Professional Documents
Culture Documents
Angiogenic Factors
Angiogenic Factors
Uploaded by
hamzaCopyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Angiogenic Factors
Angiogenic Factors
Uploaded by
hamzaCopyright:
Available Formats
Critical Reviews in Oncology/Hematology 93 (2015) 225236
Angiogenic factors in chronic lymphocytic leukaemia (CLL):
Where do we stand?
Luis Mario Aguirre Palma a,1 , Iris Gehrke b,2 , Karl-Anton Kreuzer a,
b
a Department I of Internal Medicine, University of Cologne, Cologne, Germany
Manitoba Institute of Cell Biology, University of Manitoba, Winnipeg, MB, Canada
Accepted 1 October 2014
Contents
1.
2.
3.
Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Angiogenic factors and chronic lymphocytic leukaemia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2.1. VEGF . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2.2. bFGF . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2.3. PDGF . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2.4. Leptin . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2.5. G-CSF . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2.6. Follistatin . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2.7. Ang1 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2.8. ANG . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2.9. MK . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2.10. PTN . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2.11. PGRN . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2.12. PLF . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2.13. Angiogenic factors and macrophages . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2.13.1. PlGF . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2.13.2. Del-1 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Authorship and responsibility . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Conflict of interest statement . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Reviewers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Acknowledgements . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Biography . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
226
227
227
228
229
229
229
230
230
231
231
231
231
232
232
232
232
233
233
233
233
233
233
236
Abstract
The role of angiogenesis in haematological malignancies such as chronic lymphocytic leukaemia (CLL) is difficult to envision, because
leukaemia cells are not dependent on a network of blood vessels to support basic physiological requirements. Regardless, CLL cells secrete
Corresponding author: Department I of Internal Medicine, University of Cologne, Kerpener Strasse 62, 50937 Cologne, Germany. Tel.: +49 221 478 97626;
fax: +49 221 478 97627.
E-mail addresses: luis.aguirre-palma @uk-koeln.de (L.M. Aguirre Palma), Iris.Gehrke@cancercare.mb.ca (I. Gehrke), karl-anton.kreuzer@uni-koeln.de
(K.-A. Kreuzer).
1 Department I of Internal Medicine, University of Cologne, Kerpener Strasse 62, 50937 Cologne, Germany. Tel.: +49 221 478 97384;
fax: +49 221 478 97383.
2 Manitoba Institute of Cell Biology, University of Manitoba, Winnipeg, 675 McDermot, Canada MB R3E 0T3. Tel.+1 204 787 8776.
http://dx.doi.org/10.1016/j.critrevonc.2014.10.007
1040-8428/ 2014 Elsevier Ireland Ltd. All rights reserved.
226
L.M. Aguirre Palma et al. / Critical Reviews in Oncology/Hematology 93 (2015) 225236
high levels of major angiogenic factors, such as vascular endothelial growth factor (VEGF), basic fibroblast growth factor (bFGF), and
platelet derived growth factor (PDGF). Nonetheless, it remains unclear how most angiogenic factors regulate accumulation and delayed
apoptosis of CLL cells. Angiogenic factors such as leptin, granulocyte colony-stimulating factor (G-CSF), follistatin, angiopoietin-1
(Ang1), angiogenin (ANG), midkine (MK), pleiotrophin (PTN), progranulin (PGRN), proliferin (PLF), placental growth factor (PIGF),
and endothelial locus-1 (Del-1), represent novel therapeutic targets of future CLL research but have remained widely overlooked. This review
aims to outline our current understanding of angiogenic growth factors and their relationship with CLL, a still uncured haematopoietic
malignancy.
2014 Elsevier Ireland Ltd. All rights reserved.
Keywords: Angiogenesis; Angiogenic factors; Microenvironment; Chronic lymphocytic leukaemia (CLL); Pathological angiogenesis
1. Introduction
Angiogenesis, the development of new blood vessels,
is highly active during embryogenesis and development,
but in adult life only occurs during wound healing, menstrual cycles [1], and in heart and skeletal muscles from
strenuous exercise [2]. The complexity of angiogenesis is
illustrated by the interplay between a plethora of molecular and cellular elements, all of which regulate the
microenvironmental stability. In the bone marrow (BM)
microenvironment, T-cells, B-cells, osteocytes, stromal cells,
adipocytes, white blood cells, fibroblasts, and endothelial
cells (EC) live in an angiogenically-balanced microenvironment (Fig. 1a). This angiogenic balance is dependent on
the efficient molecular communication mediated by angiogenic factors (i.e. pro-angiogenic or angiogenic growth
factors), angiogenic inhibitors (i.e. anti-angiogenic factors),
cytokines, chemokines and accessory proteins, all of which
act in combinatorial manner to achieve optimal cellular
behaviour and tissue stability. Nevertheless, the aberrant
expression of the above-mentioned groups of molecules disturbs the angiogenic balance of organisms, turning on
the so-called angiogenic switch inducing pathological
angiogenesis.
Besides a molecular imbalance of factors, a persistent
and aberrant proliferation of EC is the outmost characteristic attributed to pathological angiogenesis. In addition to
sustaining uncontrolled growth and proliferation of solid neoplasms, pathological angiogenesis also supports leukaemia
[1]. Similarly to cells comprising solid neoplasms, malignant haematopoietic cells excessively secrete angiogenic
factors, among many other molecules, to the extra cellular
space, or better known as the microenvironment, to support
growth and proliferation [3]. In the case of CLL, angiogenesis is a permanent and dynamic subject of study in its
infancy.
CLL is a prevalent and incurable haematological malignancy among the adult population in Western societies [4]. It
is characterized by the clonal expansion of malignant CD5+
B-lymphocytes and because these fail to undergo timely apoptosis, they excessively accumulate in peripheral blood (PB),
BM (Fig. 1b), and LN. The overexpression and exorbitant
secretion of angiogenic factors disrupts the angiogenically
balanced microenvironments and supports malignant
B-cell accumulation, proliferation, and resistance to
apoptosis.
The initial correlation between pathological angiogenesis and CLL was described by Kini et al., who detected a
significant increase of microvessel density in BM biopsies
of CLL patients when compared to control BM sections
[5]. Concomitantly with a significant density increase of
microvessels, they reported increased levels of basic fibroblast growth factor (bFGF) in urine samples of CLL
patients, fostering the idea that angiogenesis is an active
processes in CLL [6]. Today it is widely accepted that
angiogenesis contributes to the development and progression of CLL [7], yet the molecular mechanisms of most
angiogenic growth factors on the CLL context factors are
unclear.
