
Renal Perfusion Index Reflects Cardiac Systolic Function in Chronic Cardio-Renal Syndrome
Renal Perfusion Index Reflects Cardiac Systolic Function in Chronic Cardio-Renal Syndrome
You might also like
- Jeet Selal Diet PlanDocument10 pagesJeet Selal Diet PlanSiddharth Chaudhary67% (3)
- Case Study On Stroke PatientDocument2 pagesCase Study On Stroke PatientsparrowcrowNo ratings yet
- Congestive Nephropathy: A Neglected Entity? Proposal For Diagnostic Criteria and Future PerspectivesDocument21 pagesCongestive Nephropathy: A Neglected Entity? Proposal For Diagnostic Criteria and Future PerspectivesMuhammad SyammNo ratings yet
- Nefropatia Congestiva 21Document21 pagesNefropatia Congestiva 21John Wesley BragaNo ratings yet
- Trpkov 2021Document31 pagesTrpkov 2021Meli O'NeilNo ratings yet
- Cardiorenal SyndromeDocument18 pagesCardiorenal Syndromedauz3017No ratings yet
- Cardiorenal SyndromeDocument13 pagesCardiorenal Syndromenisa_kartikaNo ratings yet
- Renal Doppler To Assess Renal Perfusion in The Critically Ill: A ReappraisalDocument10 pagesRenal Doppler To Assess Renal Perfusion in The Critically Ill: A ReappraisalFlávio AlvesNo ratings yet
- Management of ch. heart failurein DialysisDocument23 pagesManagement of ch. heart failurein DialysisSa7arNo ratings yet
- Long-Term Outcomes of Lercanidipine Versus Other Calcium Channel Blockers in Newly Diagnosed Hypertension: A Nationwide Cohort StudyDocument8 pagesLong-Term Outcomes of Lercanidipine Versus Other Calcium Channel Blockers in Newly Diagnosed Hypertension: A Nationwide Cohort StudyApt. Mulyadi PrasetyoNo ratings yet
- Journal 7Document8 pagesJournal 7Claudia JessicaNo ratings yet
- Grant2014 PDFDocument10 pagesGrant2014 PDFRalucaNo ratings yet
- 510732Document13 pages510732PaulHerreraNo ratings yet
- Assessment of Operability of Patients With Pulmonary Arterial Hypertension Associated With Congenital Heart DiseaseDocument8 pagesAssessment of Operability of Patients With Pulmonary Arterial Hypertension Associated With Congenital Heart DiseaseWulan AviantoroNo ratings yet
- Clinical Cardiology - 2022 - Liang - Prognostic Value of RDW Alone and in Combination With NT proBNP in Patients With HeartDocument13 pagesClinical Cardiology - 2022 - Liang - Prognostic Value of RDW Alone and in Combination With NT proBNP in Patients With Heartrizkiyah prabawantiNo ratings yet
- Nikhil Thesis AbstractDocument28 pagesNikhil Thesis AbstractNikhil KalasareNo ratings yet
- Non-Invasive Tools For Compensate D Advance D Chronic Liver Disease and Portal Hypertension After Baveno VII - An UpdateDocument10 pagesNon-Invasive Tools For Compensate D Advance D Chronic Liver Disease and Portal Hypertension After Baveno VII - An UpdateValentina IorgaNo ratings yet
- SRC JurDocument7 pagesSRC JurdwiNo ratings yet
- Symptom Burden in Patients With Chronic Kidney Disease Not Requiring Renal Replacement TherapyDocument9 pagesSymptom Burden in Patients With Chronic Kidney Disease Not Requiring Renal Replacement TherapyKarito FloresNo ratings yet
- Treatment of Acute Kidney InjuryDocument18 pagesTreatment of Acute Kidney Injuryqayyum consultantfpscNo ratings yet
- Diastolic Function Is A Strong Predictor of Mortality in Patients With Chronic Kidney DiseaseDocument6 pagesDiastolic Function Is A Strong Predictor of Mortality in Patients With Chronic Kidney DiseasehanifahrafaNo ratings yet
