
Leave Requisition Form: Employee Name Designation Department
Leave Requisition Form: Employee Name Designation Department
You might also like
- Leave Request Form TemplateDocument18 pagesLeave Request Form TemplatesristakNo ratings yet
- Notice To Explain Template - PCCWDocument3 pagesNotice To Explain Template - PCCWapi-264357222No ratings yet
- Permit Overtime CertificationDocument1 pagePermit Overtime CertificationHarold ApostolNo ratings yet
- Revised Background Verification Form - Lodha GroupDocument4 pagesRevised Background Verification Form - Lodha GroupAmrit TejaniNo ratings yet
- Cuti Kecemasan - Edit 27.12.2010 (2003)Document1 pageCuti Kecemasan - Edit 27.12.2010 (2003)ISmi MumtaZahNo ratings yet
- Superceed Leave FormDocument3 pagesSuperceed Leave FormNur Syuhada RoslanNo ratings yet
- Leave ApplicationDocument1 pageLeave ApplicationLaxmikant BhandareNo ratings yet
- Application For Annual Leave: Permohanan Cuti RehatDocument1 pageApplication For Annual Leave: Permohanan Cuti RehatISmi MumtaZahNo ratings yet
- OT Request FormDocument1 pageOT Request FormMacq Trampe-ParoanNo ratings yet
- Leave Application Form: Personal ParticularsDocument1 pageLeave Application Form: Personal ParticularsNila KussrianiNo ratings yet
- Annual Leave FormDocument4 pagesAnnual Leave FormrahmanNo ratings yet
- Leave FormDocument1 pageLeave FormEncik LeepanNo ratings yet
- Leave Application FormDocument2 pagesLeave Application FormTahseen RazaNo ratings yet
- 00 Blank Time Off Request FormDocument1 page00 Blank Time Off Request FormHam ChauNo ratings yet
- Leave Application Form: 1. Applicant's DetailsDocument23 pagesLeave Application Form: 1. Applicant's DetailsMohdHuzairiRusliNo ratings yet
- Leave Form ApplicationDocument1 pageLeave Form ApplicationJun JunNo ratings yet
- Leave Cancellation FormDocument1 pageLeave Cancellation FormKanagaletchumi Veerasingam100% (1)
- Exhibit 3 - DTR - Final V2Document1 pageExhibit 3 - DTR - Final V2jessonNo ratings yet
- Leave - Permission - On Duty FormsDocument8 pagesLeave - Permission - On Duty Formsxavier_rajaNo ratings yet
- Request For Use of Vacation Time or Personal Days: Please Complete and Submit This Form To Your Provider/Office ManagerDocument1 pageRequest For Use of Vacation Time or Personal Days: Please Complete and Submit This Form To Your Provider/Office ManagerArchon RehabhNo ratings yet
- Leave Application FormDocument5 pagesLeave Application FormtalhaNo ratings yet
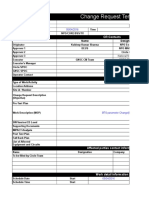
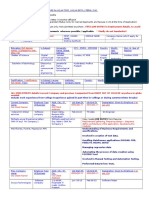
- Change Request Template: CR ContactsDocument62 pagesChange Request Template: CR ContactsKuldeep SharmaNo ratings yet
- Hrd-Leave New (4) Rev.4 - 2011Document2 pagesHrd-Leave New (4) Rev.4 - 2011asyracuaseNo ratings yet
- Employment Verification Form: o 3 Yrs Experience o Required Documents (All)Document12 pagesEmployment Verification Form: o 3 Yrs Experience o Required Documents (All)chaitu215No ratings yet
- Questionnaire For H1B and GC - 2017Document5 pagesQuestionnaire For H1B and GC - 2017Kris RavikantiNo ratings yet
- ABS-CBN Corporation: Time Keeping Justification Form (TKJF)Document1 pageABS-CBN Corporation: Time Keeping Justification Form (TKJF)Shiela ReyesNo ratings yet
- Sample Certified Job Abandonment LetterDocument1 pageSample Certified Job Abandonment LetterFELISA MANGUNENo ratings yet
- Leave Request Form R 170425Document1 pageLeave Request Form R 170425rbp9m9zz7rNo ratings yet
- 009-Courier Service RequestDocument4 pages009-Courier Service RequestShams TabrezNo ratings yet