The three most widely studied angiogenic factor in the
CLL context are vascular endothelial growth factor (VEGF),
bFGF, and platelet derived growth factor (PDGF). In this
review, we intend to shed some light on vague factors such
as leptin, granulocyte colony-stimulating factor (G-CSF),
follistatin, angiopoietin-1 (Ang1), angiogenin (ANG), and
midkine (MK). Due to their strong angiogenic properties and
their unclear role in CLL pathophysiology, we explore the
roles of developmental endothelial locus-1 (Del-1), placental growth factor (PIGF), pleiotrophin (PTN), progranulin
(PGRN), and proliferin (PLF). Whilst angiogenesis is a complex and fast growing field, this review exclusively focuses on
describing where we stand in the study of angiogenic growth
factors in the CLL context. Table 1 summarizes some of the
relevant attributed roles to each factor and indicates some of
the downstream targets.
We conclude that angiogenic factors will become the
essential targets of anti-CLL therapy, because besides
conferring CLL with survival advantage, they modulate
cellular behaviour and alter the cellular composition of the
cancer microenvironment. In addition, angiogenic factors are
receiving significant attention by the scientific community,
because they are the optimal target in trying to achieve
tumour remission. In conjunction with classical therapies,
the development of potential novel and efficient anti-CLL
therapy will target one or more of the angiogenic factors
and understanding the angiogenic molecular mechanics
L.M. Aguirre Palma et al. / Critical Reviews in Oncology/Hematology 93 (2015) 225236
227
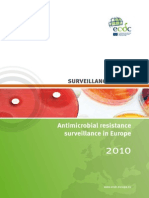
Fig. 1. Comparison of the BM and PB microenvironment between a healthy and CLL state. In the BM of healthy individuals (a), there is a balance
between angiogenic growth factors and inhibitors. B-lymphocytes numbers remain low and the ECL remains quiescent. The bone marrow environment is a rich
cellular entity hosting adipocytes, fibroblasts, stromal cells, osteocytes, endothelial cells, basophils, and white blood cells including B- and T- lymphocytes. In
CLL patients (b), malignant B-cells accumulate disproportionately in BM and PB and the excessive secretion of angiogenic factors could in return compromise
the ECL, allowing the infiltration of CLL lymphocytes. Platelets were omitted from this model. ECL, endothelial cell layer; PB, peripheral blood; BM, bone
marrow.
solely governing CLL is paramount to achieving this
task.
2. Angiogenic factors and chronic lymphocytic
leukaemia
2.1. VEGF
The VEGF family of ligands, receptors, and co-receptors
is the most widely studied molecular family in the field of
angiogenesis, because their molecular behaviour tightly links
these factors to several solid and haematopoietic malignancies [8]. For instance, the overexpression of VEGF ligands
is closely linked to tumour development, progression, and
metastasis [911]. Due to its central role in angiogenesis,
VEGF became the target of the first antiangiogenic drug ever
approved by the U.S. Food and Drug Administration (FDA)
for the treatment of colorectal cancer [12]. In fact, recent
research exploring the mechanism of action of bevacizumab
on CLL cells showed the efficiency of this monoclonal antibody in inducing apoptosis of leukaemia cells [13]. Whilst
many studies highlight the importance of VEGF as target
of research in CLL angiogenesis [7,11,1317], we are still
refining our understanding of the VEGF family in the CLL
context.
After detecting the expression of VEGF in CLL cells
[18], researchers observed a correlation between serum levels
of VEGF, risk of disease progression, and progression free
survival (PFS) [19]. The sensitivity of CLL cells to VEGF
ligands is illustrated by their expression of the three VEGF
receptors [14]. Two co-receptors of VEGFR-1 and VEGFR-2,
neuropilin-1 and -2 (NRP1/2) [20], regulate angiogenesis, tumour development, and immunological responses [7].
Recently Piechnik et al. reported higher NRP1 expression
on leukemic lymphocytes when compared to healthy Blymphocytes in a cohort that included 114 CLL patients
[7]. Furthermore, they detected an increase in NRP1 expression upon VEGF stimulation. In addition, regulatory T cells
(Tregs) and plasmacytoid dendritic cells (PDCs), essential
228
L.M. Aguirre Palma et al. / Critical Reviews in Oncology/Hematology 93 (2015) 225236
Table 1
Roles associated with angiogenic factors and the pathways/factors they regulate.
VEGF
bFGF
PDGF
Leptin
G-CSF
Follistatin
Ang1
ANG
MK
PTN
PGRN
PLF
PIGF
Del-1
Associated roles
Downstream targets
Survival, proliferation, migration, mobilization, permeability [20]
Proliferation, survival, growth arrest, migration, differentiation, tissue repair,
angiogenesis, inflammation [105]
Wound healing, tumor development [32], proliferation, migration, tube formation
[37]
Survival, proliferation [106], immunological responses [41], lymphopoiesis [43]
Granulopoiesis regulation, survival, proliferation, activation and maturation of
neutrophylic cells [46], phagocytosis enhancement [48], HPSCs mobilization [49]
Proliferation, differentiation, apoptosis [108], activin regulation [52]
Vasculogenesis [109], survival, sprouting and reorganization of blood vessels [62],
proliferation [110]
Tumor establishment and growth [69],
Proliferation, migration, anti-apoptosis, mitogenesis, transformation, tumor
angiogenesis [113]
Neovascularization, tumorogenesis [79], proliferation, migration [115]
PCy1, MAPK- FAK [20], PI3K-AKT [10]
MAPK/ERK, PI3K-AKT, STAT, PLC [21]
Cell cycle progression, motility [117], tissue repair, tumorogenesis, inflammation
[85]
Migration, proliferation [88], invasion, tube formation [91]
Tumorogenesis, vascular remodeling in a VEGF-dependent manner [120],
lymphangiogenesis, tumor cell motility [98]
Adherence and migration of endothelial cells [99], phosphatidylserine recognition
[92]
PI3K-AKT, PLC1, ERK, Akt [34]
JAK-STAT [107], NF-B [41]
JAK-STAT, RAS-MAPK [46]
Smad proteins [56]
Dok-R [111], ABIN-2 [112]
ERK1/2, PKB-AKT, SAPK-JNK [70]
ERK1/2, p38 [114]
c-SRC, FAK, PI3K and MAPK [79], [116], -catenin
phosphorylation [81]
PI3K [117], inhibits anoikis and apoptosis [118]
FGF/STAT5/PLF signaling cascade [91] JAK-STAT,
MAPK [119]
MAPK [121]
RAS-MAPK [122]
Abbreviations: ABIN-2, A20-binding inhibitor of NFB-2; ANG, angiogenin; Ang1, angiopoietin 1; Ang2, angiopoietin 2; bFGF, basic fibroblast growth factor;
c SRC, proto-oncogene tyrosine-protein kinase Src; Del-1, developmental endothelial locus-1; Dok-R, dock protein-R; ERK1/2, extracellular signal-regulated
kinase 1/2; FAK, focal adhesion kinase; FLRG, follistatin related gene; G-CSF, growth colony-stimulating factor; HPSC, hematopoietic stem/progenitor cells;
JAK, Jak2 tyrosine kinase; JAK-STAT, Janus kinase- signal transducer and activator of transcription; MAPK, mitogen activated protein kinase; MAPK/ERK,
mitogen-activated protein kinases/extracellular signal-regulated kinase; MK, midkine; NF-B, nuclear factor kappa-light-chain-enhancer of activated B cells;
p38, a mitogen-activated protein kinase pathway; PC1, phospholipase C gamma-protein; PDGF, platelet-derived growth factor; PDGF-B, platelet-derived
growth factor-B; PGRN, progranulin; PI3K-AKT, Phosphatidylinositide 3-kinase-AKT; PIGF, placental derived growth factor; PKB-AKT, protein kinase B/AKT
pathway; PLF, Proliferin; FGF, fibroblast growth factor; PTN, pleiotrophin; RAS-MAPK, RAS-mitogen-activated protein kinase; STAT, signal transducers and
activators of transcription; VEGF, Vascular endothelial factor growth factor; SAPK-JNK, stress-activated protein kinase/Jun-amino-terminal kinase.