- 828 FullDocument7 pages828 FullMayra LoeraNo ratings yet
- Sfad 101Document14 pagesSfad 101el himawatiNo ratings yet
- 082 - EIJ D 23 00836 - LauderDocument12 pages082 - EIJ D 23 00836 - LauderFrancisco Javier Robles OrtizNo ratings yet
- By DR - Vasudeva Chetty PakalaDocument97 pagesBy DR - Vasudeva Chetty Pakalaace forumNo ratings yet
- Ischemic Nephropathy - Detection and Therapeutic InterventionDocument6 pagesIschemic Nephropathy - Detection and Therapeutic InterventionfransiskaNo ratings yet
- Meghan E.Document11 pagesMeghan E.Dr. Jatin GargNo ratings yet
- Beloncle Et Al Determinants of RRI Impact On Hemodynamic Parameter, AKI and Predisposing FactorsDocument8 pagesBeloncle Et Al Determinants of RRI Impact On Hemodynamic Parameter, AKI and Predisposing FactorsBijay KCNo ratings yet
- Managing Acute Presentations of Atheromatous Renal Artery StenosisDocument9 pagesManaging Acute Presentations of Atheromatous Renal Artery StenosisDana MNo ratings yet
- CKD HT 2Document7 pagesCKD HT 2Peer TutorNo ratings yet
- Eco en SD CardiorenalDocument20 pagesEco en SD Cardiorenaladela pintoNo ratings yet
- Septic CardiomyopathyDocument13 pagesSeptic CardiomyopathyPedro MatosNo ratings yet
- Rapid Access Cardiology-A Nine Year ReviewDocument5 pagesRapid Access Cardiology-A Nine Year Reviewdr.ghassanaboudNo ratings yet
- ESC Heart Failure - 2020 - Jobs - Inferior Vena Cava Ultrasound in Acute Decompensated Heart Failure Design Rationale ofDocument11 pagesESC Heart Failure - 2020 - Jobs - Inferior Vena Cava Ultrasound in Acute Decompensated Heart Failure Design Rationale ofDINDA PUTRI SAVIRANo ratings yet
- Wa0099.Document12 pagesWa0099.GdfgdFdfdfNo ratings yet
- Assosiated RBC and NafldDocument14 pagesAssosiated RBC and NafldDr. Fitri1919No ratings yet
- Cardiorenal Syndrome: SciencedirectDocument10 pagesCardiorenal Syndrome: SciencedirectDwiFitriaAnggrainiNo ratings yet
- The Role of Echocardiographic Study in Patients With Chronic Kidney DiseaseDocument9 pagesThe Role of Echocardiographic Study in Patients With Chronic Kidney DiseaseshodhgangaNo ratings yet
- Association of High Blood Pressure With RenalDocument6 pagesAssociation of High Blood Pressure With RenalBima AryaputraNo ratings yet
- Review Article: The Cardiorenal Syndrome: A ReviewDocument11 pagesReview Article: The Cardiorenal Syndrome: A ReviewrezykurniaNo ratings yet
- CKD Risk FactorsDocument14 pagesCKD Risk FactorsSrinivas PingaliNo ratings yet
- Atm 09 20 1587Document14 pagesAtm 09 20 1587Wina Pertiwi 2003113414No ratings yet
- Epidemiology and Risk Factors in CKD Patients With Pulmonary HypertensionDocument8 pagesEpidemiology and Risk Factors in CKD Patients With Pulmonary HypertensionshaheershayanqaziNo ratings yet
- Fmed 08 817758Document5 pagesFmed 08 817758Mawardi SahirNo ratings yet
- Ejhf 2664Document16 pagesEjhf 2664GdfgdFdfdfNo ratings yet
- PeripheralDocument7 pagesPeripheralerdynNo ratings yet
- Articulo2 ProyectoDocument12 pagesArticulo2 ProyectoIsabella Pinto CorzoNo ratings yet
- Panitchote2019 Article FactorsAssociatedWithAcuteKidnDocument10 pagesPanitchote2019 Article FactorsAssociatedWithAcuteKidnBernard NazaraNo ratings yet
