
Chapter 85
Chapter 85
You might also like
- Smile Again CaseDocument28 pagesSmile Again CaseKeshav NautiyalNo ratings yet
- MCQs in DentistryDocument135 pagesMCQs in Dentistrysam4sl98% (85)
- Justice in Oral Health CareDocument371 pagesJustice in Oral Health CareSara Maria Menck SangiorgioNo ratings yet
- What Doctors Dont Tell You - The Dental HandbookDocument124 pagesWhat Doctors Dont Tell You - The Dental HandbookSeeTohKevin100% (1)
- Brushing and Flossing The Teeth of Conscious and Unconscious Client Procedure ChecklistDocument3 pagesBrushing and Flossing The Teeth of Conscious and Unconscious Client Procedure ChecklistMONIQUE GONZALESNo ratings yet
- Ubc ApplicationDocument3 pagesUbc Applicationapi-508959687No ratings yet
- Surgeon General'S Perspectives: Oral Health: The Silent EpidemicDocument2 pagesSurgeon General'S Perspectives: Oral Health: The Silent EpidemicArida BitanajshaNo ratings yet
- Should NHS Dentistry Be FreeDocument3 pagesShould NHS Dentistry Be FreePranav SivakumarNo ratings yet
- Oral Health in AmericaDocument332 pagesOral Health in AmericaAdrian GheorgheNo ratings yet
- Should NHS Dentistry Be FreeDocument3 pagesShould NHS Dentistry Be FreePranav SivakumarNo ratings yet
- Policy Healthcare ReformDocument3 pagesPolicy Healthcare Reformsonia_groff6256No ratings yet
- The Oral Health Information Suite (OHIS) : Its Use in The Management of Periodontal DiseaseDocument12 pagesThe Oral Health Information Suite (OHIS) : Its Use in The Management of Periodontal DiseasejemmysenseiNo ratings yet
- Women'S: A Literature Review OnDocument14 pagesWomen'S: A Literature Review OnAudrey Kristina MaypaNo ratings yet
- Should NHS Dentistry Be FreeDocument4 pagesShould NHS Dentistry Be FreePranav SivakumarNo ratings yet
- Nixon-Health Policy PaperDocument5 pagesNixon-Health Policy Paperapi-291204444No ratings yet
- Should NHS Dentistry Be FreeDocument4 pagesShould NHS Dentistry Be FreePranav SivakumarNo ratings yet
- Should NHS Dentistry Be FreeDocument4 pagesShould NHS Dentistry Be FreePranav SivakumarNo ratings yet
- Leake2008 PDFDocument9 pagesLeake2008 PDFjhon killNo ratings yet
- Klein1938 CPODDocument16 pagesKlein1938 CPODAlejandro RuizNo ratings yet
- Viewpoint Synthesis Final DraftDocument5 pagesViewpoint Synthesis Final Draftapi-589364430No ratings yet
- Boyce, 2021Document32 pagesBoyce, 2021Matheus Souza Campos CostaNo ratings yet
- Professional: Why Do We Need An Oral Health Care Policy in Canada?Document11 pagesProfessional: Why Do We Need An Oral Health Care Policy in Canada?petewin0123No ratings yet
- Senate Hearing, 113TH Congress - Dental Crisis in America: The Need To Address CostsDocument52 pagesSenate Hearing, 113TH Congress - Dental Crisis in America: The Need To Address CostsScribd Government DocsNo ratings yet
- Dental Evolving Medical Scene: Care in The CareDocument5 pagesDental Evolving Medical Scene: Care in The Carecarlina_the_bestNo ratings yet
- Thesis Statement On Universal Health CareDocument8 pagesThesis Statement On Universal Health Caretammylacyarlington100% (2)
- Intro To Biological DentistryDocument7 pagesIntro To Biological DentistryFelipe LazzarottoNo ratings yet
- Economics Health CareDocument79 pagesEconomics Health CareLuiz CarvalhoNo ratings yet
- Wahl 2006Document5 pagesWahl 2006anas dkaliNo ratings yet
- Dental Caries PandemicDocument5 pagesDental Caries PandemicKarla González GNo ratings yet
- Essay BlogDocument7 pagesEssay BlogWilliam W. LeeNo ratings yet
- Dental Implant Failure: A Clinical Guide to Prevention, Treatment, and Maintenance TherapyFrom EverandDental Implant Failure: A Clinical Guide to Prevention, Treatment, and Maintenance TherapyThomas G. Wilson Jr.No ratings yet