mediators of tumour survival and immunological responses,
commonly express NRP1. Interestingly, Treg and PDCs isolated from CLL patients also express higher levels of NRP1
when compared to controls [7]. It is possible to infer that
changes on NRP1 expression provide CLL with a mechanism of immunological protection and apoptosis evasion [7].
Targeting both NRPI and VEGF rather than only targeting
VEGF increases the benefits of anti-angiogenesis therapy in
malignancies [7]. It is not only the overexpression of ligands and receptors that contributes to CLL severity. Recent
research reveals that VEGF gene polymorphisms diversity
modulates pathophysiology of CLL cells and that this diversity has an impact on overall survival in indolent CLL cases
[16]. Since we are still unable to target VEGF in CLL patients,
the recent evidence emphasised the impact of VEGF in the
CLL microenvironment by controlling the expression of relevant VEGF receptors not only on CLL, but also on accessory
Tregs and PDCs.
2.2. bFGF
The commonly described members of FGF ligand family are acidic FGF (aFGF or FGF1) and basic FGF (bFGF or
FGF2), essential ligands for tumour growth and angiogenesis.
However, studying the FGF family represent a challenge
to CLL researchers, mainly because the family comprises
22 members of diverse biological functions, which act
as intracellular or extracellular signalling molecules in an
intracrine, paracrine or endocrine fashion [21]. Furthermore,
the interaction of FGFs with other members of the stem
cell signalling network, namely BMP/TGF (bone morphogenetic protein/transforming growth factor ), Wnt, and
Notch signalling regulates not only pluripotent stem cells, but
also cancer stem cells [22].
Upregulation of bFGF is detected in acute myeloid
leukaemia (AML), chronic myelomonocytic leukaemia
(CML), and CLL, out of which CLL presents the highest
level [23]. Similarly to VEGF levels, increased bFGF levels in
CLL patients correlate with poorer prognosis [24,25]. When
researchers treated cell lines that resemble chronic lymphoid
malignancies with fludarabine alone, or in combination with
bFGF, they showed that bFGF not only confers survival
advantage, but also induces bFGF mRNA levels synthesis,
inferring that bFGF delays fludarabine-dependent apoptosis [26]. Similarly, intensive fludarabine-containing regimens
induce a decrease of bFGF and VEGF [27]. Lenalidomide
is an immunomodulating drug (IMiD) which has shown
clinical activity against relapsed or refractory CLL cases
L.M. Aguirre Palma et al. / Critical Reviews in Oncology/Hematology 93 (2015) 225236
[28]. Administration of lenalidomide decreases the detectable
plasma level of bFGF and VEGF in stable and progressive
CLL cases [29]. Furthermore, in CLL co-cultures with ECs,
lenalidomide eliminated the survival advantage conferred by
EC layer (ECL) and reduced the amount of free ECs present
in circulation [29]. Besides emphasising the role of bFGF
in CLL survival, the above indicates lenalidomide successfully disrupt molecular communication between CLL cells
and accessory cells in the microenvironment.
2.3. PDGF
Overexpression of classical PDGFs, PDGF- and
PDGF-, is closely linked to several neoplasms and
atherosclerosis [30]. Furthermore, PDGFs stimulate proliferation of quiescent cells [31] and act as mitogens and
chemoattractants for mesenchymal cells (MSC), important
components of the cancer microenvironment [32]. PDGFR-
plays a role during embryogenesis whilst PDGFR- is widely
expressed by MSC [32]. Also, PDGFs keep vasculature in a
quiescent state by regulating pericytes and ECs [33]. PDGF-
binds and activates the corresponding receptors, PDGFR and PDGFR- [34]. Detection of PDGF-A at all stages
of B-lymphocytes shows the putative role of this factor in
controlling differentiation and proliferation of pre-leukemic
B-cell lines [35].
There is a strong correlation between elevated plasma
levels of both PDGF and VEGF and advanced CLL stages
[36]. CLL patients, however, display higher expression of
PDGF- than PDGF- and some patients show the concomitant expression of PDGF- and PDGF-R [35]; PDGFR
is not present in CLL [36]. PDGF-PDGFR signal transduction triggers MSC to secrete VEGF [36]. Fibroblasts closely
interact with the microenvironment and cancer cells and are
releasers of excess cytokines and growth factors, such as
PDGF [37]. Due to the fact that PDGF induces MSC to
secrete VEGF, this could trigger CLL cells to shift from a quiescent to a pathologically progressive status [36]. Targeting
PDGF/PDGFR signalling has been achieved with immatinib,
a tyrosine kinase inhibitor specific for PDGFRs, c-KIT and
BCR-ABL. The agent showed a promising anti-angiogenic
effect when tried on cancer lines, inhibiting cell proliferation,
invasion, and migration [38]. It is also plausible to infer that
PDGF and bFGF synergize to enhance signal transduction
events that rescue CLL cells from apoptosis [35]. Experimental strategies exploring the interaction between CLL cells
and accessory MSC will reveal the importance of PDGF in
regulating direct cell-to-cell interaction, as well as survival
advantage offered by PDGF to leukaemia cells.
