Download as pdf or txt
You might also like
- Alchemy IlluminatedDocument100 pagesAlchemy Illuminatedtravellerfellow100% (11)
- Critical Appraisal of EvidenceDocument5 pagesCritical Appraisal of EvidenceLADY JOWAHER ALLASNo ratings yet
- Coca-Cola Porters Five Forces-SWOT AnalysisDocument72 pagesCoca-Cola Porters Five Forces-SWOT Analysishahahakim50% (2)
- SpriteDocument18 pagesSpriteNupur BagdiNo ratings yet
- Fallout - New Vegas PerksDocument7 pagesFallout - New Vegas PerksJosé Luis Buenaño DuránNo ratings yet
- Module 4 NRSG780Document9 pagesModule 4 NRSG780justdoyourNo ratings yet
- Impact of A Designed Self-Care Program On Selected Outcomes Among Patients Undergoing HemodialysisDocument18 pagesImpact of A Designed Self-Care Program On Selected Outcomes Among Patients Undergoing HemodialysisImpact JournalsNo ratings yet
- Health Belief ModelDocument12 pagesHealth Belief Modelrenzelpacleb123No ratings yet
- The Effect of Progressive Muscle Relaxation On Cancer Patients' Self-EfficacyDocument8 pagesThe Effect of Progressive Muscle Relaxation On Cancer Patients' Self-EfficacySyahri FaziraNo ratings yet
- Ramseier Et Al-2015-Journal of Clinical Periodontology PDFDocument12 pagesRamseier Et Al-2015-Journal of Clinical Periodontology PDFChristine HacheNo ratings yet
- Quality of Life of Filipino Cancer PatientsDocument2 pagesQuality of Life of Filipino Cancer PatientsApril Garcia MayoNo ratings yet
- The Practices Subspecialty Internists Counseling Smoking ExerciseDocument5 pagesThe Practices Subspecialty Internists Counseling Smoking ExerciseIlyichia HuttonNo ratings yet
- Pelvic Pain in EndometriosisDocument7 pagesPelvic Pain in Endometriosism_tonydharmawanNo ratings yet
- Periodic Health ExaminationDocument38 pagesPeriodic Health ExaminationHilma NadhifaNo ratings yet
- Jurnal Cbe 1Document21 pagesJurnal Cbe 1Dewi SurayaNo ratings yet
- TUIL 4 - Ivan Wima Aditama - 20548 - 05 PDFDocument6 pagesTUIL 4 - Ivan Wima Aditama - 20548 - 05 PDFIvan Wima AditamaNo ratings yet
- Healthy Teens Counseling ApproachDocument6 pagesHealthy Teens Counseling ApproachDebbie CharlotteNo ratings yet
- Cancer - 1 October 1994 - Given - The Impact of Age Treatment and Symptoms On The Physical and Mental Health of CancerDocument11 pagesCancer - 1 October 1994 - Given - The Impact of Age Treatment and Symptoms On The Physical and Mental Health of Cancervyhnl.psyNo ratings yet
- Research Article: Acupuncture For Functional Dyspepsia: A Single Blinded, Randomized, Controlled TrialDocument10 pagesResearch Article: Acupuncture For Functional Dyspepsia: A Single Blinded, Randomized, Controlled TrialairinNo ratings yet
- Sopc 2023 GhidDocument26 pagesSopc 2023 GhidVlad RadulescuNo ratings yet
- Promoting in MMDocument8 pagesPromoting in MMAna Luiza ToldoNo ratings yet
- Evidence Based Health Maintenance Protocols (Screening) in Adult/elderlyDocument58 pagesEvidence Based Health Maintenance Protocols (Screening) in Adult/elderlyB 70 Mohit KumarNo ratings yet
- Empowerment Program For People With Prediabetes: A Randomized Controlled TrialDocument13 pagesEmpowerment Program For People With Prediabetes: A Randomized Controlled TrialMittaningtyasNo ratings yet
