Download as pdf or txt
You might also like
- Quaker Oats & SnappleDocument5 pagesQuaker Oats & SnappleemmafaveNo ratings yet
- Gums HNMJ v27n1p69 enDocument9 pagesGums HNMJ v27n1p69 enBazlina Zahra WahyusaputriNo ratings yet
- Research Proposal IntroductionDocument8 pagesResearch Proposal IntroductionIsaac OmwengaNo ratings yet
- Clinical Inertia in T2DM ManagementDocument11 pagesClinical Inertia in T2DM ManagementEva GabrielNo ratings yet
- PPA 124858 Factors Influencing The Quality of Life Perception in Patien VVDocument7 pagesPPA 124858 Factors Influencing The Quality of Life Perception in Patien VVBrevi Istu PambudiNo ratings yet
- Pubmed 2Document5 pagesPubmed 2Nadia HasnurNo ratings yet
- (MM2014-2-26) Chorobowość I Czynniki Ryzyka Retinopatii Cukrzycowej (DR) U Pacjentów Z Cukrzycą Typu 1 o Krótkim Okresie TrwaniaDocument5 pages(MM2014-2-26) Chorobowość I Czynniki Ryzyka Retinopatii Cukrzycowej (DR) U Pacjentów Z Cukrzycą Typu 1 o Krótkim Okresie TrwaniaTowarzystwo Edukacji TerapeutycznejNo ratings yet
- Health, Jurnal Bhs Inggris Bu Titin OkeDocument26 pagesHealth, Jurnal Bhs Inggris Bu Titin OkePrast PratamaNo ratings yet
- My Nature CureDocument16 pagesMy Nature Curehemraj.koiralaNo ratings yet
- Amelia 2018 IOP Conf. Ser. Earth Environ. Sci. 125 012171Document6 pagesAmelia 2018 IOP Conf. Ser. Earth Environ. Sci. 125 012171Marcia Lourdes Larico BernabéNo ratings yet
- Factors Associated With Self-Care Behavior of Elderly Patients With Type 2Document4 pagesFactors Associated With Self-Care Behavior of Elderly Patients With Type 2audy saviraNo ratings yet
- Pengaruh Hipoglikemia Pada Pasien Diabetes MelitusDocument8 pagesPengaruh Hipoglikemia Pada Pasien Diabetes Melitusmail junkNo ratings yet
- Health and Quality of Life OutcomesDocument11 pagesHealth and Quality of Life OutcomesAoikiji KuzanNo ratings yet
- Pengaruh Hipoglikemia Pada Pasien Diabetes Melitus Tipe 2 Terhadap Kepatuhan Terapi Dan Kualitas HidupDocument8 pagesPengaruh Hipoglikemia Pada Pasien Diabetes Melitus Tipe 2 Terhadap Kepatuhan Terapi Dan Kualitas Hidupilma adilla syahidaNo ratings yet
- Alencar 2010Document6 pagesAlencar 2010Tín NguyễnNo ratings yet
- Diabetes and Cardiovascular Disease: Story of DiscoveryDocument5 pagesDiabetes and Cardiovascular Disease: Story of DiscoveryMahesh DmNo ratings yet
- HypoglikemiaDocument12 pagesHypoglikemiaChandra PandianganNo ratings yet
- Research Article: Keywords: Health Related Quality of Life, Insulin Based Therapy, Type 2 Diabetes MellitusDocument9 pagesResearch Article: Keywords: Health Related Quality of Life, Insulin Based Therapy, Type 2 Diabetes MellitusNadia HasnurNo ratings yet
- Medication Review 1Document5 pagesMedication Review 1baiqnesya9No ratings yet
- Adherence and Quality of Life Among Diabetic Patients With HypertensionDocument6 pagesAdherence and Quality of Life Among Diabetic Patients With HypertensionIJPHSNo ratings yet
- Editorial: Complications of Diabetes 2017Document5 pagesEditorial: Complications of Diabetes 2017landoo oooNo ratings yet
- Komplikasi DiabetesDocument4 pagesKomplikasi DiabetesFrans SaputraNo ratings yet
- Health Beliefs, Self-Care Behaviors and Quality of Life in Adults With Type 2 DiabetesDocument9 pagesHealth Beliefs, Self-Care Behaviors and Quality of Life in Adults With Type 2 DiabetesgamzeNo ratings yet