2.4. Leptin
Leptin, obese (ob) gene [39], is a mitogen, an angiogenic
factor [40], and a regulator of essential immunological
responses [41]. One of the utmost characteristics of this
angiogenic factor is its putative ability to regulate the efficient
229
energy expenditure during angiogenesis [42]. Upon binding
to its receptors, Ob-receptors (Ob-Rs), leptin activates the
haematopoietic pathways that trigger lymphopoiesis [43].
Leptin/Ob-Rs interaction promotes B-cell homeostasis,
initiating expression of Bcl-2 and cyclin-D [41]. Furthermore, leptin signalling apparently provides B-cells with
cytoprotection, thus promoting survival, proliferation, and
possibly evasion to apoptosis through the activation of
B-cell CLL/lymphoma 2 (Bcl-2) and cyclin D1 [41]. In
addition, leptin is likely to support proliferation of the T-cell
population [44].
There have been conflicting studies about the leptin levels
found in CLL and their correlation with the severity of the
disease. Earlier, Pamuk et al. described an increase in leptin
levels in CLL cases which correlated with the poor prognosis
marker CD38 [44]. However, in a more recent study, Dalamaga et al. showed that leptin levels were lower in CLL patients
than in controls, a pattern also detected in acute myeloid
leukaemia (AML) and acute lymphoblastic leukaemia (ALL)
patients [45]. Notably, Dalamaga et al. matched control
patients admitted to the hospital for non-neoplastic/-infection
diagnosis with CLL patients based on age (5 years), gender, and year/month of diagnosis (1 month). Whilst Pamuk
et al. included serum from 13 CLL patients and employed
ELISA for the detection of leptin, Dalamaga et al. included
95 CLL patients and employed a sensitive radioimmunoassay
to measure serum leptin concentration. Future research will
refine the guidelines for measurement of angiogenic factors
concentration, but whether it is the up- or downregulation of
leptin, both scenarios indicated that leptin levels do correlate
with the CLL status. Furthermore, the capacity of leptin to
support proliferation of T-cell indicates that changes in leptin
concentration could alter the cellular composition in the BM
microenvironment.
2.5. G-CSF
G-CSF supports survival of normal haematopoietic progenitor cells, myeloid leukaemia cells, and leukemic cell
lines [46]. Together with stem cell factor (SCF), interleukin3 (IL-3), granulocyte-macrophage colony-stimulating factor
(GMCSF), and IL-6, G-CSF induces myeloid progenitors
to proliferate, differentiate, and mature [46]. Additionally,
G-CSF is the only angiogenic factor capable of regulating terminal maturation of neutrophilic granulocytes [46].
Above all, G-CSF is vital for host defence and expression
can increase up to 10-fold during infection [47].
G-CSF induces premature release of neutrophils from
the marrow [48] and is commonly employed to mobilize
haematopoietic progenitor stem cells (HPSCs) in allogeneic
transplant recipients [49]. In combination with CXC
chemokine receptor type-4 (CXCR-4), G-CSF -induced
mobilization of HPSCs is a strategy of potential use in CLL
and AML patients to improve the results of chemotherapy
treatment [50]. As a matter of fact, the administration of
G-CSF in combination with fludarabine, cyclophosphamide,
230
L.M. Aguirre Palma et al. / Critical Reviews in Oncology/Hematology 93 (2015) 225236
and rituximab (FCR) improved clinical status of CLL patients
by enhancing progression-free survival and overall survival
[51].
2.6. Follistatin
The main role of follistatin is to regulate activin A [52], a
potential regulator of growth and differentiation of a variety of
cell types, including haematopoietic progenitors [53]. Activin
A is secreted by macrophages, stimulates antibody production, and modulates development Treg cells. Additionally,
activin A appears to regulate inflammatory and immunological responses, as well as fibrosis [54]. Follistatin binds to
activin A with high affinity preventing binding of activin A
to the constitutively activated type II receptor kinase, thus
inhibiting downstream signalling [55]. Furthermore, it has
been shown that the presence of activin A induces follistatin expression possibly as a negative feedback mechanism
against excessive activin A activity [56].
In 1998, the follistatin related-factor-gene (FLRG) homologous to follistatin was cloned from a case of CLL bearing
t(11;19) translocation [57]. However, FLRG is not detected in
haematopoietic cells from lymphoid B and T lineage [53,57].
Similarly to follistatin, CLL-derived FLRG binds to activin
A to regulate haematopoietic processes [53]. Interestingly,
activin A is functional in vivo within the haematopoietic
microenvironment, as a regulator of B-cell growth [58]. High
levels of activin A appear to negatively impact the generation of B-lymphocytes as shown in BM culture by inhibiting
B-cell spread and accumulation whereas follistatin enhances
pre-B-cell production [58].
Whilst FLRG acts as haematopoietic cytokine to trigger immature progenitor differentiation, follistatin acts over
the more mature population [59]. The role of follistatin and
FLRG in determining B-cell generation makes it an attractive
target on the CLL angiogenesis, because activin A inhibits
B-cell generation and this in turn is a factor secreted by
macrophages, which are important cellular components of
the CLL microenvironment. It is likely that disruption in
the follistatin/FLGR and activin molecular interaction could
influence the generation and accumulation of CLL cells, as
well as their interaction with macrophages. Whether CLL cell
express the receptor to either follistatin/FLRG remains to be
elucidated.
2.7. Ang1
The main players of the Ang-Tie signalling pathway are
the ligands angiopoietin-1 and angiopoietin-2 (Ang1 and
Ang2), and the receptors tyrosine kinase with immunoglobulin and endothelial growth factor domain-1 (Tie1) and
Tie2. Ang1 acts by binding Tie2 functioning as a regulator of vasculogenesis and angiogenesis. Additionally,
Ang1 has an attributed anti-inflammatory role that promotes
pericyte-dependent vessel integrity and supports a Tie2constitutively activated state, thus modulating the quiescent
vascular endothelium [60]. Whilst Ang1 and Ang2 are
homologous, they differ widely in their biological roles
[61]. Ang2, the Ang1 antagonist, is an angiogenic inhibitor
involved in destabilization and vascular remodelling [60] and
is strongly released during vasculogenesis and inflammation
[62]. Tie1 and Tie2 are tyrosine receptor kinases receptors
vital for proliferation, migration, and survival of EC [63].