- Aids DissertationDocument5 pagesAids DissertationCustomPaperWritersUK100% (1)
- Alginate ImpressionDocument60 pagesAlginate ImpressionNugraha AnggaNo ratings yet
- Epidemiology of Oral Health Conditions in Older People: OriginalarticleDocument8 pagesEpidemiology of Oral Health Conditions in Older People: OriginalarticleWJNo ratings yet
- BMC Oral Health: Biotech and Biomaterials Research To Reduce The Caries EpidemicDocument7 pagesBMC Oral Health: Biotech and Biomaterials Research To Reduce The Caries EpidemicKranti PrajapatiNo ratings yet
- Oral Health Disparities Among The Elderly: Interdisciplinary Challenges For The FutureDocument10 pagesOral Health Disparities Among The Elderly: Interdisciplinary Challenges For The FutureJASPREETKAUR0410No ratings yet
- Periodicity DentalGuideDocument52 pagesPeriodicity DentalGuideSalam BataienehNo ratings yet
- State of DecayDocument8 pagesState of DecayWisdomToothOHANo ratings yet
- History of US Health Care System-Final ProjectDocument12 pagesHistory of US Health Care System-Final ProjectAntonio Abreu Jr.100% (1)
- Geriatric Oral Health Concerns A Dental Public Hea PDFDocument6 pagesGeriatric Oral Health Concerns A Dental Public Hea PDFفواز نميرNo ratings yet
- Akikut - Pride PaperDocument15 pagesAkikut - Pride Paperapi-486142180No ratings yet
- Planificacion en VIDocument16 pagesPlanificacion en VIGaby Tipan JNo ratings yet
- Health Care Crisis Thesis StatementDocument4 pagesHealth Care Crisis Thesis Statementsdeaqoikd100% (1)
- Dentistry in Post COVIDDocument3 pagesDentistry in Post COVIDsagrika groverNo ratings yet
- Intelligent Kindness: Reforming The Culture of HealthcareDocument7 pagesIntelligent Kindness: Reforming The Culture of Healthcarefarnaz_2647334No ratings yet
- Covid-19 Impact An Oral Health With A Focus On Temporomandibular Joint DisordersDocument5 pagesCovid-19 Impact An Oral Health With A Focus On Temporomandibular Joint Disordersbotak berjamaahNo ratings yet
- Final TintinDocument5 pagesFinal TintinRenier FloresNo ratings yet
- Universal Health Care Research PaperDocument5 pagesUniversal Health Care Research Paperwftvsutlg100% (1)
- Dental Amalgam and Mercury in Dentistry: Invited ReviewDocument11 pagesDental Amalgam and Mercury in Dentistry: Invited ReviewRichard Serrano Garcia OrtegaNo ratings yet
- Sage Publications, Inc., American Academy of Political and Social Science The Annals of The American Academy of Political and Social ScienceDocument9 pagesSage Publications, Inc., American Academy of Political and Social Science The Annals of The American Academy of Political and Social Scienceassaini carinta padangNo ratings yet
- Rough Draft Health Care 4Document10 pagesRough Draft Health Care 4long_paula1No ratings yet
- SJ BDJ 2008Document1 pageSJ BDJ 2008idurdNo ratings yet
- Letter To Mrs. Clinton-May 1993-By Trudy Attenberg-Face ForwardDocument2 pagesLetter To Mrs. Clinton-May 1993-By Trudy Attenberg-Face ForwardNeil GillespieNo ratings yet
- Managementofedentulous Patients: Damian J. Lee,, Paola C. SaponaroDocument13 pagesManagementofedentulous Patients: Damian J. Lee,, Paola C. Saponarosnehal jaiswalNo ratings yet
- The Young Professions Australia Roundtable 2003 Achieving A Sustainable Future A Dental PerspectiveDocument7 pagesThe Young Professions Australia Roundtable 2003 Achieving A Sustainable Future A Dental PerspectiveAhmed GendiaNo ratings yet
- ND Annual: Oral & Maxillofacial Pathology ReviewDocument12 pagesND Annual: Oral & Maxillofacial Pathology Reviewsulai701280No ratings yet
