Download as pdf or txt
You might also like
- Sail Ipd FormDocument2 pagesSail Ipd Formshami73% (11)
- Revised MOADocument3 pagesRevised MOATimothy John Banaira Talusan100% (1)
- Justice Lodha Committee Report On IPLDocument59 pagesJustice Lodha Committee Report On IPLLatest Laws TeamNo ratings yet
- Controlling Sex and Decency in Advertising Around The WorldDocument12 pagesControlling Sex and Decency in Advertising Around The WorldShwetha ShekharNo ratings yet
- UIICHdfc ClaimformDocument2 pagesUIICHdfc ClaimformdomyomglolNo ratings yet
- United India Insurance Co. LTD.,: Mediclaim Insurance Policy Reimbursement Claim FormDocument2 pagesUnited India Insurance Co. LTD.,: Mediclaim Insurance Policy Reimbursement Claim Form'Θκ'βύτ-Ίισνέγσύ.No ratings yet
- OIC Claim FormDocument4 pagesOIC Claim FormPrashant SinghNo ratings yet
- National Insurance Company LimitedDocument4 pagesNational Insurance Company Limitedkaransandesara777No ratings yet
- New GHPL Claim Form PDFDocument3 pagesNew GHPL Claim Form PDFp_srib4uNo ratings yet
- Claim FormDocument3 pagesClaim FormSumit ManglaniNo ratings yet
- Claim Form: (For Reimbursement of Expenses)Document4 pagesClaim Form: (For Reimbursement of Expenses)Shankar NathNo ratings yet
- WISE CF W - Instructions 120216Document4 pagesWISE CF W - Instructions 120216Jotaro KujooNo ratings yet
- Health Total Claim FormDocument2 pagesHealth Total Claim Formpavan reddyNo ratings yet
- GHPL Claim FormDocument2 pagesGHPL Claim FormadddataNo ratings yet
- Pacific MMI Claim Form PDFDocument3 pagesPacific MMI Claim Form PDFKaitaMahn100% (1)
- National Inurance Company Limited - Claim FormDocument3 pagesNational Inurance Company Limited - Claim FormfuckyouprettyNo ratings yet
- PH IcformDocument4 pagesPH IcformHihiNo ratings yet
- GMC Claim Form How To File A ClaimDocument4 pagesGMC Claim Form How To File A ClaimtweetknotNo ratings yet
- Personal Accident Claim FormDocument5 pagesPersonal Accident Claim FormMadhava Reddy MunagalaNo ratings yet
- Claim FormDocument3 pagesClaim FormKhameer L Shah100% (1)
- NiramayaclaimformDocument2 pagesNiramayaclaimformu409023No ratings yet
- The Oriental Insurance Company Limited (Incorporated in India, Subsidiary of General Insurance Corporation of India)Document4 pagesThe Oriental Insurance Company Limited (Incorporated in India, Subsidiary of General Insurance Corporation of India)Mcnet WideNo ratings yet
- AXA Reimbursement Form ALL enDocument2 pagesAXA Reimbursement Form ALL enReynard Delos SantosNo ratings yet
- Claims Form For New India AssuranceDocument2 pagesClaims Form For New India AssuranceRafael BlackNo ratings yet
- Extended Health Benefits Claim FormDocument2 pagesExtended Health Benefits Claim FormHolystreamNo ratings yet
- Axa Claim FormDocument2 pagesAxa Claim FormReem Mohamed El BarraniNo ratings yet
- Application For Membership Form: Application No.: Effectivity Date: Contract No.Document2 pagesApplication For Membership Form: Application No.: Effectivity Date: Contract No.Lizeth QuerubinNo ratings yet
- Head Office: 87, M G Road, Fort, Mumbai-400001: I. II - CLAIM NO.Document5 pagesHead Office: 87, M G Road, Fort, Mumbai-400001: I. II - CLAIM NO.gaddipati_ramuNo ratings yet
- Claim Form - Part A: United India Insurance Company Limited Registered & Head Office: 24, Whites Road, Chennai-600014Document4 pagesClaim Form - Part A: United India Insurance Company Limited Registered & Head Office: 24, Whites Road, Chennai-600014Boby GanaNo ratings yet