There is an notable increase in the expression of Ang2
ligand that appears to negatively impact disease course in
CLL patients [64]. Concomitant with the elevated increase
in Ang2 levels in CLL cases is an aberrant vascularization
observed in BM sections [65]. Besides secreting high Ang2
levels, there is an associated upregulation of VEGF [65].
Moreover, elevated levels of Ang2 can be linked to Binet
staging [66]. Recent epigenetic evidence showed that Ang2
displays lower DNA methylation in CLL, which correlates
with poor prognosis, shorter time to first treatment (TTFT),
and shorter survival [64]. All of this points toward an active
role of Ang2 in regulating the pathophysiology of CLL cells
through the Ang-Tie signalling pathways.
Thanks to a series of elegant biochemical experiments,
nowadays we are able to better understand the molecular
mechanics behind the Ang-Tie signalling system. Evidence
clearly demonstrates that Tie1, formally known as an orphan
receptor, acts as an active inhibitor of Tie2, thus strongly
regulating the Ang-Tie signalling system and downstream
molecular events. Tie1 and Tie2 bind and form an inhibitory
complex. Interestingly this complex only requires that Tie1
and Tie2 interact through their ectodomains and neither
Ang1, Ang2, nor another auxiliary factor is involved in the
formation this complex [63]. Nevertheless, Ang1 and Ang2
ligands regulate the molecular behaviour of the Tie1Tie2
receptor complex in very different manners. Ang1 is capable
of destabilizing the complex and inducing Tie2 signal transduction. However, Ang2, the antagonist ligands, is incapable
of disrupting the Tie1Tie2 complex and therefore fails to
induce Tie2-dependent signal transduction [61]. In addition,
Ang2 binds to Tie2 and prevents binding of Ang1 [63]. Cells
that express only Tie2 but not Tie2 are susceptible to Ang2
activity and in this scenario Ang2 is capable of triggering
Tie2-dependent signal transduction [63]. In support of the
different performance of Ang1 and Ang2, there is recent
evidence clearly identifying the specific amino acid residues
on Ang1 and Ang2, which determine their roles as either
agonist or antagonist [61].
Interestingly, CLL cells fail to express receptor Tie2, but
express Tie1, Ang1 [67], and highly express Ang2 [65],
[66]. If only the ectodomain interaction between Tie1 and
Tie2 is important to establish the a Tie1Tie2 complex,
expression of Tie1 on CLL cells strongly indicates a putative interaction with Tie2-expressing cells in order to prevent
Ang2 from activating Tie2-only expressing cells present in
the CLL microenvironment. This suggests a cell-to-cell regulatory mechanism of Ang-Tie signalling pathway, which
would require direct cell contact between CLL cells and
Tie2-expressing cells.
L.M. Aguirre Palma et al. / Critical Reviews in Oncology/Hematology 93 (2015) 225236
2.8. ANG
Angiogenin (ANG) is a powerful angiogenic factor
produced by neoplastic cells and cells from the cancer microenvironment [68]. The increased levels of ANG
in malignancies is associated with tumour initiation and
development [69]. Acute myeloid leukaemia (AML) and
myelodysplastic syndrome (MS), and a variety of other
malignancies display ANG upregulation [70]. This upregulation also correlates to poor prognosis in patients of myeloid
leukaemia and myelodysplastic syndromes [68].
Evidence linking CLL and ANG comes from a study
including 77 CLL cases of untreated patients on Binet stage
A [71]. In spite of reporting only a minor difference of ANG
levels, the 5-year progression-free survival was 85% for
patients with ANG above the median (300 ng/ml), against
51.5% for those with values lower than the median when taking into consideration the cut-off ANG concentration [71].
Additionally, the levels of ANG could be integrated into Rai
substages [71]. Previously, Pavlov et al. suggested ANG as
a possible prognostic marker and potential target of antiangiogenic therapy [72]. Notably, ANG is capable of directly
binding follistatin without the help of interacting pattern,
not even activin a, suggesting a follistatin/ANG synergy
[73]. Concomitantly with bFGF and VEGF downregulation
is overexpression of ANG and Ang2 in CLL upon lenalidomide administration [29]. Possibly ANG actively interacts
with Ang2, bFGF, VEGF, and follistatin to regulate survival
and quiescent in the cancer microenvironment.
2.9. MK
Upregulation of MK correlates with poor prognosis in
neuroblastomas, astrocytomas, pancreatic head carcinomas,
gastrointestinal stromal tumours, and blood malignancies
[7476]. This factor has been remarkably associated with
unregulated cell growth [75]. CLL patients present an
elevated level of MK secretion as detected by serum measurements [74]. A similar expression pattern of MK expression
is observed in other haematopoietic malignancies [77]. The
singularity of MK resides in its ability to activate a mechanism that regulates survival and homeostasis of peripheral
mature B-cells and CLL cells [74].
MK triggers angiogenesis by binding to receptor protein
tyrosine phosphatase zeta (RPTP), inducing Bcl-2 expression and inhibiting caspase-3/-7 [76] without compromising
caspase-8 activity [78]. Interaction of MK and the receptor RPTP modulate signal transduction events that lead to
survival advantage [74]. Blocking the interaction between
MK and RPTP results in CLLs apoptosis and inhibition of
MIF/CD74 signal transduction [74]. Due to its proapoptotic
effect on CLL cells, MK appears as a potential therapeutic
development, however, even when efficient, blocking of the
RPTP is not complete [74]. MK is a novel angiogenic factor and further studies will provide an integral understanding
231
of how the MK/RPTP signalling system influences CLL
pathogenesis.
2.10. PTN
PTN is a novel angiogenic factor that appears to induce ex
vivo angiogenesis, neovascularization in developing nervous
system and tumourigenesis [79]. The receptors implicated
in PTN signal transduction are N-syndecan, anaplastic lymphoma kinase (ALK) associated with PTN-related tumour
growth receptor, RPTR beta/zeta (RPTP/), and 3 integrins [80]. By interacting with 3 integrins, PTN induces
EC migration [80]. Even when the evidence derives from
aortic rings models, it is clear that PTN possesses the
proangiogenic capacity to generate capillary networks [79].
Together with VEGF upregulation, high levels of PTN correlated with bad prognosis in colorectal cancer patients,
suggesting the use of PTN as a prognosis factor [81]. Even
though no evident link existed between PTN, evidence shows
that PTN binds to the receptor RPTP/ and modulates catenin phosphorylation, thus regulating VEGF production
[81].
