Download as pdf or txt
You might also like
- Focused Soap NoteDocument4 pagesFocused Soap Noteapi-24735887592% (13)
- ACT For Sleep Protocol-FinalDocument17 pagesACT For Sleep Protocol-Finalkenny.illanesNo ratings yet
- Select Your Remedy: by Rai Bahadur Bishambhar DasDocument534 pagesSelect Your Remedy: by Rai Bahadur Bishambhar Daslilian_vera_175% (4)
- Project ProposalDocument21 pagesProject Proposalfarhad khan100% (8)
- Community Engagement, Solidarity and CitizenshipDocument15 pagesCommunity Engagement, Solidarity and CitizenshipJoel Briones70% (10)
- Clinical Hypnosis For Smoking CessationDocument9 pagesClinical Hypnosis For Smoking Cessationamad90100% (1)
- Treatment and OutcomeDocument26 pagesTreatment and OutcomeChristine EnriquezNo ratings yet
- Treatment of Mood DisordersDocument27 pagesTreatment of Mood DisordersCamelutza IsaiNo ratings yet
- CBT Course AnswersDocument34 pagesCBT Course AnswersAvinash ShenoyNo ratings yet
- FINAL Overview - Evidence - Base - BriefingDocument11 pagesFINAL Overview - Evidence - Base - BriefingManuela MesquitaNo ratings yet
- Being The Other Therapist 2001Document14 pagesBeing The Other Therapist 2001malwinatmdNo ratings yet
- Analytical Hypnotherapy: A Beginner's 3-Step Quick Start Guide, with an FAQFrom EverandAnalytical Hypnotherapy: A Beginner's 3-Step Quick Start Guide, with an FAQNo ratings yet
- Analytical Hypnotherapy: A Beginner's 3-Step Quick Start Guide, with an FAQFrom EverandAnalytical Hypnotherapy: A Beginner's 3-Step Quick Start Guide, with an FAQNo ratings yet
- Pain Management Patient Defense BriefDocument6 pagesPain Management Patient Defense BriefAnonymous 2KoAxgiZJNo ratings yet
- Discuss Assessing The Effectiveness of One TreatmentDocument2 pagesDiscuss Assessing The Effectiveness of One TreatmentEmilia PiotrakNo ratings yet
- PsychotherapyDocument4 pagesPsychotherapyFaustrock Dionyso MingonkNo ratings yet
- Behavioral Activation Group Therapy: Therapist ManualDocument37 pagesBehavioral Activation Group Therapy: Therapist ManualcaballeroNo ratings yet
- Joaquín Andrade & David Feinstein - ENERGY PSYCHOLOGYDocument19 pagesJoaquín Andrade & David Feinstein - ENERGY PSYCHOLOGYlandburender100% (1)
- Why Do People Change Addictive BehaviorDocument10 pagesWhy Do People Change Addictive BehaviorGerson de la Fuente OlaveNo ratings yet
- Index: 22/8/14 1 Natural Happiness: The Truth About Exercise and DepressionDocument11 pagesIndex: 22/8/14 1 Natural Happiness: The Truth About Exercise and DepressionSiliconNo ratings yet
- For AbdiDocument75 pagesFor AbdiAb Staholic BoiiNo ratings yet
- Guía de Apa 2008 de TocDocument6 pagesGuía de Apa 2008 de TockarlunchoNo ratings yet
- Non-Pharmacological Treatments For Depression in Primary Care - An OverviewDocument8 pagesNon-Pharmacological Treatments For Depression in Primary Care - An OverviewknowlardNo ratings yet
- Back Pain May BeDocument9 pagesBack Pain May BeMano RajNo ratings yet
- Psychological Treatments of Schizophrenia CBT NotesDocument2 pagesPsychological Treatments of Schizophrenia CBT NotesQueen Bee (Tt)No ratings yet