- Online Form: The Institute of Chartered Accountants of India Final Examination - May 2012Document4 pagesOnline Form: The Institute of Chartered Accountants of India Final Examination - May 2012VenkatReddyNo ratings yet
- Leave FormDocument1 pageLeave FormApoorv MahajanNo ratings yet
- Travel Order FormDocument1 pageTravel Order FormJack SprwNo ratings yet
- Application For Leave: Employee Code: Department: Employee Name: Site / Location: DesignationDocument1 pageApplication For Leave: Employee Code: Department: Employee Name: Site / Location: Designationsanjayak_3No ratings yet
- Candidate Must Delete As Appropriate Important Information, Please ReadDocument6 pagesCandidate Must Delete As Appropriate Important Information, Please ReadsojeckNo ratings yet
- 2017 Nomination FormDocument1 page2017 Nomination FormJose PamocolNo ratings yet
- Vacation Leave (Blank Form)Document2 pagesVacation Leave (Blank Form)uddinnadeemNo ratings yet
- Timesheet & O.T. SlipDocument2 pagesTimesheet & O.T. SlipFradz RockNo ratings yet
- HR Action Form: Employee Name: Department: Date HiredDocument2 pagesHR Action Form: Employee Name: Department: Date HiredFrance Marie NTNo ratings yet
- 1 Separation ChecklistDocument2 pages1 Separation ChecklistVenu TarigoppulaNo ratings yet
- Leave Application FormatDocument1 pageLeave Application FormatdeobittuvermaNo ratings yet
- Clearance FormDocument2 pagesClearance FormselvamuthukumarNo ratings yet
- 11 Holiday Request FormDocument1 page11 Holiday Request FormYusak TewalNo ratings yet
- Manpower Requisition FormDocument3 pagesManpower Requisition FormjasmeenNo ratings yet
- Online Form: The Institute of Chartered Accountants of India Final Examination - May 2012Document4 pagesOnline Form: The Institute of Chartered Accountants of India Final Examination - May 2012Sunakshi SaxenaNo ratings yet
- Overtime Claim Form: Mon Tues Weds Thurs Fri Sat SunDocument2 pagesOvertime Claim Form: Mon Tues Weds Thurs Fri Sat SunHassan SalamaNo ratings yet
- PDF NewDocument4 pagesPDF Newapi-3745021No ratings yet
- Travel Requisition FormDocument2 pagesTravel Requisition Formamolrameshjoshi706No ratings yet
- HR FormsDocument7 pagesHR FormsChristopher Bersales LorezoNo ratings yet
- Leave Cancellation FormDocument1 pageLeave Cancellation FormbkwsubantingNo ratings yet
- Application Form CoordinatorDocument2 pagesApplication Form CoordinatorAtif ShakilNo ratings yet
- Rejoining Form: INSTRUCTION: When Employee Returns From Annual Leave, Emergency Leave, Official Business Trip or Not AsDocument1 pageRejoining Form: INSTRUCTION: When Employee Returns From Annual Leave, Emergency Leave, Official Business Trip or Not Assameh100% (1)
- Leave ApplicationDocument1 pageLeave ApplicationTM Musfiqur RahmanNo ratings yet
- Background Check Form and Letter of ConsentDocument3 pagesBackground Check Form and Letter of ConsentJohn Reigh CatipayNo ratings yet
- FORM I & Receipt GratuityDocument4 pagesFORM I & Receipt Gratuityemin100% (3)
- Leave Application FormDocument1 pageLeave Application FormjonathanelaineNo ratings yet
- Online Form: The Institute of Chartered Accountants of India Final Examination - May 2013Document4 pagesOnline Form: The Institute of Chartered Accountants of India Final Examination - May 2013Eric EllisNo ratings yet
- Force Iron & Metal: Employee InformationDocument2 pagesForce Iron & Metal: Employee InformationSarah LunnNo ratings yet
- Periodicity: Daily Reporting by Team Members/ Employees To The Team Leader/ OfficeDocument9 pagesPeriodicity: Daily Reporting by Team Members/ Employees To The Team Leader/ OfficeCA Prateek GuptaNo ratings yet