- CardiovascularDocument9 pagesCardiovascularPra BowoNo ratings yet
- The Relationship of Diabetes Mellitus Diet Knowledge With Blood Glucose Levels in Patients Diabetes Mellitus Type Ii in Hermana Hospital LembeanDocument5 pagesThe Relationship of Diabetes Mellitus Diet Knowledge With Blood Glucose Levels in Patients Diabetes Mellitus Type Ii in Hermana Hospital LembeanIrene Hana HutagalungNo ratings yet
- Glimepiride 13 (18.84%) Dan Gliquidon 21 (30.43%) Metformin 29 (40.03%), Thiazolinedone Jenis Obat Pioglitazone 6 (8.7%)Document10 pagesGlimepiride 13 (18.84%) Dan Gliquidon 21 (30.43%) Metformin 29 (40.03%), Thiazolinedone Jenis Obat Pioglitazone 6 (8.7%)noviantyramadhani12No ratings yet
- HUang, 2008 D-39Document12 pagesHUang, 2008 D-39Fadel TrianzahNo ratings yet
- Current Concepts in Diabetic Retinopathy: Diabetes & Metabolism Journal December 2014Document11 pagesCurrent Concepts in Diabetic Retinopathy: Diabetes & Metabolism Journal December 2014Elison J PanggaloNo ratings yet
- Final Article 4 IJMSNR 31.03.2022Document7 pagesFinal Article 4 IJMSNR 31.03.2022Int J of Med Sci and Nurs ResNo ratings yet
- Ass Knowledge and MaDocument1 pageAss Knowledge and MaB04-BALKIS SOLEHAHNo ratings yet
- Diabetic Medicine - 2017 - Perrin - The Prevalence of Diabetes Specific Emotional Distress in People With Type 2 DiabetesDocument13 pagesDiabetic Medicine - 2017 - Perrin - The Prevalence of Diabetes Specific Emotional Distress in People With Type 2 Diabetesnirmala amirNo ratings yet
- Health and Quality of Life Outcomes Impairment of Quality of Life in Type 2 Diabetes Mellitus: A Cross-Sectional StudyDocument7 pagesHealth and Quality of Life Outcomes Impairment of Quality of Life in Type 2 Diabetes Mellitus: A Cross-Sectional StudyFadel TrianzahNo ratings yet
- Journal of Diabetes and Its ComplicationsDocument5 pagesJournal of Diabetes and Its ComplicationsQqNo ratings yet
- Factors Related To Non-Adherence To Lifestyle Modi PDFDocument9 pagesFactors Related To Non-Adherence To Lifestyle Modi PDFnorma widya afrianiNo ratings yet
- Longitudinal Predictors of Reduced Mobility and Physical Disability in Patients With Type 2 DiabetesDocument7 pagesLongitudinal Predictors of Reduced Mobility and Physical Disability in Patients With Type 2 DiabetesNugiNo ratings yet
- Predictors For Diabetic Retinopathy in Normoalbuminuric People With Type 2 Diabetes MellitusDocument6 pagesPredictors For Diabetic Retinopathy in Normoalbuminuric People With Type 2 Diabetes MellitusdrheriNo ratings yet
- Diabetes Distress Paper EfmjDocument16 pagesDiabetes Distress Paper EfmjAhmed NabilNo ratings yet
- Developing and Validating The Arabic Version of The Diabetes Quality of Life QuestionnaireDocument13 pagesDeveloping and Validating The Arabic Version of The Diabetes Quality of Life Questionnairezomorda kammounNo ratings yet
- Diabetic MacularDocument15 pagesDiabetic MacularagugdewiNo ratings yet
- 717-Article Text-2767-1-10-20200813Document8 pages717-Article Text-2767-1-10-20200813Devana Prayitno PutriNo ratings yet
- Alasan Ke ManusiaDocument12 pagesAlasan Ke ManusiaafiwahyuNo ratings yet
- Efektivitas Konseling DM Dalam Meningkatkan Kepatuhan Dan Pengendalian Gula Darah Pada Diabetes Melitus Tipe 2Document12 pagesEfektivitas Konseling DM Dalam Meningkatkan Kepatuhan Dan Pengendalian Gula Darah Pada Diabetes Melitus Tipe 2AmmarForeverAjaNo ratings yet