- Hemodynamic Indices in Pulmonary Hypertension: A Narrative ReviewDocument15 pagesHemodynamic Indices in Pulmonary Hypertension: A Narrative ReviewfabiolaNo ratings yet
- 2014 Journal - Patient With Congenital Systemic To Pulmonary Shunts and Increased Pulmonary Vascular ResistanceDocument7 pages2014 Journal - Patient With Congenital Systemic To Pulmonary Shunts and Increased Pulmonary Vascular ResistanceAryfKurniawanNo ratings yet
- European J of Heart Fail - 2010 - Gheorghiade - Assessing and Grading Congestion in Acute Heart Failure A ScientificDocument11 pagesEuropean J of Heart Fail - 2010 - Gheorghiade - Assessing and Grading Congestion in Acute Heart Failure A ScientificVlad RusuNo ratings yet
- High Ultrafiltration Rate Induced Intradialytic Hypotension Is A Predictor For Cardiac Remodeling A 5-Year Cohort StudyDocument10 pagesHigh Ultrafiltration Rate Induced Intradialytic Hypotension Is A Predictor For Cardiac Remodeling A 5-Year Cohort StudyfabiolaNo ratings yet
- Narrative Review: Pulmonary Hypertension in CKDDocument11 pagesNarrative Review: Pulmonary Hypertension in CKDDr. Jatin GargNo ratings yet
- Articol Na TisularDocument10 pagesArticol Na TisularAndra-Elena ObrejaNo ratings yet
- JreadDocument1 pageJreadAiraa ShaneNo ratings yet
- International Journal of Cardiology: SciencedirectDocument8 pagesInternational Journal of Cardiology: SciencedirectsarahNo ratings yet
- Accepted Manuscript: Journal of HepatologyDocument45 pagesAccepted Manuscript: Journal of HepatologyLuis Enrique Caceres AlavrezNo ratings yet
- Ehf2 13044Document9 pagesEhf2 13044re septian IlhamsyahNo ratings yet
- KDIGO Blood Pressure Conference Scope of Work Public ReviewDocument7 pagesKDIGO Blood Pressure Conference Scope of Work Public ReviewYulia SyarifaNo ratings yet
- Kidney Size and Cortical Thickness KI 2002Document8 pagesKidney Size and Cortical Thickness KI 2002Sundar RamanathanNo ratings yet
- 5g-Tantangan Terapi HF & COPDDocument6 pages5g-Tantangan Terapi HF & COPDsukiyantoNo ratings yet
- Evidence-Based NephrologyFrom EverandEvidence-Based NephrologyDonald A. Molony, M.D.No ratings yet
- The Essential Guide To Fat Loss Phil DaviesDocument61 pagesThe Essential Guide To Fat Loss Phil DaviesmaryjaybeeNo ratings yet
- Health Benefits of Playing BadmintonDocument6 pagesHealth Benefits of Playing BadmintonkencghNo ratings yet
- 8 JunkfoodDocument10 pages8 JunkfoodLuminitaNo ratings yet
- Ch22 HeartDocument65 pagesCh22 HeartC Bala Diwakesh100% (4)
- Nutrition Throughout The Life CycleDocument87 pagesNutrition Throughout The Life Cyclealsuwaidi5No ratings yet
- Adjectives AdverbsDocument15 pagesAdjectives AdverbsFrancisco Antonio López RevellesNo ratings yet
- Minimum Residue DietDocument1 pageMinimum Residue DietyulisesNo ratings yet
- TAN Assignment BDocument11 pagesTAN Assignment BBea TanNo ratings yet
- Obesity and PregnancyDocument4 pagesObesity and PregnancyRL FlacamaNo ratings yet
- Dieta 2 SemanasDocument2 pagesDieta 2 SemanasAndrey CaroNo ratings yet
- 3950 6002 1 PBDocument9 pages3950 6002 1 PBAhmed SaeedNo ratings yet
- Hydrogenation of Vegetable OilsDocument7 pagesHydrogenation of Vegetable OilsKroya HunNo ratings yet
- Carbohydrate MetabolismDocument30 pagesCarbohydrate MetabolismHafsahNo ratings yet