- Oral Diseases - 2023 - JainDocument7 pagesOral Diseases - 2023 - JainGita PratamaNo ratings yet
- IMPORTANTE Promoc Educac Salud Adult MayorDocument4 pagesIMPORTANTE Promoc Educac Salud Adult MayorJorge BalzanNo ratings yet
- Thesis Topics Public Health DentistryDocument5 pagesThesis Topics Public Health DentistryKristen Flores100% (2)
- Dental EducationDocument14 pagesDental EducationiwanntataNo ratings yet
- U O H S P 2016-2020: Topia RAL Ealth Urveillance LANDocument15 pagesU O H S P 2016-2020: Topia RAL Ealth Urveillance LANNoor Muddassir KhanNo ratings yet
- Gallium and Indium ScanDocument1 pageGallium and Indium ScanSri HariNo ratings yet
- 30 37Document8 pages30 37Sri HariNo ratings yet
- Lesson 1Document6 pagesLesson 1Sri HariNo ratings yet
- Chapter 2 Radionuclide ImagingDocument5 pagesChapter 2 Radionuclide ImagingSri HariNo ratings yet
- Management of Acute and Chronic Retention in MenDocument52 pagesManagement of Acute and Chronic Retention in MenSri HariNo ratings yet
- Usg in UrologyDocument25 pagesUsg in UrologySri HariNo ratings yet
- Renogram GuidelineDocument14 pagesRenogram GuidelineSri HariNo ratings yet
- Contrast Induced Nephropathy in Urology: Viji Samuel Thomson, Kumar Narayanan, J. Chandra SinghDocument9 pagesContrast Induced Nephropathy in Urology: Viji Samuel Thomson, Kumar Narayanan, J. Chandra SinghSri HariNo ratings yet
- Uro DynamicsDocument64 pagesUro DynamicsSri HariNo ratings yet
- Intraluminal Navigation Through Any Hollow Viscus Is PossibleDocument3 pagesIntraluminal Navigation Through Any Hollow Viscus Is PossibleSri HariNo ratings yet
- Uro Dynamics 1Document22 pagesUro Dynamics 1Sri HariNo ratings yet
- UroflowDocument41 pagesUroflowSri HariNo ratings yet
- Contrast Media: Dr.R.Abhiman Gautam, MCH Urology Prof - DR.RK Unit Stanley Medical CollegeDocument18 pagesContrast Media: Dr.R.Abhiman Gautam, MCH Urology Prof - DR.RK Unit Stanley Medical CollegeSri HariNo ratings yet
- Xray AbdomenDocument22 pagesXray AbdomenSri HariNo ratings yet
- Intravenous Radiographic Contrast Induced Adverse Reactions - Their Causes, Prevention and Relief MeasuresDocument7 pagesIntravenous Radiographic Contrast Induced Adverse Reactions - Their Causes, Prevention and Relief MeasuresSri HariNo ratings yet
- CT Angiography in UrologyDocument2 pagesCT Angiography in UrologySri HariNo ratings yet
- Contrast Induced NephropathyDocument2 pagesContrast Induced NephropathySri HariNo ratings yet
- Contrast Arteriography: Reasons Not As A Preliminary Screening ToolDocument3 pagesContrast Arteriography: Reasons Not As A Preliminary Screening ToolSri HariNo ratings yet
- Contrast Induced Nephropathy in Urology: Viji Samuel Thomson, Kumar Narayanan, J. Chandra SinghDocument9 pagesContrast Induced Nephropathy in Urology: Viji Samuel Thomson, Kumar Narayanan, J. Chandra SinghSri HariNo ratings yet
- Rajiv Gandhi University of Health Sciences, Bangalore, Karnataka. Performa For Registration of Subject For DissertationDocument21 pagesRajiv Gandhi University of Health Sciences, Bangalore, Karnataka. Performa For Registration of Subject For DissertationSri HariNo ratings yet
- Clean Intermittent Catheterization (CIC) : IndicationsDocument2 pagesClean Intermittent Catheterization (CIC) : IndicationsSri HariNo ratings yet
- Impact of Endometrial Preparation Protocols For Frozen Embryo Transfer On Live Birth RatesDocument8 pagesImpact of Endometrial Preparation Protocols For Frozen Embryo Transfer On Live Birth RatesSri HariNo ratings yet