- AXA Reimbursement Claim FormDocument2 pagesAXA Reimbursement Claim Formrajkamal eshwarNo ratings yet
- NAIC Claim Form PDFDocument3 pagesNAIC Claim Form PDFMohit BaggaNo ratings yet
- 1 Claim FormDocument36 pages1 Claim Formkarmayukh1No ratings yet
- GP Mediclaim-Claim NewwerDocument3 pagesGP Mediclaim-Claim Newwervatsalshah24No ratings yet
- Axa Reimbursement Claim Form 01Document2 pagesAxa Reimbursement Claim Form 01Tarak FakhfakhNo ratings yet
- Claimant Statement With ETF Mandate FormDocument6 pagesClaimant Statement With ETF Mandate FormKishan GarhtiyaNo ratings yet
- Tata AIA Life Insurance Company Limited: Total & Permanent Disability Claim FormDocument2 pagesTata AIA Life Insurance Company Limited: Total & Permanent Disability Claim FormPrashob SugathanNo ratings yet
- Student Application FormDocument6 pagesStudent Application FormelletjiesNo ratings yet
- Medical Claim Reimbursement Form EnglishDocument2 pagesMedical Claim Reimbursement Form EnglishHananAhmedNo ratings yet
- Claim Form NewDocument4 pagesClaim Form NewVicky GautamNo ratings yet
- NTUC Claim FormDocument5 pagesNTUC Claim FormHihiNo ratings yet
- AXA Non Death Claim FormDocument4 pagesAXA Non Death Claim FormKenji ChinNo ratings yet
- 10 New India Assurance Company - Reimbursement Claim FormDocument3 pages10 New India Assurance Company - Reimbursement Claim FormbhurajeshNo ratings yet
- Sicom Claim FormDocument1 pageSicom Claim FormAshvin Chukun100% (2)
- Bajaj Allianz General Insurance Company Limited: Claim Form - Domiciliary and OpdDocument2 pagesBajaj Allianz General Insurance Company Limited: Claim Form - Domiciliary and OpdvkbasavaNo ratings yet
- Crewsure Claim Form (XLCatlin) 1.3Document2 pagesCrewsure Claim Form (XLCatlin) 1.3Andrei Belehuzi0% (1)
- Health CLAIM FORM PDFDocument2 pagesHealth CLAIM FORM PDFstarlingmediaNo ratings yet
- Claim Form For Out of Canada H.S.M. Expense Benefit: Section 1 - Must Be Completed by The Provider of ServiceDocument1 pageClaim Form For Out of Canada H.S.M. Expense Benefit: Section 1 - Must Be Completed by The Provider of Servicemichel_adam1701No ratings yet
- Kutumb Swasthya Bima Policy - GroupDocument4 pagesKutumb Swasthya Bima Policy - Grouprohit kakkarNo ratings yet
- Claim Form - IPDDocument2 pagesClaim Form - IPDEswar Kiran ReddyNo ratings yet
- Annexure For Advance PymtDocument3 pagesAnnexure For Advance PymtrenupnbeNo ratings yet
- Portability Form Annexure 31-01-2012Document3 pagesPortability Form Annexure 31-01-2012irshadgraymanNo ratings yet
- Proposal Form Ashakiran PDFDocument6 pagesProposal Form Ashakiran PDFSreejith Rajendran PillaiNo ratings yet
- CLAIMS REIMBURSEMENT FORM EditedDocument1 pageCLAIMS REIMBURSEMENT FORM EditedOliver SyNo ratings yet
- JF Elite Plus Student Insurance Claim Form: ImportantDocument2 pagesJF Elite Plus Student Insurance Claim Form: ImportantJayesh GoplaniNo ratings yet
- Oman New Reimbursement Claim FormDocument3 pagesOman New Reimbursement Claim Formtoalok4723No ratings yet
- Form 300Document8 pagesForm 300Sachin SharmaNo ratings yet
- BCBSTX Halliburton Intl Claim FormDocument2 pagesBCBSTX Halliburton Intl Claim FormLoganBohannonNo ratings yet
- SI Increase - Health Proposal FormDocument3 pagesSI Increase - Health Proposal FormbjitudNo ratings yet
