Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5820)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Blank Lab Work ReportsDocument8 pagesBlank Lab Work ReportsPamTremble100% (4)
- Shubhangini A Joshi - Nutrition and Dietetics (2015, McGraw-Hill Education)Document676 pagesShubhangini A Joshi - Nutrition and Dietetics (2015, McGraw-Hill Education)Ravi Kumar Verma94% (54)
- ISO 50001 StandardDocument17 pagesISO 50001 StandardMuhammad Reza PradectaNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Scholarship Maeci 2019 2020 PDFDocument1 pageScholarship Maeci 2019 2020 PDFMuhammad Reza PradectaNo ratings yet
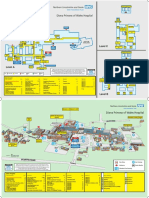
- Diana Princess of Wales Hospital: Level CDocument2 pagesDiana Princess of Wales Hospital: Level CTeamkamal FillahNo ratings yet
- Program Specification of Mechanical Engineering Undergraduate ProgramDocument11 pagesProgram Specification of Mechanical Engineering Undergraduate ProgramMuhammad Reza PradectaNo ratings yet
- Scholarships Poli Milano 2019 F PDocument3 pagesScholarships Poli Milano 2019 F PMuhammad Reza PradectaNo ratings yet
- Concordance Table FinalDocument1 pageConcordance Table FinalMuhammad Reza PradectaNo ratings yet
- General Formula of ReliabilityDocument2 pagesGeneral Formula of ReliabilityMuhammad Reza Pradecta100% (1)
- Muhammad Reza Pradecta - International Conference On Energy Sciences 2019-2Document8 pagesMuhammad Reza Pradecta - International Conference On Energy Sciences 2019-2Muhammad Reza PradectaNo ratings yet
- Cost of Electricity From Enhanced Geothermal SystemsDocument11 pagesCost of Electricity From Enhanced Geothermal SystemsMuhammad Reza PradectaNo ratings yet
- Research Topics: International Research Center For Hydrogen EnergyDocument1 pageResearch Topics: International Research Center For Hydrogen EnergyMuhammad Reza PradectaNo ratings yet
- NeuCo Boiler OptimisationDocument40 pagesNeuCo Boiler OptimisationMuhammad Reza PradectaNo ratings yet
- System Refrigerasi Lec 1 S1Document37 pagesSystem Refrigerasi Lec 1 S1Muhammad Reza PradectaNo ratings yet
- M3 TKM3306 1D ConductionDocument37 pagesM3 TKM3306 1D ConductionMuhammad Reza PradectaNo ratings yet
- Route To MajalengkaDocument3 pagesRoute To MajalengkaMuhammad Reza PradectaNo ratings yet
- 25 Application of Complex Numbers To Parallel A.C. NetworksDocument1 page25 Application of Complex Numbers To Parallel A.C. NetworksMuhammad Reza PradectaNo ratings yet
- Vol06 b2 32-33strDocument2 pagesVol06 b2 32-33strAyuAnggayantiNo ratings yet
- Booklet The 8th JAKINUDocument20 pagesBooklet The 8th JAKINUsamuelionardiNo ratings yet
- V 5 N 1Document190 pagesV 5 N 1Jorge RodriguezNo ratings yet
- Pathmorpho2nd 1Document1 pagePathmorpho2nd 1Hart ElettNo ratings yet
- Screw Retained Vs Cement Retained Implant-Supported Fixed Dental ProsthesisDocument11 pagesScrew Retained Vs Cement Retained Implant-Supported Fixed Dental ProsthesisMario Troncoso AndersennNo ratings yet
- De Quervain's TendinosisDocument19 pagesDe Quervain's TendinosisSze Wing LeeNo ratings yet
- Dental Fear/anxiety Among Children and Adolescents. A Systematic ReviewDocument10 pagesDental Fear/anxiety Among Children and Adolescents. A Systematic ReviewfghdhmdkhNo ratings yet
- Introduction To MetagenomicsDocument16 pagesIntroduction To MetagenomicsSuhail PatharvatNo ratings yet
- Acsm NormsDocument5 pagesAcsm NormsSagar Gawankar100% (1)
- Novel Drugs Targeting The Sars-Cov-2/Covid-19 Machinery: Ariane Sternberg, Dwight L. Mckee and Cord NaujokatDocument11 pagesNovel Drugs Targeting The Sars-Cov-2/Covid-19 Machinery: Ariane Sternberg, Dwight L. Mckee and Cord Naujokatperi umardianaNo ratings yet
- Agustus Monitoring HemodinamikDocument61 pagesAgustus Monitoring HemodinamikFikriYTNo ratings yet
- Ablation Pédiatrique Alice MaltretDocument36 pagesAblation Pédiatrique Alice Maltretmihalcea alinNo ratings yet
- ART20199185 Kaya Kalpa Benefits StudyDocument5 pagesART20199185 Kaya Kalpa Benefits StudyRaghavendra RaoNo ratings yet
- Degree of Burns: CharacteristicsDocument2 pagesDegree of Burns: CharacteristicsAnu TripathiNo ratings yet
- 13 Unit 5 PainDocument4 pages13 Unit 5 PainAndres SalazarNo ratings yet
- Asthma Bronchiale: Dr. Ramelan Navy Hospital SurabayaDocument53 pagesAsthma Bronchiale: Dr. Ramelan Navy Hospital SurabayaCornelia CindyNo ratings yet
- Predictors of Outcome in AneurysmalDocument7 pagesPredictors of Outcome in AneurysmalNeni NirmalaNo ratings yet
- UntitledDocument264 pagesUntitledFed Espiritu Santo GNo ratings yet
- Faisal ImranDocument2 pagesFaisal ImranSharjeel AhmedNo ratings yet
- Endometriosis GuidelineDocument44 pagesEndometriosis GuidelineHen DriNo ratings yet
- By Muslimah: The Healing Powers of The Names of AllahDocument2 pagesBy Muslimah: The Healing Powers of The Names of AllahMOULIANNA8949No ratings yet
- V. AzapironesDocument2 pagesV. AzapironesChristine Pialan SalimbagatNo ratings yet
- Rcs e v13 With Guidelines Score SheetDocument4 pagesRcs e v13 With Guidelines Score SheetgabrimarteNo ratings yet
- Best Practice Recommendations For Management of Boutonnier Deformity in Rheumatoid ArthritisDocument8 pagesBest Practice Recommendations For Management of Boutonnier Deformity in Rheumatoid ArthritisRisa MuthmainahNo ratings yet
- Hormone HandoutDocument2 pagesHormone Handoutszisz889No ratings yet
- Giant Juvenile Fibroadenoma of Breast Mimicking Phylloides Tumour - A Case ReportDocument8 pagesGiant Juvenile Fibroadenoma of Breast Mimicking Phylloides Tumour - A Case ReportsridharNo ratings yet
- Local AnestheticsDocument44 pagesLocal Anestheticsblack pink in ur area 21No ratings yet