Download as pdf or txt
You might also like
- Detailed Lesson Plan in English Grade 9Document5 pagesDetailed Lesson Plan in English Grade 9Dayhen Afable Bianes83% (35)
- Verbal Fluency Test (FAS Test) InstructionsDocument1 pageVerbal Fluency Test (FAS Test) InstructionsJoNo ratings yet
- DEM Test NotesDocument6 pagesDEM Test NotesJoão CunhaNo ratings yet
- ( (#Ve?@ (2 ( (#Ve?@ (G ( (#Ve?@ (M (R6 (,cbwxcd@yz (KG54GN ( (V/6L (Document1 page( (#Ve?@ (2 ( (#Ve?@ (G ( (#Ve?@ (M (R6 (,cbwxcd@yz (KG54GN ( (V/6L (Ramiro ReckziegelNo ratings yet
- Ravlt 2010 PDFDocument7 pagesRavlt 2010 PDFPriscila KleinNo ratings yet
- PIIS0003999311009725 Programa de Terapia de McNeill PDFDocument6 pagesPIIS0003999311009725 Programa de Terapia de McNeill PDFAngelica Maria LizarazoNo ratings yet
- Daily Grammar Warm-UpsDocument200 pagesDaily Grammar Warm-Upsapi-30486095475% (4)
- Norms For CERAD Constructional Praxis RecallDocument17 pagesNorms For CERAD Constructional Praxis RecallTeuku Ona AriefNo ratings yet
- Tablas ChileDocument11 pagesTablas ChileShannon GuerraNo ratings yet
- Laminas Test de BostonDocument27 pagesLaminas Test de BostonKarla Garcia CancinoNo ratings yet
- HVLT InstructionsDocument2 pagesHVLT InstructionsJoNo ratings yet
- Dislexia FonológicaDocument9 pagesDislexia FonológicaBrenda BorgesNo ratings yet
- Blue Dye TestDocument9 pagesBlue Dye TestMacarena Elizabeth Olavarría Gómez100% (1)
- DSM-5 Adult ADHD Checklist - Self-Report: January 2021Document2 pagesDSM-5 Adult ADHD Checklist - Self-Report: January 2021Sandy KOLBASINo ratings yet
- Malloy Diniz Et Al. 2007 PDFDocument7 pagesMalloy Diniz Et Al. 2007 PDFHectorNo ratings yet
- EpiTrack Tracking Cognitive Side Effects of Medication On AttentionDocument7 pagesEpiTrack Tracking Cognitive Side Effects of Medication On AttentionGonzalo GVNo ratings yet
- Lasker, Garret, Fox (2007)Document9 pagesLasker, Garret, Fox (2007)Lorenzo Nifto AmmàrNo ratings yet
- School-Age Form: Ages 4 To 18 YearsDocument2 pagesSchool-Age Form: Ages 4 To 18 YearsMarmtt MarmotaNo ratings yet
- Teste Faux PasDocument5 pagesTeste Faux PasAdriano FerrazNo ratings yet
- Protocolo WisconsinDocument2 pagesProtocolo WisconsinSofiaPsicopedagogaNo ratings yet
- MDADIDocument3 pagesMDADIKhumaira SantaNo ratings yet
- Re STDocument18 pagesRe STMaritzashuNo ratings yet
- 1508 Orofacial Muscle Tone & Strength Across The Dysarthrias (PDFDrive)Document97 pages1508 Orofacial Muscle Tone & Strength Across The Dysarthrias (PDFDrive)Földesi Borhi Noémi100% (1)
- Neuropsychological Assessment of Cultrually and Linguistically DiDocument24 pagesNeuropsychological Assessment of Cultrually and Linguistically DiphodoraNo ratings yet
- Restart DCM - Method. EnglishDocument35 pagesRestart DCM - Method. EnglishMinkushNo ratings yet
- Minimental ParkinsonDocument9 pagesMinimental ParkinsondquebradasNo ratings yet
- Moca Test Spanish PDFDocument1 pageMoca Test Spanish PDFMaria Constanza BahamondeNo ratings yet
- Edith Kaplan and The Boston Process Approach Libon2013Document13 pagesEdith Kaplan and The Boston Process Approach Libon2013MiguelySusy Ramos-RojasNo ratings yet
- Baremos TMTDocument21 pagesBaremos TMTAntonio J. LópezNo ratings yet
- Fas InglesDocument54 pagesFas Inglescgalain100% (2)
- BVMT-R - Sample Report - PiCDocument5 pagesBVMT-R - Sample Report - PiCCesarNo ratings yet
- PASAT Norms For The Portuguese PopulationDocument8 pagesPASAT Norms For The Portuguese PopulationMarília RodriguesNo ratings yet