- ESIS Claims PO Box 6562 Scranton, PA 18505-6562 +1 913-748-8894 Tel +1 844 890-6967 FaxDocument3 pagesESIS Claims PO Box 6562 Scranton, PA 18505-6562 +1 913-748-8894 Tel +1 844 890-6967 FaxFrank PascarellaNo ratings yet
- Hospitalisation Claim FormsDocument6 pagesHospitalisation Claim FormspritamNo ratings yet
- Newman's Billing and Coding Technicians Study GuideFrom EverandNewman's Billing and Coding Technicians Study GuideRating: 4.5 out of 5 stars4.5/5 (2)
- Caterino v. Barry, 1st Cir. (1993)Document37 pagesCaterino v. Barry, 1st Cir. (1993)Scribd Government DocsNo ratings yet
- LEA 2 Competency 1Document5 pagesLEA 2 Competency 1Kristel AnnNo ratings yet
- Filed: Patrick FisherDocument30 pagesFiled: Patrick FisherScribd Government DocsNo ratings yet
- Landbank vs. AlsuaDocument6 pagesLandbank vs. AlsuaJames Ibrahim Alih100% (1)
- Christmas Party Permission FormDocument2 pagesChristmas Party Permission FormIL Aguilar0% (1)
- Gàidhealtachd Act 2017Document2 pagesGàidhealtachd Act 2017msp-archiveNo ratings yet
- Special Crime InvestigationDocument11 pagesSpecial Crime InvestigationHurtley galidayNo ratings yet
- Professional Services Agreement Sample 3Document7 pagesProfessional Services Agreement Sample 3Vj DelatadoNo ratings yet
- The Historical Development of Islamic LawDocument17 pagesThe Historical Development of Islamic LawPalak Rawat100% (1)
- Comm120 DIGESTDocument1 pageComm120 DIGESTCorinne CatibayanNo ratings yet
- PTECDocument2 pagesPTECabdulbeg1986No ratings yet
- 2020-07-31 Newsweek InternationalDocument54 pages2020-07-31 Newsweek InternationalMaria GrecuNo ratings yet
- Habana Vs RoblesDocument2 pagesHabana Vs RoblesRex Traya100% (1)
- Complaint: Plaintiff, Through The Undersigned Counsel, Unto This Honorable Court, Hereby Respectfully Avers ThatDocument6 pagesComplaint: Plaintiff, Through The Undersigned Counsel, Unto This Honorable Court, Hereby Respectfully Avers ThatRoan HabocNo ratings yet
- People Vs GaffudDocument2 pagesPeople Vs GaffudIan MarcoNo ratings yet
- Crim Pro Add'l Case DigestsDocument6 pagesCrim Pro Add'l Case DigestsAlicia Jane NavarroNo ratings yet
- Cover Form 137.Document10 pagesCover Form 137.rosnic25No ratings yet
- Codes of Practice - 6Document4 pagesCodes of Practice - 6Muhammad sajjadNo ratings yet
- Identity Theft Red Flags Rule TemplateDocument15 pagesIdentity Theft Red Flags Rule TemplateDarshit ThakkarNo ratings yet
- SM Line Bill of Lading Terms and Conditions SM Line Bill of LadingDocument3 pagesSM Line Bill of Lading Terms and Conditions SM Line Bill of LadingDung LeNo ratings yet
- Alyeasha Residential PermitDocument1 pageAlyeasha Residential PermitiyayofficialNo ratings yet
- CLJ ExamDocument53 pagesCLJ ExamJeselyn Malaluan100% (1)
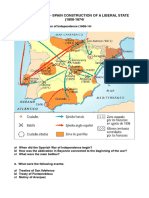
- Questionnaire Spain - Construction of A Liberal StateDocument3 pagesQuestionnaire Spain - Construction of A Liberal StateSAUL SILVANo ratings yet
- Parliamentary Vs Presidential - (Pakistan’ S Domestic Affairs) PDFDocument4 pagesParliamentary Vs Presidential - (Pakistan’ S Domestic Affairs) PDFmeerhamzaNo ratings yet
- Verified Motion For Reconsideration: NLRC LAC NO. 07-002695-19 RAB CASE NO. RAB IV 7-01352-18-CDocument8 pagesVerified Motion For Reconsideration: NLRC LAC NO. 07-002695-19 RAB CASE NO. RAB IV 7-01352-18-CPau JoyosaNo ratings yet
- Imm5621gen052022 2-104a8pdeDocument2 pagesImm5621gen052022 2-104a8pderajesh kumarNo ratings yet
- Rovenstine Press ReleaseDocument2 pagesRovenstine Press ReleaseWSBT 22No ratings yet