- Amkor Technology Philippines, Inc.: Payroll Adjustment FormDocument1 pageAmkor Technology Philippines, Inc.: Payroll Adjustment FormJayjay MonterdeNo ratings yet
- Pawankumar (3 3)Document3 pagesPawankumar (3 3)supriya nayakNo ratings yet
- Curriculum Vitae: Job ProfileDocument3 pagesCurriculum Vitae: Job Profilesupriya nayakNo ratings yet
- Job Description: Send Me Jobs Like ThisDocument2 pagesJob Description: Send Me Jobs Like Thissupriya nayakNo ratings yet
- Job Descriptio3 FarvisionDocument1 pageJob Descriptio3 Farvisionsupriya nayakNo ratings yet
- Stuti S0103@gmail ComDocument2 pagesStuti S0103@gmail Comsupriya nayakNo ratings yet
- CurrentDocument1 pageCurrentsupriya nayakNo ratings yet
- Book 1Document1 pageBook 1supriya nayakNo ratings yet
- Manu BiodataDocument4 pagesManu Biodatasupriya nayakNo ratings yet
- R.Rajin - Raj +91 9746473799: Academic ProfileDocument4 pagesR.Rajin - Raj +91 9746473799: Academic Profilesupriya nayakNo ratings yet
- VikramSingh (5 0)Document2 pagesVikramSingh (5 0)supriya nayakNo ratings yet
- BikramDocument3 pagesBikramsupriya nayakNo ratings yet
- Curriculum Vitae: Sunny Sudan S/o Sh. Om Parkash R/O:Ward No. 2 House No. 39 Kathua, J&K 184101 (+91) 9906028228Document3 pagesCurriculum Vitae: Sunny Sudan S/o Sh. Om Parkash R/O:Ward No. 2 House No. 39 Kathua, J&K 184101 (+91) 9906028228supriya nayakNo ratings yet
- Sushant Prakash: Seeking Assignment in Sales & Marketing With A Leading Reputable Manufacturing ConcernDocument3 pagesSushant Prakash: Seeking Assignment in Sales & Marketing With A Leading Reputable Manufacturing Concernsupriya nayakNo ratings yet
- Office CircularDocument2 pagesOffice Circularsupriya nayakNo ratings yet
- Quality Process Quality Control Quality Assurance Quality ProcessDocument1 pageQuality Process Quality Control Quality Assurance Quality Processsupriya nayakNo ratings yet
- Dear MRDocument1 pageDear MRsupriya nayakNo ratings yet









































































Download as doc, pdf, or txt
You might also like
- Leave Request Form TemplateDocument18 pagesLeave Request Form TemplatesristakNo ratings yet
- Notice To Explain Template - PCCWDocument3 pagesNotice To Explain Template - PCCWapi-264357222No ratings yet
- Permit Overtime CertificationDocument1 pagePermit Overtime CertificationHarold ApostolNo ratings yet
- Revised Background Verification Form - Lodha GroupDocument4 pagesRevised Background Verification Form - Lodha GroupAmrit TejaniNo ratings yet
- Cuti Kecemasan - Edit 27.12.2010 (2003)Document1 pageCuti Kecemasan - Edit 27.12.2010 (2003)ISmi MumtaZahNo ratings yet
- Superceed Leave FormDocument3 pagesSuperceed Leave FormNur Syuhada RoslanNo ratings yet
- Leave ApplicationDocument1 pageLeave ApplicationLaxmikant BhandareNo ratings yet
- Application For Annual Leave: Permohanan Cuti RehatDocument1 pageApplication For Annual Leave: Permohanan Cuti RehatISmi MumtaZahNo ratings yet
- OT Request FormDocument1 pageOT Request FormMacq Trampe-ParoanNo ratings yet
- Leave Application Form: Personal ParticularsDocument1 pageLeave Application Form: Personal ParticularsNila KussrianiNo ratings yet
- Annual Leave FormDocument4 pagesAnnual Leave FormrahmanNo ratings yet
- Leave FormDocument1 pageLeave FormEncik LeepanNo ratings yet
- Leave Application FormDocument2 pagesLeave Application FormTahseen RazaNo ratings yet
- 00 Blank Time Off Request FormDocument1 page00 Blank Time Off Request FormHam ChauNo ratings yet
- Leave Application Form: 1. Applicant's DetailsDocument23 pagesLeave Application Form: 1. Applicant's DetailsMohdHuzairiRusliNo ratings yet
- Leave Form ApplicationDocument1 pageLeave Form ApplicationJun JunNo ratings yet