- Captopril Renography: Physiologic Principle - Loss of Preferential Vasoconstriction of The EfferentDocument3 pagesCaptopril Renography: Physiologic Principle - Loss of Preferential Vasoconstriction of The EfferentSri HariNo ratings yet
- European Journal of Obstetrics & Gynecology and Reproductive BiologyDocument5 pagesEuropean Journal of Obstetrics & Gynecology and Reproductive BiologySri HariNo ratings yet
- Mccormick: Michael J. CoughlinDocument1 pageMccormick: Michael J. CoughlinSri HariNo ratings yet
- Access SheathDocument22 pagesAccess SheathSri HariNo ratings yet
- Maternal Mortality: Liliana Carvajal Vibeke Oestreich Nielsen Armando H. SeucDocument38 pagesMaternal Mortality: Liliana Carvajal Vibeke Oestreich Nielsen Armando H. SeucSri HariNo ratings yet
- 03 A025 5123Document13 pages03 A025 5123Sri HariNo ratings yet
- History of Articulators Part 1 2004Document13 pagesHistory of Articulators Part 1 2004ayduggal100% (4)
- Biomimetic AllemanDocument6 pagesBiomimetic AllemanAlireza RaieNo ratings yet
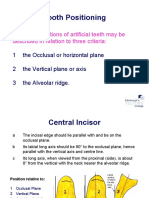
- Tooth Positioning: The Basic Positions of Artificial Teeth May Be Described in Relation To Three CriteriaDocument19 pagesTooth Positioning: The Basic Positions of Artificial Teeth May Be Described in Relation To Three CriteriaCherine SnookNo ratings yet
- Ahead FPD QuesDocument11 pagesAhead FPD QuesMostafa FayadNo ratings yet
- Cephalometric Distintion of Class II Division 2Document8 pagesCephalometric Distintion of Class II Division 2Diego SolaqueNo ratings yet
- KariesDocument4 pagesKariesSherlocknovNo ratings yet
- Oral Hygiene InstructionsDocument2 pagesOral Hygiene Instructionstepokpantat100% (1)
- Malkinson Et Al. 2012Document15 pagesMalkinson Et Al. 2012Nawaf RuwailiNo ratings yet
- Kep NursewndDocument18 pagesKep NursewndUntung Edi SaputraNo ratings yet
- SPSC 2018 Paper Type ADocument8 pagesSPSC 2018 Paper Type AMeenaNo ratings yet
- BIO C Repair With For Horizontal Root Fracture PDFDocument5 pagesBIO C Repair With For Horizontal Root Fracture PDFDaniel Vivas0% (1)
- Cementoblastoma and Periapical Cemento-Osseous DysplasiaDocument15 pagesCementoblastoma and Periapical Cemento-Osseous DysplasiaHessa AloliwiNo ratings yet
- Prost Ho Don TicsDocument172 pagesProst Ho Don Ticsسماح صلاحNo ratings yet
- Smile Arc Protection Part 2Document4 pagesSmile Arc Protection Part 2M.Laura100% (1)
- Annual Review of Selected ScientificDocument50 pagesAnnual Review of Selected Scientificpasber26No ratings yet
- Stability and RetentionDocument8 pagesStability and RetentionlizetNo ratings yet
- CHN Compre Exm 1Document8 pagesCHN Compre Exm 1Roy Salvador100% (1)
- Gingival Biotype Classification, Assessment, and Clinical Importance: A ReviewDocument7 pagesGingival Biotype Classification, Assessment, and Clinical Importance: A ReviewKetherin LeeNo ratings yet
- Davidovitch1995 PDFDocument6 pagesDavidovitch1995 PDFRahulLife'sNo ratings yet
- Dental Clinic (Job Description)Document10 pagesDental Clinic (Job Description)A'ihNo ratings yet
- Friday June 18, 2010 LeaderDocument47 pagesFriday June 18, 2010 LeaderSurrey/North Delta LeaderNo ratings yet
- Test - 10 Root (Radicular) CystsDocument5 pagesTest - 10 Root (Radicular) CystsIsak ShatikaNo ratings yet
- Project Practicum PresentationDocument37 pagesProject Practicum Presentationapi-652480224No ratings yet
- Oral Hygiene Instruction Presentation Danielle WilsonDocument15 pagesOral Hygiene Instruction Presentation Danielle Wilsonapi-348271404No ratings yet
- Texas Medicaid and CHIP Provider FAQsDocument4 pagesTexas Medicaid and CHIP Provider FAQsangelina smithNo ratings yet
- Guide To BolognaDocument48 pagesGuide To Bolognamiry89No ratings yet




















































































