- Fiit Principle and Workout - Hed 1Document4 pagesFiit Principle and Workout - Hed 1api-357269544No ratings yet
- 187 - Hilmy Abyan - Critical AppraisalDocument6 pages187 - Hilmy Abyan - Critical Appraisalnona diniNo ratings yet
- Chemistry Investigatory Project ON: Study of Quantity of Casein Present in Different Samples of MilkDocument12 pagesChemistry Investigatory Project ON: Study of Quantity of Casein Present in Different Samples of Milkanand katre0% (1)
- Maam Rosalie H. Lim 2018 Newly Edited 3 4 5 Etc.Document8 pagesMaam Rosalie H. Lim 2018 Newly Edited 3 4 5 Etc.EmanoAceNo ratings yet
- 4 Gi Hormones I: Endocrine HormonesDocument4 pages4 Gi Hormones I: Endocrine HormonesLinh PhanNo ratings yet
- School Form 8 (11-HUMSS A)Document2 pagesSchool Form 8 (11-HUMSS A)CHARLENE SAGUINHONNo ratings yet
- Nursing Management/Intervention For Ecclampsia, Preeclampsia, PIH.Document11 pagesNursing Management/Intervention For Ecclampsia, Preeclampsia, PIH.KathNo ratings yet
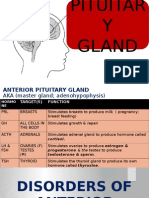
- Disorders of Pituitary GlandDocument34 pagesDisorders of Pituitary GlandninaaltheaNo ratings yet
- Force RECONDocument8 pagesForce RECONYasser E Kasan100% (1)
- FastingDocument21 pagesFastingtpau6272100% (1)
- Chem 31.1 Unknown Analysis Cheat SheetDocument2 pagesChem 31.1 Unknown Analysis Cheat Sheetฝน เมนโดซาNo ratings yet
- 2018-09-01 MuscleFitness Hers PDFDocument100 pages2018-09-01 MuscleFitness Hers PDFMonica Stibli100% (1)
- HeartDocument72 pagesHeartfyzanfroshie100% (1)
- Osteoporosis: Davin PannaaustenDocument23 pagesOsteoporosis: Davin PannaaustenDavinPannaaustenNo ratings yet
- Prepared By: Group 7Document41 pagesPrepared By: Group 7Ehm Zhy NhelNo ratings yet























































































Download as pdf or txt
You might also like
- Jeet Selal Diet PlanDocument10 pagesJeet Selal Diet PlanSiddharth Chaudhary67% (3)
- Case Study On Stroke PatientDocument2 pagesCase Study On Stroke PatientsparrowcrowNo ratings yet
- Congestive Nephropathy: A Neglected Entity? Proposal For Diagnostic Criteria and Future PerspectivesDocument21 pagesCongestive Nephropathy: A Neglected Entity? Proposal For Diagnostic Criteria and Future PerspectivesMuhammad SyammNo ratings yet
- Nefropatia Congestiva 21Document21 pagesNefropatia Congestiva 21John Wesley BragaNo ratings yet
- Trpkov 2021Document31 pagesTrpkov 2021Meli O'NeilNo ratings yet
- Cardiorenal SyndromeDocument18 pagesCardiorenal Syndromedauz3017No ratings yet
- Cardiorenal SyndromeDocument13 pagesCardiorenal Syndromenisa_kartikaNo ratings yet
- Renal Doppler To Assess Renal Perfusion in The Critically Ill: A ReappraisalDocument10 pagesRenal Doppler To Assess Renal Perfusion in The Critically Ill: A ReappraisalFlávio AlvesNo ratings yet
- Management of ch. heart failurein DialysisDocument23 pagesManagement of ch. heart failurein DialysisSa7arNo ratings yet
- Long-Term Outcomes of Lercanidipine Versus Other Calcium Channel Blockers in Newly Diagnosed Hypertension: A Nationwide Cohort StudyDocument8 pagesLong-Term Outcomes of Lercanidipine Versus Other Calcium Channel Blockers in Newly Diagnosed Hypertension: A Nationwide Cohort StudyApt. Mulyadi PrasetyoNo ratings yet
- Journal 7Document8 pagesJournal 7Claudia JessicaNo ratings yet
