Download as docx, pdf, or txt
You might also like
- Neurokinesthetic Approach To Hand Function and HandwritingDocument84 pagesNeurokinesthetic Approach To Hand Function and HandwritingMichelle Huet100% (2)
- Primitive Reflexes Development OolsDocument19 pagesPrimitive Reflexes Development OolsMaRiaNo ratings yet
- Motor Coordination in Young Children (Charlop-Atwell Scale)Document6 pagesMotor Coordination in Young Children (Charlop-Atwell Scale)Andreia Santos100% (2)
- Phases of Language DevelopmentDocument2 pagesPhases of Language DevelopmentPallaviKulshresthaNo ratings yet
- Uniform Terminology AOTA PDFDocument8 pagesUniform Terminology AOTA PDFLaura GuevaraNo ratings yet
- NDT by Dr. Rati.Document13 pagesNDT by Dr. Rati.Anup PednekarNo ratings yet
- Bobath Approach: Neuro-Developmental TechniquesDocument25 pagesBobath Approach: Neuro-Developmental TechniquesJAZA RIZVI100% (1)
- Process of Motor DevelopmentDocument33 pagesProcess of Motor Developmentmohitnet1327No ratings yet
- Reflex Testing Methods For Evaluating CNS DevelopmentDocument80 pagesReflex Testing Methods For Evaluating CNS DevelopmentTaufik100% (5)
- The Effects of Tactile Defensiveness and Tactile Discrimination On In-Hand ManipulationDocument8 pagesThe Effects of Tactile Defensiveness and Tactile Discrimination On In-Hand ManipulationNuriaNo ratings yet
- Rockschool-Bass-Grade-1 2 PDFDocument27 pagesRockschool-Bass-Grade-1 2 PDFmartin100% (1)
- Motor Development in Preschool and Late ChildhoodDocument81 pagesMotor Development in Preschool and Late ChildhoodPATIL.MANJULA.S.13291 5300No ratings yet
- PreschoolersDocument22 pagesPreschoolersShamae Perez100% (1)
- Sensory IntegrationDocument14 pagesSensory Integrationvenkata ramakrishnaiahNo ratings yet
- Gross Motor: USD #232 Special ServicesDocument9 pagesGross Motor: USD #232 Special ServicesSusiChelsea FanNo ratings yet
- Classic Reflex Hierarchy and ReflexesDocument8 pagesClassic Reflex Hierarchy and ReflexesJaclyn ArpinNo ratings yet
- Assessment of Gross Motor DevelopmentDocument38 pagesAssessment of Gross Motor DevelopmentGustavo Cabanas100% (2)
- Pediatric Physiotherapy Assessment Aidaaaaa 2Document15 pagesPediatric Physiotherapy Assessment Aidaaaaa 2Khaled M.A. AlqedraNo ratings yet
- Motor DevelopmentDocument91 pagesMotor DevelopmentBebe Bunso100% (1)
- 21 Positioning of Cerebral Palsy ChildDocument8 pages21 Positioning of Cerebral Palsy ChildAdnan RezaNo ratings yet
- Integrating NDT and SI-Theory and PracticeDocument7 pagesIntegrating NDT and SI-Theory and PracticePaulinaNo ratings yet
- Wee FimDocument9 pagesWee FimdeffyNo ratings yet
- WeeFIM Clinical ReviewDocument10 pagesWeeFIM Clinical Reviewsss_sarzzzNo ratings yet
- Pediatric Wheelchair Toolkit FINALDocument6 pagesPediatric Wheelchair Toolkit FINALIndiana Family to FamilyNo ratings yet
- Developmental MilestonesDocument14 pagesDevelopmental MilestonesMarimarianne100% (1)
- DR Luh - Role of PMR in NICUDocument50 pagesDR Luh - Role of PMR in NICUad putraNo ratings yet
- CARESOSA - Research Questions Set 1Document7 pagesCARESOSA - Research Questions Set 1Lucille CaresosaNo ratings yet
- Functional Assessment Checklist For Programmeing of Children With Profound Mental Retardation (Facp-Pmr)Document20 pagesFunctional Assessment Checklist For Programmeing of Children With Profound Mental Retardation (Facp-Pmr)HimaniNo ratings yet
- Pediatric Outcome MeasuresDocument40 pagesPediatric Outcome MeasuresMaybelle Anne ZamoraNo ratings yet