- Tobacco Cessation Treatment PlanDocument7 pagesTobacco Cessation Treatment PlanyellowishmustardNo ratings yet
- The Coping MechanismsDocument3 pagesThe Coping MechanismsMIKI RULOMANo ratings yet
- Smoking Cessation: What Good Will Doctor's Advice Do?Document6 pagesSmoking Cessation: What Good Will Doctor's Advice Do?Getstop SmokingNo ratings yet
- Markowitz PPD IptDocument4 pagesMarkowitz PPD IptIoana BocaNo ratings yet
- Medications: Mental Health Medications Medication GuidesDocument3 pagesMedications: Mental Health Medications Medication GuidesVincent Paul SantosNo ratings yet
- Hypn AnalgDocument17 pagesHypn AnalgparaypanNo ratings yet
- Psychotropic MedicationsDocument87 pagesPsychotropic MedicationsDWAI McJohnsonNo ratings yet
- ACLM-Article-Avoidance of Risky SubstancesDocument3 pagesACLM-Article-Avoidance of Risky SubstancesMosiah Araújo SilvaNo ratings yet
- Cognitive Behavioral Therapy For DepressionDocument37 pagesCognitive Behavioral Therapy For DepressionP Neha100% (1)
- Contemporary Psychiatric Mental Health Nursing 3rd Edition Kneisl Solutions ManualDocument13 pagesContemporary Psychiatric Mental Health Nursing 3rd Edition Kneisl Solutions Manualphenicboxironicu9100% (29)
- Cognitive Behavioural Strategies For General PracticeDocument7 pagesCognitive Behavioural Strategies For General PracticeArturo MelgarNo ratings yet
- Project - Read Article and Answer QuestionsDocument4 pagesProject - Read Article and Answer QuestionsRazanrazaNo ratings yet
- Common Empirically Researched Substance Use Disorder TreatmentsDocument7 pagesCommon Empirically Researched Substance Use Disorder TreatmentsmainaNo ratings yet
- Placebo FinalDocument9 pagesPlacebo FinalRica Jane TorresNo ratings yet
- Alladin-Stages Hypnotherapy PDFDocument34 pagesAlladin-Stages Hypnotherapy PDFcarlammartinsNo ratings yet
- Communication SkillsDocument5 pagesCommunication SkillssanthoshNo ratings yet
- Effectiveness of Psychotherapeutic Treatment: Michael J. LambertDocument14 pagesEffectiveness of Psychotherapeutic Treatment: Michael J. LambertGerson De La FuenteNo ratings yet
- Planned Brief PsychotherapyDocument7 pagesPlanned Brief PsychotherapyRoci ArceNo ratings yet
- What Is Psychotherapy 15 Techniques and ExercisesDocument7 pagesWhat Is Psychotherapy 15 Techniques and ExercisesMihaela VădeanuNo ratings yet
- Treatment PlanDocument14 pagesTreatment Planharrieo100% (1)
- Andrade Feinstein PaperDocument26 pagesAndrade Feinstein PaperJulia PerellonNo ratings yet
- Healing through Psychotherapy: How to Mentally Heal & Beat Depression NaturallyFrom EverandHealing through Psychotherapy: How to Mentally Heal & Beat Depression NaturallyNo ratings yet
- Catalyzing The Therapeutic Proccess The Use of HypnosisDocument32 pagesCatalyzing The Therapeutic Proccess The Use of HypnosisZoita MandilaNo ratings yet
- Elkin Et AlDocument3 pagesElkin Et AlGabrysia MajsikNo ratings yet
- Beautiful Vibrations: Living through medical illness with Bach flower remediesFrom EverandBeautiful Vibrations: Living through medical illness with Bach flower remediesNo ratings yet