- Grant2014 PDFDocument10 pagesGrant2014 PDFRalucaNo ratings yet
- 510732Document13 pages510732PaulHerreraNo ratings yet
- Assessment of Operability of Patients With Pulmonary Arterial Hypertension Associated With Congenital Heart DiseaseDocument8 pagesAssessment of Operability of Patients With Pulmonary Arterial Hypertension Associated With Congenital Heart DiseaseWulan AviantoroNo ratings yet
- Clinical Cardiology - 2022 - Liang - Prognostic Value of RDW Alone and in Combination With NT proBNP in Patients With HeartDocument13 pagesClinical Cardiology - 2022 - Liang - Prognostic Value of RDW Alone and in Combination With NT proBNP in Patients With Heartrizkiyah prabawantiNo ratings yet
- Nikhil Thesis AbstractDocument28 pagesNikhil Thesis AbstractNikhil KalasareNo ratings yet
- Non-Invasive Tools For Compensate D Advance D Chronic Liver Disease and Portal Hypertension After Baveno VII - An UpdateDocument10 pagesNon-Invasive Tools For Compensate D Advance D Chronic Liver Disease and Portal Hypertension After Baveno VII - An UpdateValentina IorgaNo ratings yet
- SRC JurDocument7 pagesSRC JurdwiNo ratings yet
- Symptom Burden in Patients With Chronic Kidney Disease Not Requiring Renal Replacement TherapyDocument9 pagesSymptom Burden in Patients With Chronic Kidney Disease Not Requiring Renal Replacement TherapyKarito FloresNo ratings yet
- Treatment of Acute Kidney InjuryDocument18 pagesTreatment of Acute Kidney Injuryqayyum consultantfpscNo ratings yet
- Diastolic Function Is A Strong Predictor of Mortality in Patients With Chronic Kidney DiseaseDocument6 pagesDiastolic Function Is A Strong Predictor of Mortality in Patients With Chronic Kidney DiseasehanifahrafaNo ratings yet
- 828 FullDocument7 pages828 FullMayra LoeraNo ratings yet
- Sfad 101Document14 pagesSfad 101el himawatiNo ratings yet
- 082 - EIJ D 23 00836 - LauderDocument12 pages082 - EIJ D 23 00836 - LauderFrancisco Javier Robles OrtizNo ratings yet
- By DR - Vasudeva Chetty PakalaDocument97 pagesBy DR - Vasudeva Chetty Pakalaace forumNo ratings yet
- Ischemic Nephropathy - Detection and Therapeutic InterventionDocument6 pagesIschemic Nephropathy - Detection and Therapeutic InterventionfransiskaNo ratings yet
- Meghan E.Document11 pagesMeghan E.Dr. Jatin GargNo ratings yet
- Beloncle Et Al Determinants of RRI Impact On Hemodynamic Parameter, AKI and Predisposing FactorsDocument8 pagesBeloncle Et Al Determinants of RRI Impact On Hemodynamic Parameter, AKI and Predisposing FactorsBijay KCNo ratings yet
- Managing Acute Presentations of Atheromatous Renal Artery StenosisDocument9 pagesManaging Acute Presentations of Atheromatous Renal Artery StenosisDana MNo ratings yet
- CKD HT 2Document7 pagesCKD HT 2Peer TutorNo ratings yet
- Eco en SD CardiorenalDocument20 pagesEco en SD Cardiorenaladela pintoNo ratings yet
- Septic CardiomyopathyDocument13 pagesSeptic CardiomyopathyPedro MatosNo ratings yet
- Rapid Access Cardiology-A Nine Year ReviewDocument5 pagesRapid Access Cardiology-A Nine Year Reviewdr.ghassanaboudNo ratings yet
- ESC Heart Failure - 2020 - Jobs - Inferior Vena Cava Ultrasound in Acute Decompensated Heart Failure Design Rationale ofDocument11 pagesESC Heart Failure - 2020 - Jobs - Inferior Vena Cava Ultrasound in Acute Decompensated Heart Failure Design Rationale ofDINDA PUTRI SAVIRANo ratings yet