- OT - Milestone RetypedDocument6 pagesOT - Milestone RetypedAubrey Vale SagunNo ratings yet
- Satco Clinical WorkbookDocument6 pagesSatco Clinical WorkbookKidz to Adultz Exhibitions100% (1)
- Positioning and Handling To Foster Motor FunctionDocument60 pagesPositioning and Handling To Foster Motor FunctionBambang Ulan Aeiyu100% (1)
- Assessment of Development and GrowthDocument21 pagesAssessment of Development and Growthdrng48No ratings yet
- The Role of Early Fine and Gross MotorDocument14 pagesThe Role of Early Fine and Gross MotorClaudiaNo ratings yet
- Doris Bergen Assessment Methods For Infants and BDocument551 pagesDoris Bergen Assessment Methods For Infants and BMogoș Cris-AndreiNo ratings yet
- W1-1 Growth and Development I - LectureDocument96 pagesW1-1 Growth and Development I - Lectureali fawziNo ratings yet
- Physical, Cognitive and Socio-Emotional Developments of Intermediate SchoolersDocument10 pagesPhysical, Cognitive and Socio-Emotional Developments of Intermediate Schoolerschristian rod echonNo ratings yet
- Physical Development of Infants and ToddlersDocument31 pagesPhysical Development of Infants and ToddlersNeth CaparosNo ratings yet
- Bobath ConceptDocument5 pagesBobath ConceptdrprasantNo ratings yet
- Motor MildstonesDocument13 pagesMotor MildstonesVaio Wolff AbendrothNo ratings yet
- Chapter 8Document30 pagesChapter 8Karla CarazoNo ratings yet
- Application of Facilitatory Approaches in Developmental DysarthriaDocument22 pagesApplication of Facilitatory Approaches in Developmental Dysarthriakeihoina keihoinaNo ratings yet
- Movement Difficulties in Developmental Disorders: Practical Guidelines for Assessment and ManagementFrom EverandMovement Difficulties in Developmental Disorders: Practical Guidelines for Assessment and ManagementNo ratings yet
- Guidelines Down Syndrome Assessment and Intervention PDFDocument292 pagesGuidelines Down Syndrome Assessment and Intervention PDFZenithaMeidaNo ratings yet
- Weefim Score Sheet: Brain InjuryDocument3 pagesWeefim Score Sheet: Brain InjuryDiedeeNo ratings yet
- Weefim Score Sheet: Burns: Area Score Age Norm Is Score Due To The Burns? Explain Reasons For Giving This ScoreDocument2 pagesWeefim Score Sheet: Burns: Area Score Age Norm Is Score Due To The Burns? Explain Reasons For Giving This ScoreAlvaro Bejarano MartinNo ratings yet
- Motor SkillsDocument31 pagesMotor SkillsAzwan Azri100% (1)
- EDUC 101 Final RevisionDocument48 pagesEDUC 101 Final RevisionKate SubacNo ratings yet
- Developmental Approach or Frame of ReferenceDocument27 pagesDevelopmental Approach or Frame of ReferenceHEMA CHANDRAN100% (1)
- Management of Gross Motor (PT)Document63 pagesManagement of Gross Motor (PT)Xulkanain ZENo ratings yet
- Child Development: Prof. Rachelle Gay R. Pacial, MSN, RN Saint Louis University School of NursingDocument26 pagesChild Development: Prof. Rachelle Gay R. Pacial, MSN, RN Saint Louis University School of NursingRachelle Gay PacialNo ratings yet
- Coordination TestDocument4 pagesCoordination TestAridhotulHaqiyahNo ratings yet
- Rib Cage CoursesDocument11 pagesRib Cage CoursesPBNo ratings yet
- Coaching Approaches in Early Intervention and Paediatric RehabilitationDocument7 pagesCoaching Approaches in Early Intervention and Paediatric RehabilitationciaoNo ratings yet
- Milestones in The Development of A ChildDocument64 pagesMilestones in The Development of A ChildLakshmi Vamadevan100% (1)