- Leave Cancellation FormDocument1 pageLeave Cancellation FormKanagaletchumi Veerasingam100% (1)
- Exhibit 3 - DTR - Final V2Document1 pageExhibit 3 - DTR - Final V2jessonNo ratings yet
- Leave - Permission - On Duty FormsDocument8 pagesLeave - Permission - On Duty Formsxavier_rajaNo ratings yet
- Request For Use of Vacation Time or Personal Days: Please Complete and Submit This Form To Your Provider/Office ManagerDocument1 pageRequest For Use of Vacation Time or Personal Days: Please Complete and Submit This Form To Your Provider/Office ManagerArchon RehabhNo ratings yet
- Leave Application FormDocument5 pagesLeave Application FormtalhaNo ratings yet
- Change Request Template: CR ContactsDocument62 pagesChange Request Template: CR ContactsKuldeep SharmaNo ratings yet
- Hrd-Leave New (4) Rev.4 - 2011Document2 pagesHrd-Leave New (4) Rev.4 - 2011asyracuaseNo ratings yet
- Employment Verification Form: o 3 Yrs Experience o Required Documents (All)Document12 pagesEmployment Verification Form: o 3 Yrs Experience o Required Documents (All)chaitu215No ratings yet
- Questionnaire For H1B and GC - 2017Document5 pagesQuestionnaire For H1B and GC - 2017Kris RavikantiNo ratings yet
- ABS-CBN Corporation: Time Keeping Justification Form (TKJF)Document1 pageABS-CBN Corporation: Time Keeping Justification Form (TKJF)Shiela ReyesNo ratings yet
- Sample Certified Job Abandonment LetterDocument1 pageSample Certified Job Abandonment LetterFELISA MANGUNENo ratings yet
- Leave Request Form R 170425Document1 pageLeave Request Form R 170425rbp9m9zz7rNo ratings yet
- 009-Courier Service RequestDocument4 pages009-Courier Service RequestShams TabrezNo ratings yet
- Online Form: The Institute of Chartered Accountants of India Final Examination - May 2012Document4 pagesOnline Form: The Institute of Chartered Accountants of India Final Examination - May 2012VenkatReddyNo ratings yet
- Leave FormDocument1 pageLeave FormApoorv MahajanNo ratings yet
- Travel Order FormDocument1 pageTravel Order FormJack SprwNo ratings yet
- Application For Leave: Employee Code: Department: Employee Name: Site / Location: DesignationDocument1 pageApplication For Leave: Employee Code: Department: Employee Name: Site / Location: Designationsanjayak_3No ratings yet
- Candidate Must Delete As Appropriate Important Information, Please ReadDocument6 pagesCandidate Must Delete As Appropriate Important Information, Please ReadsojeckNo ratings yet
- 2017 Nomination FormDocument1 page2017 Nomination FormJose PamocolNo ratings yet
- Vacation Leave (Blank Form)Document2 pagesVacation Leave (Blank Form)uddinnadeemNo ratings yet
- Timesheet & O.T. SlipDocument2 pagesTimesheet & O.T. SlipFradz RockNo ratings yet
- HR Action Form: Employee Name: Department: Date HiredDocument2 pagesHR Action Form: Employee Name: Department: Date HiredFrance Marie NTNo ratings yet
- 1 Separation ChecklistDocument2 pages1 Separation ChecklistVenu TarigoppulaNo ratings yet
- Leave Application FormatDocument1 pageLeave Application FormatdeobittuvermaNo ratings yet
- Clearance FormDocument2 pagesClearance FormselvamuthukumarNo ratings yet
- 11 Holiday Request FormDocument1 page11 Holiday Request FormYusak TewalNo ratings yet
- Manpower Requisition FormDocument3 pagesManpower Requisition FormjasmeenNo ratings yet
- Online Form: The Institute of Chartered Accountants of India Final Examination - May 2012Document4 pagesOnline Form: The Institute of Chartered Accountants of India Final Examination - May 2012Sunakshi SaxenaNo ratings yet
- Overtime Claim Form: Mon Tues Weds Thurs Fri Sat SunDocument2 pagesOvertime Claim Form: Mon Tues Weds Thurs Fri Sat SunHassan SalamaNo ratings yet