- Speech-Language Pathology Rehabilitation of Oropharyngeal Dysphagia After Stroke: Literature of ReviewDocument11 pagesSpeech-Language Pathology Rehabilitation of Oropharyngeal Dysphagia After Stroke: Literature of ReviewFonoaudiologiaNo ratings yet
- Teddy BearDocument6 pagesTeddy BearPâmela MuchaNo ratings yet
- D KEFSStroopasPVT2018 PDFDocument14 pagesD KEFSStroopasPVT2018 PDFvictorpsycheNo ratings yet
- Recomendacoes em Alzheimer PDFDocument108 pagesRecomendacoes em Alzheimer PDFreneverasNo ratings yet
- TDL CataliseDocument13 pagesTDL CataliseNinoska OrtizNo ratings yet
- BORBDocument26 pagesBORBJapneet KaurNo ratings yet
- Rey-Auditory Verbal Learning Test (RAVLT, Wordlist 2) - English VersionDocument3 pagesRey-Auditory Verbal Learning Test (RAVLT, Wordlist 2) - English VersionRamees AhamadNo ratings yet
- VitalStim Electrode Placement GuideDocument1 pageVitalStim Electrode Placement GuideMd Sherajul HaqueNo ratings yet
- Galveston Orientation and Amnesia Test GOATDocument4 pagesGalveston Orientation and Amnesia Test GOATSuhana PathanNo ratings yet
- Ravlt: Males: Mean (SD) Number of Words Recalled and Recognized According To Age and TrialDocument2 pagesRavlt: Males: Mean (SD) Number of Words Recalled and Recognized According To Age and TrialPaula Calderon100% (2)
- Trail Making Test: Regression-Based Norms For The Portuguese PopulationDocument10 pagesTrail Making Test: Regression-Based Norms For The Portuguese PopulationPotenciar teNo ratings yet
- Test de WisconsinDocument25 pagesTest de WisconsinFrancisco WattNo ratings yet
- Habla ClaraDocument14 pagesHabla ClaraCristóbal Landeros TorresNo ratings yet
- Evaluating and Treating Communication and Cognitive Disorders - Approaches To Referral and Collaboration For Speech-Language Pathology and Clinical NeuropsychologyDocument16 pagesEvaluating and Treating Communication and Cognitive Disorders - Approaches To Referral and Collaboration For Speech-Language Pathology and Clinical Neuropsychologyluribe662No ratings yet
- Repeat and Point Revised Test FormDocument1 pageRepeat and Point Revised Test FormdrmssNo ratings yet
- Neuronorma 2 Spans LNS TMT SDMTDocument15 pagesNeuronorma 2 Spans LNS TMT SDMTJose Algomas KnorecuerdoNo ratings yet
- Celf 2 Pre School 2 Folleto de RegistroDocument29 pagesCelf 2 Pre School 2 Folleto de RegistroMaría Laura InsaustiNo ratings yet
- CommunicationDocument1 pageCommunicationapi-352507025No ratings yet
- Trail Making Test: Normative Data For The Latin American Spanish-Speaking Pediatric PopulationDocument37 pagesTrail Making Test: Normative Data For The Latin American Spanish-Speaking Pediatric Populationeimy.pulecio urosarioNo ratings yet
- Lingual Frenulum Changes After FrenectomyDocument5 pagesLingual Frenulum Changes After Frenectomyiradatullah suyutiNo ratings yet
- Fonema SDocument30 pagesFonema SNatalia VélezNo ratings yet
- Caring..Responsive..Well-Managed..We Are DHHSDocument2 pagesCaring..Responsive..Well-Managed..We Are DHHSNEWS CENTER MaineNo ratings yet
- Stuttering and Auditory Functions..pdf/ KUNNAMPALLIL GEJODocument90 pagesStuttering and Auditory Functions..pdf/ KUNNAMPALLIL GEJOKUNNAMPALLIL GEJO JOHNNo ratings yet
- The Reliability of The Neonatal Oral-Motor Assessment Scale: KeywordsDocument6 pagesThe Reliability of The Neonatal Oral-Motor Assessment Scale: KeywordsJosé Ignacio SepúlvedaNo ratings yet
- Boston-Token Neuronorma Mayores de 50Document12 pagesBoston-Token Neuronorma Mayores de 50Patricia Moreno OteroNo ratings yet
- AGNOSIAS - Resumen 1Document43 pagesAGNOSIAS - Resumen 1Katherine Betancur100% (3)