- Wa0099.Document12 pagesWa0099.GdfgdFdfdfNo ratings yet
- Assosiated RBC and NafldDocument14 pagesAssosiated RBC and NafldDr. Fitri1919No ratings yet
- Cardiorenal Syndrome: SciencedirectDocument10 pagesCardiorenal Syndrome: SciencedirectDwiFitriaAnggrainiNo ratings yet
- The Role of Echocardiographic Study in Patients With Chronic Kidney DiseaseDocument9 pagesThe Role of Echocardiographic Study in Patients With Chronic Kidney DiseaseshodhgangaNo ratings yet
- Association of High Blood Pressure With RenalDocument6 pagesAssociation of High Blood Pressure With RenalBima AryaputraNo ratings yet
- Review Article: The Cardiorenal Syndrome: A ReviewDocument11 pagesReview Article: The Cardiorenal Syndrome: A ReviewrezykurniaNo ratings yet
- CKD Risk FactorsDocument14 pagesCKD Risk FactorsSrinivas PingaliNo ratings yet
- Atm 09 20 1587Document14 pagesAtm 09 20 1587Wina Pertiwi 2003113414No ratings yet
- Epidemiology and Risk Factors in CKD Patients With Pulmonary HypertensionDocument8 pagesEpidemiology and Risk Factors in CKD Patients With Pulmonary HypertensionshaheershayanqaziNo ratings yet
- Fmed 08 817758Document5 pagesFmed 08 817758Mawardi SahirNo ratings yet
- Ejhf 2664Document16 pagesEjhf 2664GdfgdFdfdfNo ratings yet
- PeripheralDocument7 pagesPeripheralerdynNo ratings yet
- Articulo2 ProyectoDocument12 pagesArticulo2 ProyectoIsabella Pinto CorzoNo ratings yet
- Panitchote2019 Article FactorsAssociatedWithAcuteKidnDocument10 pagesPanitchote2019 Article FactorsAssociatedWithAcuteKidnBernard NazaraNo ratings yet
- Hemodynamic Indices in Pulmonary Hypertension: A Narrative ReviewDocument15 pagesHemodynamic Indices in Pulmonary Hypertension: A Narrative ReviewfabiolaNo ratings yet
- 2014 Journal - Patient With Congenital Systemic To Pulmonary Shunts and Increased Pulmonary Vascular ResistanceDocument7 pages2014 Journal - Patient With Congenital Systemic To Pulmonary Shunts and Increased Pulmonary Vascular ResistanceAryfKurniawanNo ratings yet
- European J of Heart Fail - 2010 - Gheorghiade - Assessing and Grading Congestion in Acute Heart Failure A ScientificDocument11 pagesEuropean J of Heart Fail - 2010 - Gheorghiade - Assessing and Grading Congestion in Acute Heart Failure A ScientificVlad RusuNo ratings yet
- High Ultrafiltration Rate Induced Intradialytic Hypotension Is A Predictor For Cardiac Remodeling A 5-Year Cohort StudyDocument10 pagesHigh Ultrafiltration Rate Induced Intradialytic Hypotension Is A Predictor For Cardiac Remodeling A 5-Year Cohort StudyfabiolaNo ratings yet
- Narrative Review: Pulmonary Hypertension in CKDDocument11 pagesNarrative Review: Pulmonary Hypertension in CKDDr. Jatin GargNo ratings yet
- Articol Na TisularDocument10 pagesArticol Na TisularAndra-Elena ObrejaNo ratings yet
- JreadDocument1 pageJreadAiraa ShaneNo ratings yet
- International Journal of Cardiology: SciencedirectDocument8 pagesInternational Journal of Cardiology: SciencedirectsarahNo ratings yet
- Accepted Manuscript: Journal of HepatologyDocument45 pagesAccepted Manuscript: Journal of HepatologyLuis Enrique Caceres AlavrezNo ratings yet
- Ehf2 13044Document9 pagesEhf2 13044re septian IlhamsyahNo ratings yet