- Counseling Overweight Patients: Analysis of Preventive Encounters in Primary CareDocument7 pagesCounseling Overweight Patients: Analysis of Preventive Encounters in Primary CareAgil SulistyonoNo ratings yet
- JournalDocument31 pagesJournalNandini VermaNo ratings yet
- Blood PressureDocument13 pagesBlood PressuremerlinNo ratings yet
- Abstract JURNAL SKRIPSI 2Document11 pagesAbstract JURNAL SKRIPSI 2Ade RatnasariNo ratings yet
- Constructing A General Competency Model For Chinese Public Health Physicians: A Qualitative and Quantitative StudyDocument7 pagesConstructing A General Competency Model For Chinese Public Health Physicians: A Qualitative and Quantitative StudyClumsyNo ratings yet
- Clinical Profile of First Year College StudentsDocument39 pagesClinical Profile of First Year College StudentsEppie Aliño BallouzNo ratings yet
- P3 Health StatusDocument9 pagesP3 Health StatusNovita Mariani GlekoNo ratings yet
- JCM 08 00454Document8 pagesJCM 08 00454Harnoor GhumanNo ratings yet
- Journal of Experimental & Clinical Cancer ResearchDocument31 pagesJournal of Experimental & Clinical Cancer Researchrawan_83No ratings yet
- The Health Belief Model Is A Theoretical Framework For Guiding Health Promotion and Disease Prevention Measures in Public HealthDocument3 pagesThe Health Belief Model Is A Theoretical Framework For Guiding Health Promotion and Disease Prevention Measures in Public HealthLarr SumalpongNo ratings yet
- Licenciatura en Psicología: Cd. Victoria, Tam. Febrero de 2014Document17 pagesLicenciatura en Psicología: Cd. Victoria, Tam. Febrero de 2014Denisse ChaconNo ratings yet
- JaffeDocument2 pagesJafferbtakemotoNo ratings yet
- Medicine and Research An Ever-Changing FieldDocument7 pagesMedicine and Research An Ever-Changing Fieldapi-665163291No ratings yet
- Proceeding The 4Th International Nursing Conference "Life Cycle Approach For Successful Aging" ISBN: 978 - 602 - 6988 - 78 - 2Document9 pagesProceeding The 4Th International Nursing Conference "Life Cycle Approach For Successful Aging" ISBN: 978 - 602 - 6988 - 78 - 2omingNo ratings yet
- Nama: Delya Siti Annisa Ibrahim NIM: 1902444 Hospital Personnel/Healthcare WorkersDocument6 pagesNama: Delya Siti Annisa Ibrahim NIM: 1902444 Hospital Personnel/Healthcare Workersdelya siti annisa ibrahimNo ratings yet
- Influence of Health Education To Improve The Proper Self Medica Tion Beha ViorDocument10 pagesInfluence of Health Education To Improve The Proper Self Medica Tion Beha Viorabdul andhimNo ratings yet
- HKG - Exercise Prescription (Doctor's Handbook)Document126 pagesHKG - Exercise Prescription (Doctor's Handbook)Chi-Wa CWNo ratings yet
- HSR ManDocument26 pagesHSR ManRana ObaidNo ratings yet
- Florindo Et Al., 2013 - Physical Activity Counseling in Primary Health Care in Brazil - A National Study On Prevalence and Associated FactorsDocument10 pagesFlorindo Et Al., 2013 - Physical Activity Counseling in Primary Health Care in Brazil - A National Study On Prevalence and Associated FactorsmarcferrNo ratings yet
- Learning ObjectivesDocument20 pagesLearning ObjectivesOmar MohamedNo ratings yet