Download as pdf or txt
You might also like
- Smile Again CaseDocument28 pagesSmile Again CaseKeshav NautiyalNo ratings yet
- MCQs in DentistryDocument135 pagesMCQs in Dentistrysam4sl98% (85)
- Justice in Oral Health CareDocument371 pagesJustice in Oral Health CareSara Maria Menck SangiorgioNo ratings yet
- What Doctors Dont Tell You - The Dental HandbookDocument124 pagesWhat Doctors Dont Tell You - The Dental HandbookSeeTohKevin100% (1)
- Brushing and Flossing The Teeth of Conscious and Unconscious Client Procedure ChecklistDocument3 pagesBrushing and Flossing The Teeth of Conscious and Unconscious Client Procedure ChecklistMONIQUE GONZALESNo ratings yet
- Ubc ApplicationDocument3 pagesUbc Applicationapi-508959687No ratings yet
- Surgeon General'S Perspectives: Oral Health: The Silent EpidemicDocument2 pagesSurgeon General'S Perspectives: Oral Health: The Silent EpidemicArida BitanajshaNo ratings yet
- Should NHS Dentistry Be FreeDocument3 pagesShould NHS Dentistry Be FreePranav SivakumarNo ratings yet
- Oral Health in AmericaDocument332 pagesOral Health in AmericaAdrian GheorgheNo ratings yet
- Should NHS Dentistry Be FreeDocument3 pagesShould NHS Dentistry Be FreePranav SivakumarNo ratings yet
- Policy Healthcare ReformDocument3 pagesPolicy Healthcare Reformsonia_groff6256No ratings yet
- The Oral Health Information Suite (OHIS) : Its Use in The Management of Periodontal DiseaseDocument12 pagesThe Oral Health Information Suite (OHIS) : Its Use in The Management of Periodontal DiseasejemmysenseiNo ratings yet
- Women'S: A Literature Review OnDocument14 pagesWomen'S: A Literature Review OnAudrey Kristina MaypaNo ratings yet
- Should NHS Dentistry Be FreeDocument4 pagesShould NHS Dentistry Be FreePranav SivakumarNo ratings yet
- Nixon-Health Policy PaperDocument5 pagesNixon-Health Policy Paperapi-291204444No ratings yet
- Should NHS Dentistry Be FreeDocument4 pagesShould NHS Dentistry Be FreePranav SivakumarNo ratings yet
- Should NHS Dentistry Be FreeDocument4 pagesShould NHS Dentistry Be FreePranav SivakumarNo ratings yet
- Leake2008 PDFDocument9 pagesLeake2008 PDFjhon killNo ratings yet
- Klein1938 CPODDocument16 pagesKlein1938 CPODAlejandro RuizNo ratings yet
- Viewpoint Synthesis Final DraftDocument5 pagesViewpoint Synthesis Final Draftapi-589364430No ratings yet
- Boyce, 2021Document32 pagesBoyce, 2021Matheus Souza Campos CostaNo ratings yet
- Professional: Why Do We Need An Oral Health Care Policy in Canada?Document11 pagesProfessional: Why Do We Need An Oral Health Care Policy in Canada?petewin0123No ratings yet
- Senate Hearing, 113TH Congress - Dental Crisis in America: The Need To Address CostsDocument52 pagesSenate Hearing, 113TH Congress - Dental Crisis in America: The Need To Address CostsScribd Government DocsNo ratings yet
- Dental Evolving Medical Scene: Care in The CareDocument5 pagesDental Evolving Medical Scene: Care in The Carecarlina_the_bestNo ratings yet
- Thesis Statement On Universal Health CareDocument8 pagesThesis Statement On Universal Health Caretammylacyarlington100% (2)
- Intro To Biological DentistryDocument7 pagesIntro To Biological DentistryFelipe LazzarottoNo ratings yet
- Economics Health CareDocument79 pagesEconomics Health CareLuiz CarvalhoNo ratings yet
- Wahl 2006Document5 pagesWahl 2006anas dkaliNo ratings yet
- Dental Caries PandemicDocument5 pagesDental Caries PandemicKarla González GNo ratings yet
- Essay BlogDocument7 pagesEssay BlogWilliam W. LeeNo ratings yet