CLL cells seem to produce higher level of PTN, and what
is more, the level of mRNA correlates to the severity of CLL
cases [82]. Whereas negative controls express the PTN transcript at a basal level, this factor is overexpressed in CLL
samples [82]. Similar to other angiogenic factors, PTN serum
levels are higher in CLL patients when compared than in controls. What is more, blocking PTN by antibody administration
in culture triggers apoptosis of CLL cells, suggesting that
PTN is directly involved in promoting the survival of CLL
cells [82]. Possibly PTN also modulates -catenin activity
in CLL cells and acts as an alternative mechanism to control
VEGF secretion of CLL cells.
2.11. PGRN
A variety of neoplasm and cervical cancer models established that relevance of PGRN in tumour cell proliferation
and tumour growth [83]. PGRN supports chemoresistance
and has a clear role in cancer cell migration, invasion, and
angiogenesis [84]. Researchers have elucidated that PGRN
directly binds tumour necrosis factor receptors (TNFRs), disrupting TNF-TNFR binding suggesting that PGRN works
as a natural antagonist of TNF and as a regulator of inflammation [85]. Stimulation of CLL with CD40 is a strategy to
recreate the LN microenvironment. A relevant feature of the
LN microenvironment is that it allows CLL cells to have an
increased NF-B activity in comparison to those derived from
peripheral blood, thus supporting a chemoresistance effect
[86]. Furthermore, mimicking the LN microenvironment
results in overexpression of TNFR-1/-2, NF-B activation,
and TNF production by CLL cells [86]. PGRN may restrict
the activation of inflammation-related signalling pathways by
interacting with CLL cells in the LN microenvironment.
232
L.M. Aguirre Palma et al. / Critical Reviews in Oncology/Hematology 93 (2015) 225236
Surprisingly, recent research by Gbel et al. demonstrated
the evident overexpression of PGRN in aggressive CLL
cases. In addition to detecting overexpression of PGRN, they
observed a correlation with bad prognosis markers, such as
unmutated IGHV status, CD38 and ZAP-70 positive status,
cytogenetics, and high Binet stage [87]. The high plasma level
of PGRN suggests the utility of this angiogenic factor as a
prognostic marker of CLL cells [84]. The inhibitory role of
PGRN on TNF-TNFR signalling and the abundant expression of PGRN detected in CLL patients indicate the dynamic
role of this angiogenic factor and denote its potential as a
novel therapeutic target.
2.12. PLF
PLF has a vital function in embryogenesis and tumour
growth support [88]. Whilst inactive in adults, reactivation
of PLF is observed in later-stage cell lines as seen in progressive fibrosarcoma [88]. PLF binds to the insulin-like
growth factor 2/mannose 6-phosphate receptor ((Man6P)/IGF-II), but the signal transduction mechanisms are
not well defined [89]. Besides interacting with PLF, this
receptor interacts and facilitates uptake of metalloproteases(M6P), cytokines, transforming growth factor- (TGF ),
leukaemia inhibitory factor, and endothelial growth factor
(EGF) [89,90].
In sarcoma models, secretion levels of PLF correlate with
disease progression [88]. bFGF is capable of inducing EC to
secrete PLF into the microenvironment by activating STAT5
[91]. It is possible to infer that bFGF and PLF synergistically
maximize the angiogenic response, since both factor, independently, support endothelial cell migration [88]. Excessive
bFGF levels secreted by CLL suggest the role of this factor in inducing PLF secretion to the CLL microenvironment.
If present in the CLL microenvironment, PLF levels will
correlate with the severity of the CLL case, however, to
our knowledge, no study has attempted to investigate PLF
in CLL.
2.13. Angiogenic factors and macrophages
Macrophages are essential cellular components of the
immune system and the cancer microenvironment, because
these cells are in charge of engulfing and eliminating
apoptotic cells before they release cytotoxic component
[92]. What is more, macrophages are essential secretors of
vital cytokines, such as TNF- and IL-6 [93], as well as
chemokines and angiogenic factors. Therefore, their recruitment is of utmost relevance in inflammation and angiogenesis
related processes. The macrophage migration inhibitory
factor (MIF) is a chemokine that appears to regulate inflammation and immune responses; CLL patients shows an
upregulation of this factor [94]. By employing murine models
to study the interaction between CLL cells and macrophages,
Reinhart et al. demonstrated that MIF is likely to regulate the
initiation of the leukemic stage as well as survival advantage
of leukaemia cells [94].
Furthermore, CLL patients display an increased monocytes counts together with infrequent cell populations such
as CD14 + CD16+ and macrophages expressing the receptor
Tie2 [95]. Since these findings suggest a strong relationship
of macrophages with CLL cells, it is plausible to think that
PIGF and Del-1, two powerful angiogenic growth factors,
could regulate CLL-macrophage relationships in the CLL
microenvironment.
2.13.1. PlGF
PlGF is secreted as a glycosylated homodimer that
stimulates angiogenesis by binding to VEGFR1 [2].
Outstandingly, PlGF recruits and activates macrophages indirectly through VEGFR1 signalling [93]. Blocking PIGF
inhibits macrophage recruitment, preventing initiation of
the angiogenic rescue program [96]. In addition, PIGF
expression is associated with inflammation processes that
accompany pathological angiogenesis [2]. As well, PIGF
strongly supports tumour burden and EC proliferation [97].
Remarkably, carcinoma-associated fibroblasts are strong
secretors of PIGF [97]. Utilization of monoclonal antibodies against PIGF showed an evident effect against tumour
development in human tumour xenographs [98]. Interestingly, employing PIGF siRNA induces a reduction of NRP1
expression, yet no changes in VEGF and VEGFR-1 are
detected [97]. Possibly PIGF and NRP1 synergize to confer stronger prosurvival signal and probably to regulate ECs
in the CLL microenvironment. Even if CLL themselves
do not express PIGF, NRP1 could be regulated by externally secreted PIGF in a paracrine fashion. Besides, PIGF
present in the CLL microenvironment is likely to regulate the
macrophage population and therefore the CLL-macrophage
interaction.
2.13.2. Del-1
Del-1 is essential during embryogenesis and the gene is
silenced in adult life [99]. Tumours expressing Del-1 show
an increased capillary density and accelerated growth rate
in vivo [100]. Del-1 is capable of increasing the number
of blood vessels and inducing proliferation of ECs [101].
Interestingly, Del-1 is secreted by activated macrophages
and recognizes phosphatidylserine, a phospholipid detected
on the outer cellular membrane of apoptotic cells [92].
