Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5834)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (350)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (824)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (405)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Intro To Plastic Injection Molding EbookDocument43 pagesIntro To Plastic Injection Molding EbookJames Farrugia78% (9)
- Stoichiometry Worksheet6-1Document6 pagesStoichiometry Worksheet6-1Von AmoresNo ratings yet
- Osgood-Schlatter DiseaseDocument6 pagesOsgood-Schlatter DiseaseDonny KurniawanNo ratings yet
- OsteoporosisDocument257 pagesOsteoporosisDonny KurniawanNo ratings yet
- Relationship Between Anaerobic Power, Vertical Jump and Aerobic Performance in Adolescent Track and Field AthletesDocument7 pagesRelationship Between Anaerobic Power, Vertical Jump and Aerobic Performance in Adolescent Track and Field AthletesDonny KurniawanNo ratings yet
- Task Force 8: Classification of SportsDocument4 pagesTask Force 8: Classification of SportsDonny KurniawanNo ratings yet
- Category Male Female Left Right Left RightDocument1 pageCategory Male Female Left Right Left RightDonny KurniawanNo ratings yet
- Injuries, Risk Factors and Prevention Initiatives in Youth SportDocument27 pagesInjuries, Risk Factors and Prevention Initiatives in Youth SportDonny KurniawanNo ratings yet
- Sport InjuryDocument61 pagesSport InjuryDonny KurniawanNo ratings yet
- Hand and Wrist ExamDocument80 pagesHand and Wrist ExamxpcoolzNo ratings yet
- CBRDocument3 pagesCBRJunita PasaribuNo ratings yet
- Homeroom Guidance: Apply Effective Ways of Protecting Oneself and OthersDocument11 pagesHomeroom Guidance: Apply Effective Ways of Protecting Oneself and OthersJazmin Nicole AbanesNo ratings yet
- Excavation TrainingDocument60 pagesExcavation TrainingFahad Abdul HaqNo ratings yet
- 1 s2.0 S096098221730708X MainDocument5 pages1 s2.0 S096098221730708X Mainrotinda bilekNo ratings yet
- Employee Training & DevelopmentDocument27 pagesEmployee Training & DevelopmentEnna Gupta100% (2)
- Model Course 1.07 PDFDocument75 pagesModel Course 1.07 PDFShiena CamineroNo ratings yet
- Process Flow ChartDocument22 pagesProcess Flow ChartKumar Ashutosh100% (1)
- Manas Arora 3 Year - B Roll No. 3 Vastu Kala AcademyDocument12 pagesManas Arora 3 Year - B Roll No. 3 Vastu Kala AcademyManasAroraNo ratings yet
- Minimum Wages in MaharashtraDocument6 pagesMinimum Wages in MaharashtrasalapeNo ratings yet
- AMRITA EXAM DatesheetDocument9 pagesAMRITA EXAM DatesheetSARRALLE EQUIPMENT INDIA PVT LTDNo ratings yet
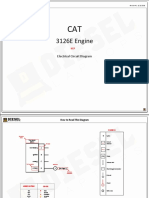
- 3126E Engine: Electrical Circuit DiagramDocument10 pages3126E Engine: Electrical Circuit DiagramPhil B.No ratings yet
- Lesson Plan in Science 1.3Document38 pagesLesson Plan in Science 1.3Heidi Dalyagan DulnagonNo ratings yet
- Extension 2 Proof GuideDocument6 pagesExtension 2 Proof GuideAlexander XieNo ratings yet
- Michigan Strategic Compliance Plan FINALDocument22 pagesMichigan Strategic Compliance Plan FINALbcap-oceanNo ratings yet
- Lab6 Phase Locked LoopsDocument20 pagesLab6 Phase Locked Loopsuitce2011No ratings yet
- Error Handling in ASPDocument116 pagesError Handling in ASPkagga1980No ratings yet
- DMA Actuator Drives For - Motorised Butterfly Valve DMK - Motorised Throttle DMLDocument8 pagesDMA Actuator Drives For - Motorised Butterfly Valve DMK - Motorised Throttle DMLemil_88No ratings yet
- Work Inspection Checklist: Project DetailsDocument1 pageWork Inspection Checklist: Project Detailsmark lester caluzaNo ratings yet
- Fallacies of Defective Induction 2Document29 pagesFallacies of Defective Induction 2Paul Romualdez Tan100% (1)
- Earth Dams Foundation & Earth Material InvestigationDocument111 pagesEarth Dams Foundation & Earth Material Investigationmustafurade1No ratings yet
- Spatial Modulation - Optimal Detection and Performance AnalysisDocument3 pagesSpatial Modulation - Optimal Detection and Performance AnalysisAliakbar AlastiNo ratings yet
- Nimble Number Logic Puzzle II QuizDocument1 pageNimble Number Logic Puzzle II QuizpikNo ratings yet
- Front Wheel Assy. DrumDocument2 pagesFront Wheel Assy. DrumSoroj BiswasNo ratings yet
- Refrigerator Freezer: Owner's ManualDocument22 pagesRefrigerator Freezer: Owner's ManualthaiNo ratings yet
- Benstones Instruments IMPAQ ELITE 4 CanalesDocument8 pagesBenstones Instruments IMPAQ ELITE 4 CanalesmauriciojjNo ratings yet
- Refrigerant Changeover Guidelines CFC-12 To R-401ADocument7 pagesRefrigerant Changeover Guidelines CFC-12 To R-401AMaria DazaNo ratings yet
- Astm d7091 13Document10 pagesAstm d7091 13Anonymous zia5og7psNo ratings yet
- Parts List: JTR-MOL254/LBADocument74 pagesParts List: JTR-MOL254/LBAJoseNo ratings yet