- Dental Implant Failure: A Clinical Guide to Prevention, Treatment, and Maintenance TherapyFrom EverandDental Implant Failure: A Clinical Guide to Prevention, Treatment, and Maintenance TherapyThomas G. Wilson Jr.No ratings yet
- Aids DissertationDocument5 pagesAids DissertationCustomPaperWritersUK100% (1)
- Alginate ImpressionDocument60 pagesAlginate ImpressionNugraha AnggaNo ratings yet
- Epidemiology of Oral Health Conditions in Older People: OriginalarticleDocument8 pagesEpidemiology of Oral Health Conditions in Older People: OriginalarticleWJNo ratings yet
- BMC Oral Health: Biotech and Biomaterials Research To Reduce The Caries EpidemicDocument7 pagesBMC Oral Health: Biotech and Biomaterials Research To Reduce The Caries EpidemicKranti PrajapatiNo ratings yet
- Oral Health Disparities Among The Elderly: Interdisciplinary Challenges For The FutureDocument10 pagesOral Health Disparities Among The Elderly: Interdisciplinary Challenges For The FutureJASPREETKAUR0410No ratings yet
- Periodicity DentalGuideDocument52 pagesPeriodicity DentalGuideSalam BataienehNo ratings yet
- State of DecayDocument8 pagesState of DecayWisdomToothOHANo ratings yet
- History of US Health Care System-Final ProjectDocument12 pagesHistory of US Health Care System-Final ProjectAntonio Abreu Jr.100% (1)
- Geriatric Oral Health Concerns A Dental Public Hea PDFDocument6 pagesGeriatric Oral Health Concerns A Dental Public Hea PDFفواز نميرNo ratings yet
- Akikut - Pride PaperDocument15 pagesAkikut - Pride Paperapi-486142180No ratings yet
- Planificacion en VIDocument16 pagesPlanificacion en VIGaby Tipan JNo ratings yet
- Health Care Crisis Thesis StatementDocument4 pagesHealth Care Crisis Thesis Statementsdeaqoikd100% (1)
- Dentistry in Post COVIDDocument3 pagesDentistry in Post COVIDsagrika groverNo ratings yet
- Intelligent Kindness: Reforming The Culture of HealthcareDocument7 pagesIntelligent Kindness: Reforming The Culture of Healthcarefarnaz_2647334No ratings yet
- Covid-19 Impact An Oral Health With A Focus On Temporomandibular Joint DisordersDocument5 pagesCovid-19 Impact An Oral Health With A Focus On Temporomandibular Joint Disordersbotak berjamaahNo ratings yet
- Final TintinDocument5 pagesFinal TintinRenier FloresNo ratings yet
- Universal Health Care Research PaperDocument5 pagesUniversal Health Care Research Paperwftvsutlg100% (1)
- Dental Amalgam and Mercury in Dentistry: Invited ReviewDocument11 pagesDental Amalgam and Mercury in Dentistry: Invited ReviewRichard Serrano Garcia OrtegaNo ratings yet
- Sage Publications, Inc., American Academy of Political and Social Science The Annals of The American Academy of Political and Social ScienceDocument9 pagesSage Publications, Inc., American Academy of Political and Social Science The Annals of The American Academy of Political and Social Scienceassaini carinta padangNo ratings yet
- Rough Draft Health Care 4Document10 pagesRough Draft Health Care 4long_paula1No ratings yet
- SJ BDJ 2008Document1 pageSJ BDJ 2008idurdNo ratings yet
- Letter To Mrs. Clinton-May 1993-By Trudy Attenberg-Face ForwardDocument2 pagesLetter To Mrs. Clinton-May 1993-By Trudy Attenberg-Face ForwardNeil GillespieNo ratings yet
- Managementofedentulous Patients: Damian J. Lee,, Paola C. SaponaroDocument13 pagesManagementofedentulous Patients: Damian J. Lee,, Paola C. Saponarosnehal jaiswalNo ratings yet
- The Young Professions Australia Roundtable 2003 Achieving A Sustainable Future A Dental PerspectiveDocument7 pagesThe Young Professions Australia Roundtable 2003 Achieving A Sustainable Future A Dental PerspectiveAhmed GendiaNo ratings yet