- Weefim Functional Independence Measure-For ChildrenDocument18 pagesWeefim Functional Independence Measure-For ChildrenLama NammouraNo ratings yet
- GmfmscoresheetDocument6 pagesGmfmscoresheetapi-260049180No ratings yet
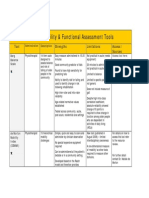
- Mobility and Functional Assessment ToolsDocument4 pagesMobility and Functional Assessment Toolssonya63265No ratings yet
- Typical and Atypical DevelopmentDocument17 pagesTypical and Atypical DevelopmentClarissa Roquero DaquioagNo ratings yet
- Reflex Testing Method For Evaluating CNS DevelopmentDocument55 pagesReflex Testing Method For Evaluating CNS DevelopmentPJHG100% (6)
- PT GoalsDocument13 pagesPT Goalsnaomi harowNo ratings yet
- Vocabulary: Match A To B To Make Phrases. A BDocument2 pagesVocabulary: Match A To B To Make Phrases. A BVictoria VmyburghNo ratings yet
- Tier 1 Irregular VerbsDocument3 pagesTier 1 Irregular VerbsRobert GloverNo ratings yet
- 21st Century Literary GenresDocument2 pages21st Century Literary GenresGO2. Aldovino Princess G.No ratings yet
- English Lesson Plan (KSSR)Document3 pagesEnglish Lesson Plan (KSSR)Suhashini RajNo ratings yet
- Cantera InglesDocument3 pagesCantera InglesJuan Reales0% (1)
- Grade 5 Third Periodical Test in MathematicsDocument7 pagesGrade 5 Third Periodical Test in Mathematicscharis l. velascoNo ratings yet
- 4.medieval BengalDocument10 pages4.medieval BengalJames MarkNo ratings yet
- The Ogham Tract - Del Auraceipt Na Eccès (Traducido)Document20 pagesThe Ogham Tract - Del Auraceipt Na Eccès (Traducido)Hector HolguinNo ratings yet
- 1st EnglishDocument4 pages1st EnglishBlasy Jean TalaidNo ratings yet
- CS502 Mcq's FinalTerm by Vu Topper RMDocument53 pagesCS502 Mcq's FinalTerm by Vu Topper RMعورت زاتNo ratings yet
- Case Test 3Document2 pagesCase Test 3John CenaNo ratings yet
- Huygens Principle and Laws of Rfraction and ReflectionDocument6 pagesHuygens Principle and Laws of Rfraction and Reflectionmahimamg2003No ratings yet
- SEA 2019 Writing Exemplars SPECIMEN PAPERDocument84 pagesSEA 2019 Writing Exemplars SPECIMEN PAPERAnthony BasantaNo ratings yet
- Saeed Mohamed Ahmed Gooda - SEDocument1 pageSaeed Mohamed Ahmed Gooda - SEsaeedgooda219No ratings yet
- Coherence Theory of TruthDocument2 pagesCoherence Theory of Truthsamu2-4u0% (1)
- Word Formation SuffixesDocument3 pagesWord Formation SuffixesgarrotemacarenaNo ratings yet
- Giselle, Mine at Last (Adult BDSM Comics)Document22 pagesGiselle, Mine at Last (Adult BDSM Comics)Arijeet SharmaNo ratings yet
- 1 Hour Lesson PlanDocument2 pages1 Hour Lesson PlanKilah IlahNo ratings yet
- DBE Answers Grade 7 Term 2 Week 3Document1 pageDBE Answers Grade 7 Term 2 Week 3msibizinhlec4No ratings yet
- Work and Jobs. Past Simple and Past ContinuousDocument18 pagesWork and Jobs. Past Simple and Past ContinuousYana FishkaNo ratings yet
- Practice Test 10Document13 pagesPractice Test 10muddasirNo ratings yet
- Ao DaiDocument2 pagesAo DaiMai Nguyễn ThịNo ratings yet
- Othello Thesis PDFDocument4 pagesOthello Thesis PDFafcmtzlda100% (2)
- Rizal Chapter 1-3Document4 pagesRizal Chapter 1-3Charissa The Ann NavarroNo ratings yet
- Plotly Express Cheat SheetDocument1 pagePlotly Express Cheat SheetMarcos Vinicius BoscariolNo ratings yet
- ConditionalsDocument1 pageConditionalsMaria Angel LopezNo ratings yet
- ReportsDocument2 pagesReportsRoba AlamatNo ratings yet
- Priniples of Church GrowthDocument47 pagesPriniples of Church Growthfrecousminzee5No ratings yet
- OOP Project ProposalDocument4 pagesOOP Project ProposalRaja Izhan Abbasi0% (1)