- Effectiveness - of - Cognitive - Beh7 NewDocument10 pagesEffectiveness - of - Cognitive - Beh7 NewfitrianiNo ratings yet
- Appendix B: Analysis Plan/Application Data/materialsDocument6 pagesAppendix B: Analysis Plan/Application Data/materialsOtieno MosesNo ratings yet
- Pengaruh Hipoglikemia Pada Pasien Diabetes Melitus Tipe 2 Terhadap Kepatuhan Terapi Dan Kualitas HidupDocument7 pagesPengaruh Hipoglikemia Pada Pasien Diabetes Melitus Tipe 2 Terhadap Kepatuhan Terapi Dan Kualitas HidupAhmad RivaiNo ratings yet
- Diabetic Autonomic Neuropathy - UpToDateDocument30 pagesDiabetic Autonomic Neuropathy - UpToDatehlau2uciNo ratings yet
- KretchyDocument10 pagesKretchyPoppy ArnitaNo ratings yet
- Zur IngestDocument29 pagesZur IngestraychandwpNo ratings yet
- Cohort Profile: The Japan Diabetes Complications Study: A Long-Term Follow-Up of A Randomised Lifestyle Intervention Study of Type 2 DiabetesDocument9 pagesCohort Profile: The Japan Diabetes Complications Study: A Long-Term Follow-Up of A Randomised Lifestyle Intervention Study of Type 2 DiabetesPutri HakimNo ratings yet
- JurnalDocument7 pagesJurnalGangsar DamaiNo ratings yet
- Diabetes Mellitus Therapy in Hospitalized Patients at Dr. Soebandi Jember Hospital 2015 Period)Document7 pagesDiabetes Mellitus Therapy in Hospitalized Patients at Dr. Soebandi Jember Hospital 2015 Period)septri desiNo ratings yet
- Diabetic Retinopathy: Merican Iabetes SsociationDocument4 pagesDiabetic Retinopathy: Merican Iabetes SsociationMuhammad Wahyu SetianiNo ratings yet
- Al Shehri 2008Document10 pagesAl Shehri 2008Dewi MaryamNo ratings yet
- Serum C-Peptide Concentrations Poorly Phenotype Type 2 Diabetic End-Stage Renal Disease PatientsDocument9 pagesSerum C-Peptide Concentrations Poorly Phenotype Type 2 Diabetic End-Stage Renal Disease PatientsekaNo ratings yet
- 1304 FullDocument8 pages1304 FullNurul AmaliaNo ratings yet
- Dme 12651Document46 pagesDme 12651emmanuel cavazosNo ratings yet
- The UK Prospective Diabetes Study (UKPDS) : Clinical and Therapeutic Implications For Type 2 DiabetesDocument6 pagesThe UK Prospective Diabetes Study (UKPDS) : Clinical and Therapeutic Implications For Type 2 DiabetesLaila KurniaNo ratings yet
- 5 Assessment of KnowledgeDocument14 pages5 Assessment of KnowledgeNejash Abdo IssaNo ratings yet
- Wa0012.Document18 pagesWa0012.Damar MiftaNo ratings yet
- EN-the-correlation-between-level-of-diabetiDocument6 pagesEN-the-correlation-between-level-of-diabetiMutiara Khaerun NisaNo ratings yet
- Diabetes Mellitus and Oral Health: An Interprofessional ApproachFrom EverandDiabetes Mellitus and Oral Health: An Interprofessional ApproachNo ratings yet
- Rubric For Short Scene With Literary DevicesDocument1 pageRubric For Short Scene With Literary DevicespaympmnpNo ratings yet
- Use Passing Chords - LarsenDocument9 pagesUse Passing Chords - Larsenrla97623No ratings yet
- Banking AssignmentDocument23 pagesBanking AssignmentRitika Ritz100% (1)
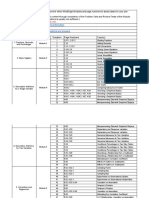
- Data Siswa Kelas Xii 2018Document84 pagesData Siswa Kelas Xii 2018Kang Mas HurieyNo ratings yet
- C955 Pre-Assessment - MindEdge Alignment Table - Sheet1Document3 pagesC955 Pre-Assessment - MindEdge Alignment Table - Sheet1Robert Allen Rippey0% (1)
- 4209 ArticleText 15346 1 10 202101142020Document15 pages4209 ArticleText 15346 1 10 202101142020Selmitha SariNo ratings yet