- PDF NewDocument4 pagesPDF Newapi-3745021No ratings yet
- Travel Requisition FormDocument2 pagesTravel Requisition Formamolrameshjoshi706No ratings yet
- HR FormsDocument7 pagesHR FormsChristopher Bersales LorezoNo ratings yet
- Leave Cancellation FormDocument1 pageLeave Cancellation FormbkwsubantingNo ratings yet
- Application Form CoordinatorDocument2 pagesApplication Form CoordinatorAtif ShakilNo ratings yet
- Rejoining Form: INSTRUCTION: When Employee Returns From Annual Leave, Emergency Leave, Official Business Trip or Not AsDocument1 pageRejoining Form: INSTRUCTION: When Employee Returns From Annual Leave, Emergency Leave, Official Business Trip or Not Assameh100% (1)
- Leave ApplicationDocument1 pageLeave ApplicationTM Musfiqur RahmanNo ratings yet
- Background Check Form and Letter of ConsentDocument3 pagesBackground Check Form and Letter of ConsentJohn Reigh CatipayNo ratings yet
- FORM I & Receipt GratuityDocument4 pagesFORM I & Receipt Gratuityemin100% (3)
- Leave Application FormDocument1 pageLeave Application FormjonathanelaineNo ratings yet
- Online Form: The Institute of Chartered Accountants of India Final Examination - May 2013Document4 pagesOnline Form: The Institute of Chartered Accountants of India Final Examination - May 2013Eric EllisNo ratings yet
- Force Iron & Metal: Employee InformationDocument2 pagesForce Iron & Metal: Employee InformationSarah LunnNo ratings yet
- Periodicity: Daily Reporting by Team Members/ Employees To The Team Leader/ OfficeDocument9 pagesPeriodicity: Daily Reporting by Team Members/ Employees To The Team Leader/ OfficeCA Prateek GuptaNo ratings yet
- Amkor Technology Philippines, Inc.: Payroll Adjustment FormDocument1 pageAmkor Technology Philippines, Inc.: Payroll Adjustment FormJayjay MonterdeNo ratings yet
- Pawankumar (3 3)Document3 pagesPawankumar (3 3)supriya nayakNo ratings yet
- Curriculum Vitae: Job ProfileDocument3 pagesCurriculum Vitae: Job Profilesupriya nayakNo ratings yet
- Job Description: Send Me Jobs Like ThisDocument2 pagesJob Description: Send Me Jobs Like Thissupriya nayakNo ratings yet
- Job Descriptio3 FarvisionDocument1 pageJob Descriptio3 Farvisionsupriya nayakNo ratings yet
- Stuti S0103@gmail ComDocument2 pagesStuti S0103@gmail Comsupriya nayakNo ratings yet
- CurrentDocument1 pageCurrentsupriya nayakNo ratings yet
- Book 1Document1 pageBook 1supriya nayakNo ratings yet
- Manu BiodataDocument4 pagesManu Biodatasupriya nayakNo ratings yet
- R.Rajin - Raj +91 9746473799: Academic ProfileDocument4 pagesR.Rajin - Raj +91 9746473799: Academic Profilesupriya nayakNo ratings yet
- VikramSingh (5 0)Document2 pagesVikramSingh (5 0)supriya nayakNo ratings yet
- BikramDocument3 pagesBikramsupriya nayakNo ratings yet
- Curriculum Vitae: Sunny Sudan S/o Sh. Om Parkash R/O:Ward No. 2 House No. 39 Kathua, J&K 184101 (+91) 9906028228Document3 pagesCurriculum Vitae: Sunny Sudan S/o Sh. Om Parkash R/O:Ward No. 2 House No. 39 Kathua, J&K 184101 (+91) 9906028228supriya nayakNo ratings yet
- Sushant Prakash: Seeking Assignment in Sales & Marketing With A Leading Reputable Manufacturing ConcernDocument3 pagesSushant Prakash: Seeking Assignment in Sales & Marketing With A Leading Reputable Manufacturing Concernsupriya nayakNo ratings yet
- Office CircularDocument2 pagesOffice Circularsupriya nayakNo ratings yet
- Quality Process Quality Control Quality Assurance Quality ProcessDocument1 pageQuality Process Quality Control Quality Assurance Quality Processsupriya nayakNo ratings yet
- Dear MRDocument1 pageDear MRsupriya nayakNo ratings yet