- Health-Related Quality of Life in Chronic Renal Predialysis Patients Exposed To A Prevention Program - Medellín, 2007-2008Document14 pagesHealth-Related Quality of Life in Chronic Renal Predialysis Patients Exposed To A Prevention Program - Medellín, 2007-2008Alejandro Vesga VinchiraNo ratings yet
- Wellness BehaviourDocument2 pagesWellness BehaviourJohn Paul Ta PhamNo ratings yet
- Effect of Intensive Health Education On Adherence To Treatment in Sputum Positive Pulmonary Tuberculosis PatientsDocument6 pagesEffect of Intensive Health Education On Adherence To Treatment in Sputum Positive Pulmonary Tuberculosis PatientspocutindahNo ratings yet
- Quality of Life in Patients With End Stage Renal Disease On HemodialysisDocument11 pagesQuality of Life in Patients With End Stage Renal Disease On HemodialysisAmalia UtamiNo ratings yet
- 18 Gouri Et AlDocument6 pages18 Gouri Et AleditorijmrhsNo ratings yet
- The Impact of Cancer On Children's Physical, Emotional, and Psychosocial Well-BeingDocument3 pagesThe Impact of Cancer On Children's Physical, Emotional, and Psychosocial Well-BeingRegina Masli PutriNo ratings yet
- Objectives: - Introduction: This Section Provides An Overview ofDocument14 pagesObjectives: - Introduction: This Section Provides An Overview ofonlineNo ratings yet
- ESRD Secondary To Diabetic Nephropathy CASE STUDY Docx 2Document42 pagesESRD Secondary To Diabetic Nephropathy CASE STUDY Docx 2Eyerusalem100% (1)
- Counselling Problem Drinkers in Medical Wards: Study: A ControlledDocument3 pagesCounselling Problem Drinkers in Medical Wards: Study: A ControlledIlyichia HuttonNo ratings yet
- (R) PainDocument7 pages(R) PainVera El Sammah SiagianNo ratings yet
- Articulo Parcial EvaluaciónDocument9 pagesArticulo Parcial Evaluacióntavo890110No ratings yet
- Review of LiteratureDocument16 pagesReview of Literatureakhils.igjNo ratings yet
- Running Head: EXERCISE AND HEALTH 1Document12 pagesRunning Head: EXERCISE AND HEALTH 1api-281674546No ratings yet
- 2000 MICHAEL SPECA - A Randomized, Wait-List Controlled Clinical Trial The Effect of A MindfulnessDocument10 pages2000 MICHAEL SPECA - A Randomized, Wait-List Controlled Clinical Trial The Effect of A Mindfulnessnermal93No ratings yet
- Pesquisa Grega 2014Document8 pagesPesquisa Grega 2014Ricardo BrandaoNo ratings yet
- Medi 95 E2791Document5 pagesMedi 95 E2791Harnoor GhumanNo ratings yet
- Bju 14047Document18 pagesBju 14047jedan185No ratings yet
- NEUK 1464 (Revised) 1 (Updated)Document21 pagesNEUK 1464 (Revised) 1 (Updated)Sameen ShafaatNo ratings yet
- Atlas of Inflammatory Bowel DiseasesFrom EverandAtlas of Inflammatory Bowel DiseasesWon Ho KimNo ratings yet
- Screening For Good Health: The Australian Guide To Health Screening And ImmunisationFrom EverandScreening For Good Health: The Australian Guide To Health Screening And ImmunisationNo ratings yet
- The Research on Anticancer Traditional Chinese Medication with Immune Regulation and Control: ——Experimental Research and Clinical Application VerificationFrom EverandThe Research on Anticancer Traditional Chinese Medication with Immune Regulation and Control: ——Experimental Research and Clinical Application VerificationNo ratings yet
- Am J Clin Nutr 2008 O'Donnell 1388 95Document8 pagesAm J Clin Nutr 2008 O'Donnell 1388 95YaumilKhalidaNo ratings yet