- Unit 10: Values: Lesson A Objective: Learn To Talk About Moral DilemmasDocument7 pagesUnit 10: Values: Lesson A Objective: Learn To Talk About Moral DilemmasLiss PeñafielNo ratings yet
- Navratna: Navratna Was The Title Given Originally To NineDocument5 pagesNavratna: Navratna Was The Title Given Originally To NineblokeshwaranNo ratings yet
- DUCKWEEDDocument2 pagesDUCKWEEDRALPH LAURENCE CASTRONo ratings yet
- Edward B. Hager v. United States, 993 F.2d 4, 1st Cir. (1993)Document3 pagesEdward B. Hager v. United States, 993 F.2d 4, 1st Cir. (1993)Scribd Government DocsNo ratings yet
- Camera Market InformationDocument5 pagesCamera Market InformationprabsyNo ratings yet
- Computer Systems Servicing: 3 Quarter Week 1Document7 pagesComputer Systems Servicing: 3 Quarter Week 1Romnick PortillanoNo ratings yet
- People v. Sy Pio, G.R. No. L-5848. April 30, 1954Document3 pagesPeople v. Sy Pio, G.R. No. L-5848. April 30, 1954Anna BarbadilloNo ratings yet
- Electromagnatic InductionDocument1 pageElectromagnatic InductionMahes JeyNo ratings yet
- SBP - Pengenalan, Induksi RulesDocument37 pagesSBP - Pengenalan, Induksi RulesTU ElektroNo ratings yet
- Agricultural Crop Production 11 - Q2 - W5Document5 pagesAgricultural Crop Production 11 - Q2 - W5Jennifer DuranNo ratings yet
- Installation Guide T-Marc 3306 MN100280 Revision ADocument43 pagesInstallation Guide T-Marc 3306 MN100280 Revision AMarco Ur100% (1)
- Conflict of Laws Paras and Salonga Reviewer PDFDocument40 pagesConflict of Laws Paras and Salonga Reviewer PDFAlyza Montilla Burdeos100% (1)
- Chapter Three Theft Article 308. Who Are Liable For Theft. - Theft Is Committed by Any Person Who, With Intent To Gain ButDocument4 pagesChapter Three Theft Article 308. Who Are Liable For Theft. - Theft Is Committed by Any Person Who, With Intent To Gain Butquail090909No ratings yet
- Female Psychology A-Z FREE GuideDocument37 pagesFemale Psychology A-Z FREE Guideklaus Beck100% (8)
- Jurnal Life BirthDocument18 pagesJurnal Life BirthSiska Cahyati FatimahNo ratings yet
- Occupational Therapy's Role in Post Concussion Management: Aimil Parmelee, MOT, OTR/L Marlaina Montgomery, MOT, OTR/LDocument27 pagesOccupational Therapy's Role in Post Concussion Management: Aimil Parmelee, MOT, OTR/L Marlaina Montgomery, MOT, OTR/Lsidney drecotteNo ratings yet
- CHM432 Fundamental Physical Chemistry: ThermodynamicsDocument97 pagesCHM432 Fundamental Physical Chemistry: ThermodynamicsPriscyyNo ratings yet
- Academic Year Şh. Yavuz Ulutaş Çelikoğlu Ortaokulu 2Nd Term 2Nd Elective English Exam For 7Th GradersDocument2 pagesAcademic Year Şh. Yavuz Ulutaş Çelikoğlu Ortaokulu 2Nd Term 2Nd Elective English Exam For 7Th GradersMustafa YamanNo ratings yet
- Design and Analysis of A Basic Class D AmplifierDocument22 pagesDesign and Analysis of A Basic Class D AmplifieranisettimanikantaNo ratings yet
- Walking With Miss Millie Readers TheaterDocument6 pagesWalking With Miss Millie Readers Theaterapi-547921371No ratings yet
- Olego vs. RebuenoDocument3 pagesOlego vs. RebuenoCaitlin KintanarNo ratings yet
- A Discourse of Amanat Galunggung TerjemahkanDocument10 pagesA Discourse of Amanat Galunggung TerjemahkanGelar T. KusumawardhanaNo ratings yet
- Geological Field Report of Attock Cherat RangesDocument12 pagesGeological Field Report of Attock Cherat RangesAnwar U Din100% (2)