- Covert Assertion, SensitizationDocument5 pagesCovert Assertion, SensitizationFatima Malik100% (3)
- Basic Ericksonian Hypnosis EbookDocument155 pagesBasic Ericksonian Hypnosis EbookCristian PopNo ratings yet
- The Easiest Way to Stop Smoking: Finding the Way That Works Best for YouFrom EverandThe Easiest Way to Stop Smoking: Finding the Way That Works Best for YouNo ratings yet
- Addiction Recovery TreatmentDocument3 pagesAddiction Recovery TreatmentHenry09No ratings yet
- Journal CritiqueDocument5 pagesJournal CritiquesonicbebopNo ratings yet
- Holistic Healing: A Comprehensive Guide to Alternative TherapiesFrom EverandHolistic Healing: A Comprehensive Guide to Alternative TherapiesNo ratings yet
- Essay 3 Final RevisedDocument8 pagesEssay 3 Final Revisedapi-643399894No ratings yet
- Comprehensive Pain Rehabilitation Center: Program GuideDocument16 pagesComprehensive Pain Rehabilitation Center: Program Guideniko4eyesNo ratings yet
- Barkus-Suggestibility Dissociation Positive Schizotypy PDFDocument6 pagesBarkus-Suggestibility Dissociation Positive Schizotypy PDFClaudio Alonso MoyNo ratings yet
- Research On: Integrating Dissociation and HypnotizabilityDocument7 pagesResearch On: Integrating Dissociation and HypnotizabilityClaudio Alonso MoyNo ratings yet
- Barling-Experiential Analogies HypnotherapyDocument8 pagesBarling-Experiential Analogies HypnotherapyClaudio Alonso MoyNo ratings yet
- Anbar-User Friendly Hypnosis Adjunct Treatment Habit Cough PDFDocument5 pagesAnbar-User Friendly Hypnosis Adjunct Treatment Habit Cough PDFClaudio Alonso MoyNo ratings yet
- Clinical Hypnosis For Psychiatrists in Training: Psychiatric BulletinDocument3 pagesClinical Hypnosis For Psychiatrists in Training: Psychiatric BulletinClaudio Alonso MoyNo ratings yet
- Hypnosis Med201.001 Bluereview Posted Date: 3/23/2004 Effective Date: 7/1/2004Document3 pagesHypnosis Med201.001 Bluereview Posted Date: 3/23/2004 Effective Date: 7/1/2004Claudio Alonso MoyNo ratings yet
- Anbar-Self Hypnosis Management Chronic Dyspnea Pediatric PDFDocument6 pagesAnbar-Self Hypnosis Management Chronic Dyspnea Pediatric PDFClaudio Alonso MoyNo ratings yet
- Askay-Virtual Reality HypnosisDocument8 pagesAskay-Virtual Reality HypnosisClaudio Alonso MoyNo ratings yet
- Anbar-Childhood Habit Cough Treated Consultation Telephone PDFDocument3 pagesAnbar-Childhood Habit Cough Treated Consultation Telephone PDFClaudio Alonso MoyNo ratings yet
- Cloud NineDocument6 pagesCloud NineJunjun CaoliNo ratings yet
- TO 2 Literasi Bahasa InggrisDocument9 pagesTO 2 Literasi Bahasa InggrisDedi Maman100% (2)
- Shoulder DystociaDocument3 pagesShoulder Dystociakarl de guzmanNo ratings yet
- Unit IG2 - Risk Assessment: Chemical and Biological AgentsDocument53 pagesUnit IG2 - Risk Assessment: Chemical and Biological AgentsJithu RajuNo ratings yet
- 12.2 Guided ReadingDocument2 pages12.2 Guided ReadingGrant Hasleton100% (1)
- Version Structures and Functions of Living Organisms 8.L.1.1Document28 pagesVersion Structures and Functions of Living Organisms 8.L.1.1Marianna HernandezNo ratings yet