Expression of Del-1 is detected in macrophages populating
the BM, indicating a tight control of the microenvironment [92]. The increased microvessel density observed in
BM sections [5,102] could possibly be linked to abnormal expression of Del-1 in the CLL microenvironment.
Nevertheless, the expression patterns of Del-1 in CLL
microenvironments and the effect on CLL cell apoptosis must
be elucidated.
L.M. Aguirre Palma et al. / Critical Reviews in Oncology/Hematology 93 (2015) 225236
233
proliferation, aberrant apoptosis, and excessive accumulation
of CLL cells.
Authorship and responsibility
LAP performed literature research and wrote the
manuscript, IG & KAK conceived the idea and wrote the
manuscript.
Fig. 2. Representation of the putative transient co-option of CLL cells
associated with TEM. Excessive secretion of angiogenic factors is tightly
linked to ECL destabilization and permeability. Refer to Fig. 1 for cell identification. Platelets were omitted from this model. ECLendothelial cell
layer; PBperipheral blood; BMbone marrow.
Conict of interest statement
All authors declare no conflict of interest. All have read
and approved the manuscript. This manuscript is not under
consideration elsewhere.
3. Conclusion
The prominent functions of angiogenic factors reside in
their ability to regulate cell proliferation, migration, survival,
tumour genesis, and tissue repair (Table 1).
It is plausible to believe that high levels of angiogenic factors secreted by CLL cells and surrounding accessory cells
compromise the stability of the ECL. This would facilitate
CLL cell infiltration and trafficking to and from the microenvironmental niche. Notably, Cinamon et al. argued that apical
chemokines on vessel endothelia attract lymphocytes, allowing their migration through ECL by a process denominated
transendothelial migration (TEM) [103]. If CLL cells are
capable of undergoing TEM, they may transiently undergo
co-option before reaching their niches. Co-option is the process in which, without inducing development of new blood
vessels, tumour cells profit from close proximity to blood
capillaries [104]. Upon compromising the ECL, CLL cells
could undergo TEM, remaining transiently and closely associated with the ECL whilst profiting from co-option (Fig. 2).
By further secreting angiogenic factors, or by interacting
with those available at their surroundings ECL, it is possible to infer that CLL cells modulate their surroundings, thus
facilitating their transport, proliferation, and evasion from
apoptosis and treatment.
Whilst VEGF, bFGF, and PDGF are among the most relevant angiogenic factors in CLL, others such as leptin, G-CSF,
follistatin, Ang1, ANG, MK, PTN, and PGRN are emerging novel factors that regulate angiogenic related process
that determine the fate of CLL molecular physiology. The
nature of PLF, Del-1, and PIGF on CLL pathophysiology is
not understood, but further studies will clarify the extent in
which they modulate survival, proliferation and escape from
apoptosis.
Certainly, the integral molecular understanding of molecular communication between angiogenic factors and their
influence on CLL pathophysiology will help develop effective treatments against CLL. Only then will we be able
to develop drugs that exclusively and only modulate the
Reviewers
Prof Eric Eldering: Meibergdreef 9, Amsterdam, The
Netherlands.
Prof Krzysztof Giannopoulos: Medical University of
Lublin, Chodzki 4a, Lublin, Poland.
Acknowledgements
We are deeply grateful to Mr. Kearnan Welch, MS (Touro
University California), for his critical comments on this
manuscript. This work was kindly supported by a grant (No.
2011.101.02) from the Wilhelm Sander-Foundation, Munich,
Germany.
References
[1] Folkman J. In: Brenner Sydney, Miller Jeffrey H, editors. Encyclopedia of genetics. New York, NY: Academic Press; 2001. p. 6673.
[2] De Falco S. The discovery of placenta growth factor and its biological
activity. Exp Mol Med 2012;44(1):19.
[3] Albitar M. Angiogenesis in acute myeloid leukemia and myelodysplastic syndrome. Acta Haematol 2001;106(4):1706.
[4] Hallek M. Chronic lymphocytic leukemia: 2013 update on diagnosis,
risk stratification and treatment. Am J Hematol 2013;88(9):80316.
[5] Kini AR, Kay NE, Peterson LC. Increased bone marrow angiogenesis in B cell chronic lymphocytic leukemia. Leukemia
2000;14(8):14148.
[6] Peterson L, Kini AR, Kay N. Angiogenesis is increased in B-cell
chronic lymphocytic leukemia. Blood 2001;97(8):252930.
[7] Piechnik A, Dmoszynska A, Omiotek M, et al. The VEGF receptor,
neuropilin-1, represents a promising novel target for chronic lymphocytic leukemia patients. Int J Cancer 2013;133(6):148996.
[8] Saharinen P, Eklund L, Pulkki K, Bono P, Alitalo K. VEGF and
angiopoietin signaling in tumor angiogenesis and metastasis. Trends
Mol Med 2011;17(7):34762.
[9] Kerbel RS. Tumor angiogenesis. N Engl J Med 2008;358(19):
203949.
234
L.M. Aguirre Palma et al. / Critical Reviews in Oncology/Hematology 93 (2015) 225236
[10] Shibuya M, Claessonwelsh L. Signal transduction by VEGF receptors
in regulation of angiogenesis and lymphangiogenesis. Exp Cell Res
2006;312(5):54960.
[11] Ayad MW, El Naggar AA. Angiogenic factor VEGF and its relationship with biological prognostic markers in chronic lymphocytic
leukemia. Egypt J Immunol Egypt Assoc Immunol 2010;17(1):5971.
[12] Ferrara N, Hillan KJ, Gerber H-P, Novotny W. Case history: discovery
and development of bevacizumab, an anti-VEGF antibody for treating
cancer. Nat Rev Drug Discovery 2004;3(5):391400.
[13] Bogusz J, Majchrzak A, Medra A, Cebula-Obrzut B, Robak T,
Smolewski P. Mechanisms of action of the anti-VEGF monoclonal antibody bevacizumab on chronic lymphocytic leukemia cells.
Postepy Hig Med Dosw (Online) 2013;67:10718.
[14] Bairey O, Boycov O, Kaganovsky E, Zimra Y, Shaklai M, Rabizadeh
E. All three receptors for vascular endothelial growth factor (VEGF)
are expressed on B-chronic lymphocytic leukemia (CLL) cells. Leuk
Res 2004;28(3):2438.
[15] Gehrke I, Gandhirajan RK, Poll-Wolbeck SJ, Hallek M, Kreuzer K-A.