- ND Annual: Oral & Maxillofacial Pathology ReviewDocument12 pagesND Annual: Oral & Maxillofacial Pathology Reviewsulai701280No ratings yet
- Oral Diseases - 2023 - JainDocument7 pagesOral Diseases - 2023 - JainGita PratamaNo ratings yet
- IMPORTANTE Promoc Educac Salud Adult MayorDocument4 pagesIMPORTANTE Promoc Educac Salud Adult MayorJorge BalzanNo ratings yet
- Thesis Topics Public Health DentistryDocument5 pagesThesis Topics Public Health DentistryKristen Flores100% (2)
- Dental EducationDocument14 pagesDental EducationiwanntataNo ratings yet
- U O H S P 2016-2020: Topia RAL Ealth Urveillance LANDocument15 pagesU O H S P 2016-2020: Topia RAL Ealth Urveillance LANNoor Muddassir KhanNo ratings yet
- Gallium and Indium ScanDocument1 pageGallium and Indium ScanSri HariNo ratings yet
- 30 37Document8 pages30 37Sri HariNo ratings yet
- Lesson 1Document6 pagesLesson 1Sri HariNo ratings yet
- Chapter 2 Radionuclide ImagingDocument5 pagesChapter 2 Radionuclide ImagingSri HariNo ratings yet
- Management of Acute and Chronic Retention in MenDocument52 pagesManagement of Acute and Chronic Retention in MenSri HariNo ratings yet
- Usg in UrologyDocument25 pagesUsg in UrologySri HariNo ratings yet
- Renogram GuidelineDocument14 pagesRenogram GuidelineSri HariNo ratings yet
- Contrast Induced Nephropathy in Urology: Viji Samuel Thomson, Kumar Narayanan, J. Chandra SinghDocument9 pagesContrast Induced Nephropathy in Urology: Viji Samuel Thomson, Kumar Narayanan, J. Chandra SinghSri HariNo ratings yet
- Uro DynamicsDocument64 pagesUro DynamicsSri HariNo ratings yet
- Intraluminal Navigation Through Any Hollow Viscus Is PossibleDocument3 pagesIntraluminal Navigation Through Any Hollow Viscus Is PossibleSri HariNo ratings yet
- Uro Dynamics 1Document22 pagesUro Dynamics 1Sri HariNo ratings yet
- UroflowDocument41 pagesUroflowSri HariNo ratings yet
- Contrast Media: Dr.R.Abhiman Gautam, MCH Urology Prof - DR.RK Unit Stanley Medical CollegeDocument18 pagesContrast Media: Dr.R.Abhiman Gautam, MCH Urology Prof - DR.RK Unit Stanley Medical CollegeSri HariNo ratings yet
- Xray AbdomenDocument22 pagesXray AbdomenSri HariNo ratings yet
- Intravenous Radiographic Contrast Induced Adverse Reactions - Their Causes, Prevention and Relief MeasuresDocument7 pagesIntravenous Radiographic Contrast Induced Adverse Reactions - Their Causes, Prevention and Relief MeasuresSri HariNo ratings yet
- CT Angiography in UrologyDocument2 pagesCT Angiography in UrologySri HariNo ratings yet
- Contrast Induced NephropathyDocument2 pagesContrast Induced NephropathySri HariNo ratings yet
- Contrast Arteriography: Reasons Not As A Preliminary Screening ToolDocument3 pagesContrast Arteriography: Reasons Not As A Preliminary Screening ToolSri HariNo ratings yet
- Contrast Induced Nephropathy in Urology: Viji Samuel Thomson, Kumar Narayanan, J. Chandra SinghDocument9 pagesContrast Induced Nephropathy in Urology: Viji Samuel Thomson, Kumar Narayanan, J. Chandra SinghSri HariNo ratings yet
- Rajiv Gandhi University of Health Sciences, Bangalore, Karnataka. Performa For Registration of Subject For DissertationDocument21 pagesRajiv Gandhi University of Health Sciences, Bangalore, Karnataka. Performa For Registration of Subject For DissertationSri HariNo ratings yet
- Clean Intermittent Catheterization (CIC) : IndicationsDocument2 pagesClean Intermittent Catheterization (CIC) : IndicationsSri HariNo ratings yet
- Impact of Endometrial Preparation Protocols For Frozen Embryo Transfer On Live Birth RatesDocument8 pagesImpact of Endometrial Preparation Protocols For Frozen Embryo Transfer On Live Birth RatesSri HariNo ratings yet