- KDIGO Blood Pressure Conference Scope of Work Public ReviewDocument7 pagesKDIGO Blood Pressure Conference Scope of Work Public ReviewYulia SyarifaNo ratings yet
- Kidney Size and Cortical Thickness KI 2002Document8 pagesKidney Size and Cortical Thickness KI 2002Sundar RamanathanNo ratings yet
- 5g-Tantangan Terapi HF & COPDDocument6 pages5g-Tantangan Terapi HF & COPDsukiyantoNo ratings yet
- Evidence-Based NephrologyFrom EverandEvidence-Based NephrologyDonald A. Molony, M.D.No ratings yet
- The Essential Guide To Fat Loss Phil DaviesDocument61 pagesThe Essential Guide To Fat Loss Phil DaviesmaryjaybeeNo ratings yet
- Health Benefits of Playing BadmintonDocument6 pagesHealth Benefits of Playing BadmintonkencghNo ratings yet
- 8 JunkfoodDocument10 pages8 JunkfoodLuminitaNo ratings yet
- Ch22 HeartDocument65 pagesCh22 HeartC Bala Diwakesh100% (4)
- Nutrition Throughout The Life CycleDocument87 pagesNutrition Throughout The Life Cyclealsuwaidi5No ratings yet
- Adjectives AdverbsDocument15 pagesAdjectives AdverbsFrancisco Antonio López RevellesNo ratings yet
- Minimum Residue DietDocument1 pageMinimum Residue DietyulisesNo ratings yet
- TAN Assignment BDocument11 pagesTAN Assignment BBea TanNo ratings yet
- Obesity and PregnancyDocument4 pagesObesity and PregnancyRL FlacamaNo ratings yet
- Dieta 2 SemanasDocument2 pagesDieta 2 SemanasAndrey CaroNo ratings yet
- 3950 6002 1 PBDocument9 pages3950 6002 1 PBAhmed SaeedNo ratings yet
- Hydrogenation of Vegetable OilsDocument7 pagesHydrogenation of Vegetable OilsKroya HunNo ratings yet
- Carbohydrate MetabolismDocument30 pagesCarbohydrate MetabolismHafsahNo ratings yet
- Fiit Principle and Workout - Hed 1Document4 pagesFiit Principle and Workout - Hed 1api-357269544No ratings yet
- 187 - Hilmy Abyan - Critical AppraisalDocument6 pages187 - Hilmy Abyan - Critical Appraisalnona diniNo ratings yet
- Chemistry Investigatory Project ON: Study of Quantity of Casein Present in Different Samples of MilkDocument12 pagesChemistry Investigatory Project ON: Study of Quantity of Casein Present in Different Samples of Milkanand katre0% (1)
- Maam Rosalie H. Lim 2018 Newly Edited 3 4 5 Etc.Document8 pagesMaam Rosalie H. Lim 2018 Newly Edited 3 4 5 Etc.EmanoAceNo ratings yet
- 4 Gi Hormones I: Endocrine HormonesDocument4 pages4 Gi Hormones I: Endocrine HormonesLinh PhanNo ratings yet
- School Form 8 (11-HUMSS A)Document2 pagesSchool Form 8 (11-HUMSS A)CHARLENE SAGUINHONNo ratings yet
- Nursing Management/Intervention For Ecclampsia, Preeclampsia, PIH.Document11 pagesNursing Management/Intervention For Ecclampsia, Preeclampsia, PIH.KathNo ratings yet
- Disorders of Pituitary GlandDocument34 pagesDisorders of Pituitary GlandninaaltheaNo ratings yet
- Force RECONDocument8 pagesForce RECONYasser E Kasan100% (1)
- FastingDocument21 pagesFastingtpau6272100% (1)
- Chem 31.1 Unknown Analysis Cheat SheetDocument2 pagesChem 31.1 Unknown Analysis Cheat Sheetฝน เมนโดซาNo ratings yet
- 2018-09-01 MuscleFitness Hers PDFDocument100 pages2018-09-01 MuscleFitness Hers PDFMonica Stibli100% (1)
- HeartDocument72 pagesHeartfyzanfroshie100% (1)
- Osteoporosis: Davin PannaaustenDocument23 pagesOsteoporosis: Davin PannaaustenDavinPannaaustenNo ratings yet
- Prepared By: Group 7Document41 pagesPrepared By: Group 7Ehm Zhy NhelNo ratings yet