- Impact of Imposed Exercise On Energy Intake in Children at Risk For OverweightDocument9 pagesImpact of Imposed Exercise On Energy Intake in Children at Risk For OverweightYaumilKhalidaNo ratings yet
- Musculus Origo Insersi Fungsi Inervasi Pleksus M. IliacusDocument5 pagesMusculus Origo Insersi Fungsi Inervasi Pleksus M. IliacusYaumilKhalidaNo ratings yet
- Treadmill Stress TestingDocument23 pagesTreadmill Stress TestingYaumilKhalidaNo ratings yet
- Vignesh WKDocument57 pagesVignesh WKVignesh KrishnanNo ratings yet
- Jewish Telegraph in BohinjDocument2 pagesJewish Telegraph in BohinjbohinjparkhotelNo ratings yet
- Relaxed Pronunciation ReferenceDocument8 pagesRelaxed Pronunciation Referencevimal276No ratings yet
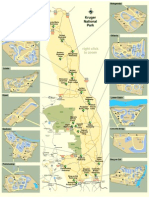
- KNP Camps Gates MapDocument1 pageKNP Camps Gates MapAdmin MindocsNo ratings yet
- Soyabean Milk Project Class 12Document8 pagesSoyabean Milk Project Class 12Neba Khan40% (5)
- Germany Poem Cup Waikoloa Spiegelau Import Crystal Brandy Glass White Wine Cup Ocean - Lazada PHDocument5 pagesGermany Poem Cup Waikoloa Spiegelau Import Crystal Brandy Glass White Wine Cup Ocean - Lazada PHjune dela cernaNo ratings yet
- Batti / Grandmothers / Prepare / OftenDocument2 pagesBatti / Grandmothers / Prepare / OftenNatalia PereaNo ratings yet
- Long Island Wine Press - Summer 2012Document88 pagesLong Island Wine Press - Summer 2012Wine Press100% (1)
- The Perceptions of Grade 12 Students (2019-2020) On The Effects of Beverages Consumed On Their Study Habits at HomeDocument21 pagesThe Perceptions of Grade 12 Students (2019-2020) On The Effects of Beverages Consumed On Their Study Habits at Homebry uyNo ratings yet
- Kami Export - Lucas Perez - Prohibitions WebquestDocument3 pagesKami Export - Lucas Perez - Prohibitions WebquestTactical DogeNo ratings yet
- How To Get Taller - 7 Step To Take Based On ScienceDocument10 pagesHow To Get Taller - 7 Step To Take Based On SciencehealthcrabNo ratings yet
- FBS QuizDocument3 pagesFBS QuizPam EstoqueNo ratings yet
- History of Frozen Foods and Its EvolutionsDocument7 pagesHistory of Frozen Foods and Its Evolutionssha_beeNo ratings yet
- Marketing Management: East West UniversityDocument51 pagesMarketing Management: East West UniversityYeasin Tusher100% (1)
- How To Heal Leaky GutDocument26 pagesHow To Heal Leaky Gutajax86% (7)
- PSY201 Review 7Document4 pagesPSY201 Review 7Sittie Hafsah Panambulan LiwalugNo ratings yet
- Test 13 Ngay 7-5-21-HSDocument6 pagesTest 13 Ngay 7-5-21-HSThảo Phương NguyễnNo ratings yet
- ABM Relactation BreastfeedingDocument2 pagesABM Relactation Breastfeedingdragomir_emilia92No ratings yet
- The Winepress - Lectura 1Document13 pagesThe Winepress - Lectura 1Diego Ernesto Gómez TrujilloNo ratings yet
- Mediterranean Diet GuideDocument8 pagesMediterranean Diet Guideama00100% (1)
- Avdenio Lexicon (Sorted)Document62 pagesAvdenio Lexicon (Sorted)api-288750682No ratings yet
- Repaso 3 EvalDocument23 pagesRepaso 3 Evalcarmen reyesNo ratings yet
- Dining PresentationDocument34 pagesDining PresentationAnonymous y3E7ia100% (1)
- RempeyekDocument7 pagesRempeyekelyasliaNo ratings yet
- 1 ADocument23 pages1 ANour AbuMeteirNo ratings yet
- Unidad 5Document17 pagesUnidad 5Carlos RedrovánNo ratings yet