention: A Cross-Sectional StudyMuji SuswantoNo ratings yet
- Meeting the Needs of Older Adults with Serious Illness: Challenges and Opportunities in the Age of Health Care ReformFrom EverandMeeting the Needs of Older Adults with Serious Illness: Challenges and Opportunities in the Age of Health Care ReformAmy S. KelleyNo ratings yet
- Sept 2015 Crim Law DigestsDocument15 pagesSept 2015 Crim Law Digestsjerwin rodelasNo ratings yet
- Crim Finals Cases 2Document13 pagesCrim Finals Cases 2Ella QuiNo ratings yet
- Lindsay Saunders-Velez v. Colorado Department of Corrections, Et. Al.: Request For Temporary Restraining OrderDocument9 pagesLindsay Saunders-Velez v. Colorado Department of Corrections, Et. Al.: Request For Temporary Restraining OrderMichael_Lee_RobertsNo ratings yet
- Criminal Law Book 2Document6 pagesCriminal Law Book 2John Felix Andal100% (1)
- PNP - Article HandbookDocument7 pagesPNP - Article Handbookjacob nobleNo ratings yet
- WPV State of HawaiiDocument213 pagesWPV State of HawaiiJack PlaxeNo ratings yet
- 2008green Book CommunityResourceDirectoryDocument64 pages2008green Book CommunityResourceDirectoryrfleming100% (2)
- WWW Targeted One 2020 09-16-6213 Garden Acre Drive Fort Worth StalkingDocument10 pagesWWW Targeted One 2020 09-16-6213 Garden Acre Drive Fort Worth StalkingDaniel LNo ratings yet
- Murder, Sexual Assault, Narcotic Trafficking Alaska National GuardDocument12 pagesMurder, Sexual Assault, Narcotic Trafficking Alaska National Guardmary engNo ratings yet
- Law of Torts (Trespass To Person)Document2 pagesLaw of Torts (Trespass To Person)Zafar Azeemi100% (1)
- Finished Proposal With ReflectionDocument11 pagesFinished Proposal With Reflectionapi-310735110No ratings yet
- Peoria County Booking Sheet 07/29/15Document11 pagesPeoria County Booking Sheet 07/29/15Journal Star police documentsNo ratings yet
- Crimes Against PersonDocument5 pagesCrimes Against PersonTata YoungNo ratings yet
- Types of Abuse and ExamplesDocument4 pagesTypes of Abuse and Exampleslly89395No ratings yet
- RAPE (RPC, ART. 266-A) : HangoversDocument2 pagesRAPE (RPC, ART. 266-A) : HangoversJose MasarateNo ratings yet
- 2011 Torts Exam NotesDocument24 pages2011 Torts Exam NotesAnthony Celi100% (1)
- Hidden Texts of Nostradamus Part OneDocument21 pagesHidden Texts of Nostradamus Part OnejosephkiwiNo ratings yet
- People Vs Cupino GR No. 125688 FactsDocument6 pagesPeople Vs Cupino GR No. 125688 FactstinctNo ratings yet
- Legal Med Physical InjuriesDocument78 pagesLegal Med Physical InjuriesTammy YahNo ratings yet
- What Is The Me Too MovementDocument13 pagesWhat Is The Me Too MovementShad FarasNo ratings yet
- Duane Brecheisen v. Eloy Mondragon, Warden And, Attorney General, State of New Mexico, 833 F.2d 238, 10th Cir. (1987)Document10 pagesDuane Brecheisen v. Eloy Mondragon, Warden And, Attorney General, State of New Mexico, 833 F.2d 238, 10th Cir. (1987)Scribd Government DocsNo ratings yet
- 1981 New York City Police Department Analysis of Police Combat SituationsDocument15 pages1981 New York City Police Department Analysis of Police Combat SituationsCostantino Isononami Dojo BrandozziNo ratings yet
- 1p40k - Apocalypse Rules v3.3.0Document1 page1p40k - Apocalypse Rules v3.3.0lynx147No ratings yet
- Battle of Gaugamela 4xxviiiDocument6 pagesBattle of Gaugamela 4xxviiiathozaNo ratings yet