- Captopril Renography: Physiologic Principle - Loss of Preferential Vasoconstriction of The EfferentDocument3 pagesCaptopril Renography: Physiologic Principle - Loss of Preferential Vasoconstriction of The EfferentSri HariNo ratings yet
- European Journal of Obstetrics & Gynecology and Reproductive BiologyDocument5 pagesEuropean Journal of Obstetrics & Gynecology and Reproductive BiologySri HariNo ratings yet
- Mccormick: Michael J. CoughlinDocument1 pageMccormick: Michael J. CoughlinSri HariNo ratings yet
- Access SheathDocument22 pagesAccess SheathSri HariNo ratings yet
- Maternal Mortality: Liliana Carvajal Vibeke Oestreich Nielsen Armando H. SeucDocument38 pagesMaternal Mortality: Liliana Carvajal Vibeke Oestreich Nielsen Armando H. SeucSri HariNo ratings yet
- 03 A025 5123Document13 pages03 A025 5123Sri HariNo ratings yet
- History of Articulators Part 1 2004Document13 pagesHistory of Articulators Part 1 2004ayduggal100% (4)
- Biomimetic AllemanDocument6 pagesBiomimetic AllemanAlireza RaieNo ratings yet
- Tooth Positioning: The Basic Positions of Artificial Teeth May Be Described in Relation To Three CriteriaDocument19 pagesTooth Positioning: The Basic Positions of Artificial Teeth May Be Described in Relation To Three CriteriaCherine SnookNo ratings yet
- Ahead FPD QuesDocument11 pagesAhead FPD QuesMostafa FayadNo ratings yet
- Cephalometric Distintion of Class II Division 2Document8 pagesCephalometric Distintion of Class II Division 2Diego SolaqueNo ratings yet
- KariesDocument4 pagesKariesSherlocknovNo ratings yet
- Oral Hygiene InstructionsDocument2 pagesOral Hygiene Instructionstepokpantat100% (1)
- Malkinson Et Al. 2012Document15 pagesMalkinson Et Al. 2012Nawaf RuwailiNo ratings yet
- Kep NursewndDocument18 pagesKep NursewndUntung Edi SaputraNo ratings yet
- SPSC 2018 Paper Type ADocument8 pagesSPSC 2018 Paper Type AMeenaNo ratings yet
- BIO C Repair With For Horizontal Root Fracture PDFDocument5 pagesBIO C Repair With For Horizontal Root Fracture PDFDaniel Vivas0% (1)
- Cementoblastoma and Periapical Cemento-Osseous DysplasiaDocument15 pagesCementoblastoma and Periapical Cemento-Osseous DysplasiaHessa AloliwiNo ratings yet
- Prost Ho Don TicsDocument172 pagesProst Ho Don Ticsسماح صلاحNo ratings yet
- Smile Arc Protection Part 2Document4 pagesSmile Arc Protection Part 2M.Laura100% (1)
- Annual Review of Selected ScientificDocument50 pagesAnnual Review of Selected Scientificpasber26No ratings yet
- Stability and RetentionDocument8 pagesStability and RetentionlizetNo ratings yet
- CHN Compre Exm 1Document8 pagesCHN Compre Exm 1Roy Salvador100% (1)
- Gingival Biotype Classification, Assessment, and Clinical Importance: A ReviewDocument7 pagesGingival Biotype Classification, Assessment, and Clinical Importance: A ReviewKetherin LeeNo ratings yet
- Davidovitch1995 PDFDocument6 pagesDavidovitch1995 PDFRahulLife'sNo ratings yet
- Dental Clinic (Job Description)Document10 pagesDental Clinic (Job Description)A'ihNo ratings yet
- Friday June 18, 2010 LeaderDocument47 pagesFriday June 18, 2010 LeaderSurrey/North Delta LeaderNo ratings yet
- Test - 10 Root (Radicular) CystsDocument5 pagesTest - 10 Root (Radicular) CystsIsak ShatikaNo ratings yet
- Project Practicum PresentationDocument37 pagesProject Practicum Presentationapi-652480224No ratings yet
- Oral Hygiene Instruction Presentation Danielle WilsonDocument15 pagesOral Hygiene Instruction Presentation Danielle Wilsonapi-348271404No ratings yet
- Texas Medicaid and CHIP Provider FAQsDocument4 pagesTexas Medicaid and CHIP Provider FAQsangelina smithNo ratings yet
- Guide To BolognaDocument48 pagesGuide To Bolognamiry89No ratings yet