- Cap 13 - 1Document16 pagesCap 13 - 1Manuel VillagranNo ratings yet
- Hughlings-Jackson1878 - ON AFFECTIONS OF SPEECH FROM DISEASE OF THE BRAINDocument27 pagesHughlings-Jackson1878 - ON AFFECTIONS OF SPEECH FROM DISEASE OF THE BRAINErick SolisNo ratings yet
- AfasiaDocument23 pagesAfasiaAlexis A.No ratings yet
- The Epilepsy Aphasias: Landau Kleffner Syndrome and Rolandic EpilepsyFrom EverandThe Epilepsy Aphasias: Landau Kleffner Syndrome and Rolandic EpilepsyNo ratings yet
- 5th Grade Week 22 ElaDocument3 pages5th Grade Week 22 Elaapi-287852347No ratings yet
- 1 Clause Complexes ViviDocument26 pages1 Clause Complexes ViviEnDang SakinahNo ratings yet
- Simple Present Story 1 PDFDocument7 pagesSimple Present Story 1 PDFMaya Ernie83% (6)
- Sentence Diagramming Adjectives Adverbs ArticlesDocument2 pagesSentence Diagramming Adjectives Adverbs ArticlesrowenimaryNo ratings yet
- Future TenseDocument9 pagesFuture TenseNida AmmarNo ratings yet
- Cohesive Explicitness and Explicitation in An English-German Translation CorpusDocument25 pagesCohesive Explicitness and Explicitation in An English-German Translation CorpusWaleed OthmanNo ratings yet
- Passive VoiceDocument16 pagesPassive Voicenikee_shieNo ratings yet
- SyntaxDocument25 pagesSyntaxBieya SabiraNo ratings yet
- Natural Language ProcessingDocument57 pagesNatural Language Processingআশফাকুর রহমান আরজুNo ratings yet
- Final ENGLISH-SUBJECTDocument5 pagesFinal ENGLISH-SUBJECTbernsNo ratings yet
- ArticlesDocument2 pagesArticlesuser160496No ratings yet
- English For Translation Class2 Module2&3 (20120916)Document23 pagesEnglish For Translation Class2 Module2&3 (20120916)api-262694358No ratings yet
- Common Sentence Problems..9999999Document18 pagesCommon Sentence Problems..9999999SusanaNo ratings yet
- 2006 Narrative PreconstructionDocument10 pages2006 Narrative PreconstructionJe S BeNo ratings yet
- Conditional PPDocument10 pagesConditional PPDoctoraHolderNo ratings yet
- Goodwon - The Mood and TensesDocument300 pagesGoodwon - The Mood and TensesMaruu RomanelliNo ratings yet
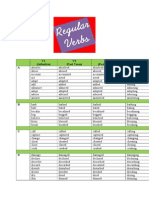
- V1 (Infinitive) V2 (Past Tense) V3 (Past Participle) V-Ing (Present Participle) ADocument5 pagesV1 (Infinitive) V2 (Past Tense) V3 (Past Participle) V-Ing (Present Participle) AJhon AritonangNo ratings yet
- Comparatives and Superlatives TestDocument3 pagesComparatives and Superlatives TestJuan Antonio Dominguez Arroyo50% (2)
- Simple Past and Present PerfectDocument10 pagesSimple Past and Present PerfectNur RudiyantoNo ratings yet
- Lesson Plan Reported SpeechDocument7 pagesLesson Plan Reported Speechaidawardhananti100% (1)
- Dutch Course 32 EditionN-KleinDocument66 pagesDutch Course 32 EditionN-KleinMurat Colakoglu100% (5)
- Adverb Clause PresentationDocument24 pagesAdverb Clause PresentationRieyukie Park 동방신기 Hwaiting0% (1)
- Practica de Intermedio 2Document4 pagesPractica de Intermedio 2joshe003No ratings yet
- GrammarDocument11 pagesGrammarPutri SundariNo ratings yet
- Accuplacer - Sentence StructureDocument25 pagesAccuplacer - Sentence StructureLaura Davenport0% (1)
- Planificare CalendaristicaDocument4 pagesPlanificare CalendaristicaDrozd AnamariaNo ratings yet
- Eng 100BC ClassificationandDivisionEssaysDocument51 pagesEng 100BC ClassificationandDivisionEssaysjeanninestankoNo ratings yet
- Exercises Unit 1: 1.1 Right or Wrong? Tick or Correct The SentencesDocument24 pagesExercises Unit 1: 1.1 Right or Wrong? Tick or Correct The SentencesBoris SegarraNo ratings yet