- Clinical Staging of Oral Submucous Fibrosis: A Review: Shivakumar.G.C., and Sahana.SDocument4 pagesClinical Staging of Oral Submucous Fibrosis: A Review: Shivakumar.G.C., and Sahana.Smorza rahbrNo ratings yet
- Metabolic and Complicated Cataract: DR - Ajai Agrawal Additional Professor Department of Ophthalmology AIIMS, RishikeshDocument31 pagesMetabolic and Complicated Cataract: DR - Ajai Agrawal Additional Professor Department of Ophthalmology AIIMS, Rishikeshsai shantanu100% (1)
- The Origin of Comfort TheoryDocument6 pagesThe Origin of Comfort Theoryibrahimaldarawi34No ratings yet
- ACCT6194039-Ethics and Corporate Governance - 2502150881Document12 pagesACCT6194039-Ethics and Corporate Governance - 2502150881Dini SaputriNo ratings yet
- 50K Training PlanDocument2 pages50K Training PlanStephen RoemerNo ratings yet
- Ensuring Patient Comfort and Clinical Accuracy During Impression Taking 3Document11 pagesEnsuring Patient Comfort and Clinical Accuracy During Impression Taking 3Raul HernandezNo ratings yet
- NCM 3260 - Gastro - Intestinal ObstructionDocument36 pagesNCM 3260 - Gastro - Intestinal ObstructionCherish Marie HurbodaNo ratings yet
- Assessment of Permit HolderDocument22 pagesAssessment of Permit HolderdhaspNo ratings yet
- Shigella PDFDocument2 pagesShigella PDFxpmathNo ratings yet
- SUPAC-IR Questions and Answers About SUPAC-IR Guidance - FDADocument13 pagesSUPAC-IR Questions and Answers About SUPAC-IR Guidance - FDAmodava-2No ratings yet
- ACCREDITED PROFESSIONAL ORGANIZATIONS (APOs) and ACCREDITED INTEGRATED PROFESSIONAL ORGANIZATIONS (AIPOs) As of March 4 2021Document7 pagesACCREDITED PROFESSIONAL ORGANIZATIONS (APOs) and ACCREDITED INTEGRATED PROFESSIONAL ORGANIZATIONS (AIPOs) As of March 4 2021ChinoNo ratings yet
- Palmoplantar Hyperhidrosis: A Therapeutic ChallengeDocument4 pagesPalmoplantar Hyperhidrosis: A Therapeutic ChallengeWesley DornelasNo ratings yet
- PROGNOSIS EbmDocument25 pagesPROGNOSIS EbmcarinasheliaNo ratings yet
- LA Union: PDRRM ODocument32 pagesLA Union: PDRRM OEnash RidNo ratings yet
- Stok Opname Awal Bulan Februari 2019Document11 pagesStok Opname Awal Bulan Februari 2019Yulianti YuliNo ratings yet
- Poster Chi2 - Ocular Albinism HKDocument1 pagePoster Chi2 - Ocular Albinism HKyollayusticiaNo ratings yet
- Accepted ManuscriptDocument29 pagesAccepted ManuscriptDaniel CarcamoNo ratings yet
- Jawbone CavitationsDocument8 pagesJawbone CavitationsCAESA96No ratings yet
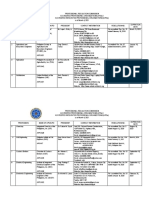
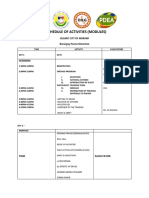
- CBRP Schedule of Activities (Modules) : Islamic City of Marawi Barangay Poona MarantaoDocument6 pagesCBRP Schedule of Activities (Modules) : Islamic City of Marawi Barangay Poona MarantaoJazzera Mustapha100% (1)
- Simorangkir (2021) - DONEDocument13 pagesSimorangkir (2021) - DONEMaya HammoudNo ratings yet
- Mrs DR Doris Voit Patient Safety in Germany - From The Hospital PerspectiveDocument74 pagesMrs DR Doris Voit Patient Safety in Germany - From The Hospital PerspectiveDissa Naratania HantraNo ratings yet
- Healing Purrs Article About Health Benefits of CatsDocument4 pagesHealing Purrs Article About Health Benefits of Catsbudalastina1No ratings yet