Bone marrow stromal cell-derived vascular endothelial growth factor
(VEGF) rather than chronic lymphocytic leukemia (CLL) cell-derived
VEGF is essential for the apoptotic resistance of cultured CLL cells.
Mol Med Camb Mass 2011;17(7-8):61927.
[16] Lozano-Santos C, Martinez-Velasquez J, Fernandez-Cuevas B, et al.
Vascular endothelial growth factor A (VEGFA) gene polymorphisms
have an impact on survival in a subgroup of indolent patients with
chronic lymphocytic leukemia. PLoS One 2014;9(6).
[17] Wrbel T, Mazur G, Dzietczenia J, Gebura K, Kuliczkowski
K, Bogunia-Kubik K. VEGF and bFGF gene polymorphisms in
Polish patients with B-CLL. Med Oncol Northwood Lond Engl
2013;30(1):456.
[18] Baban D, Murray J, Earl H, Kerr D, Seymour L. Quantitative analysis
of vascular endothelial growth factor expression in chronic lymphocytic leukaemia. Int J Oncol 1996;8(1):2934.
[19] Molica S, Vitelli G, Levato D, Gandolfo GM, Liso V. Increased serum
levels of vascular endothelial growth factor predict risk of progression in early B-cell chronic lymphocytic leukaemia. Br J Haematol
1999;107(3):60510.
[20] Hicklin DJ, Ellis LM. Role of the vascular endothelial growth
factor pathway in tumor growth and angiogenesis. J Clin Oncol
2005;23(5):101127.
[21] Itoh N, Ornitz DM. Fibroblast growth factors: from molecular evolution to roles in development, metabolism and disease. J Biochem
(Tokyo) 2011;149(2):12130.
[22] Katoh M. Network of WNT and other regulatory signaling cascades in
pluripotent stem cells and cancer stem cells. Curr Pharm Biotechnol
2011;12(2):16070.
[23] Aguayo A, Kantarjian H, Manshouri T, et al. Angiogenesis in
acute and chronic leukemias and myelodysplastic syndromes. Blood
2000;96(6):22405.
[24] Smolej L, Andrys C, Maisnar V, Pour L, Maly J. Plasma concentrations of vascular endothelial growth factor and basic fibroblast growth
factor in lymphoproliferative disorders. Acta Medica Hradec Krl
Univ Carol Fac Medica Hradec Krl 2005;48(1):578.
[25] Menzel T, Rahman Z, Calleja E, et al. Elevated intracellular level of
basic fibroblast growth factor correlates with stage of chronic lymphocytic leukemia and is associated with resistance to fludarabine.
Blood 1996;87(3):105663.
[26] Knig A, Menzel T, Lynen S, et al. Basic fibroblast growth factor
(bFGF) upregulates the expression of bcl-2 in B cell chronic lymphocytic leukemia cell lines resulting in delaying apoptosis. Leukemia
1997;11(2):25865.
[27] Smolej L, Andrys C, Krejsek J, et al. Basic fibroblast growth factor
(bFGF) and vascular endothelial growth factor (VEGF) are elevated
in peripheral blood plasma of patients with chronic lymphocytic
leukemia and decrease after intensive fludarabine-based treatment.
Vnitrn Lkarstv 2007;53(11):11716.
[28] Chanan-Khan A, Miller KC, Musial L, et al. Clinical efficacy
of lenalidomide in patients with relapsed or refractory chronic
lymphocytic leukemia: results of a phase II study. J Clin Oncol
2006;24(34):53439.
[29] Maffei R, Fiorcari S, Bulgarelli J, et al. Endothelium-mediated survival of leukemic cells and angiogenesis-related factors are affected
by lenalidomide treatment in chronic lymphocytic leukemia. Exp
Hematol 2013;42(2):12636.
[30] Li H, Fredriksson L, Li X, Eriksson U. PDGF-D is a potent transforming and angiogenic growth factor. Oncogene 2003;22(10):150110.
[31] Antoniades HN, Scher CD, Stiles CD. Purification of human
platelet-derived growth factor. Proc Natl Acad Sci USA 1979;76(4):
180913.
[32] Zhang X, Nie D, Chakrabarty S. Growth factors in tumor microenvironment. Front Biosci J Virtual Libr 2010;15:15165.
[33] Dong J, Grunstein J, Tejada M, et al. VEGF-null cells require PDGFR?
signaling-mediated stromal fibroblast recruitment for tumorigenesis.
EMBO J 2004;23(14):280010.
[34] Kwon HJ, Kim G-E, Lee YT, et al. Inhibition of platelet-derived
growth factor receptor tyrosine kinase and downstream signaling
pathways by Compound C. Cell Signal 2013;25(4):88397.
[35] Ho C-L, Hsu L-F, Phyliky RL, Li C-Y. Autocrine expression of
platelet-derived growth factor B in B cell chronic lymphocytic
leukemia. Acta Haematol 2005;114(3):13340.
[36] Ding W, Knox TR, Tschumper RC, et al. Platelet-derived
growth factor (PDGF)-PDGF receptor interaction activates bone
marrow-derived mesenchymal stromal cells derived from chronic
lymphocytic leukemia: implications for an angiogenic switch. Blood
2010;116(16):298493.
[37] Gialeli C, Nikitovic D, Kletsas D, Theocharis AD, Tzanakakis
GN, Karamanos NK. PDGF/PDGFR signaling and targeting in cancer growth and progression: focus on tumor microenvironment and
cancer-associated fibroblasts. Curr Pharm Des 2013;20(17):28438.
[38] Malavaki CJ, Roussidis AE, Gialeli C, et al. Imatinib as a key inhibitor
of the platelet-derived growth factor receptor mediated expression of
cell surface heparan sulfate proteoglycans and functional properties
of breast cancer cells. FEBS J 2013;280(10):247789.
[39] Zhang Y, Proenca R, Maffei M, Barone M, Leopold L, Friedman JM.
Positional cloning of the mouse obese gene and its human homologue.
Nature 1994;372(6505):42532.
[40] Garofalo C, Surmacz E. Leptin and cancer. J Cell Physiol
2006;207(1):1222.
[41] Lam QLK, Wang S, Ko OKH, Kincade PW, Lu L. Leptin signaling
maintains B-cell homeostasis via induction of Bcl-2 and Cyclin D1.
Proc Natl Acad Sci USA 2010;107(31):138127.
[42] Sierra-Honigmann MR, Nath AK, Murakami C, et al. Biological action of leptin as an angiogenic factor. Science
1998;281(5383):16836.
[43] Bennett BD, Solar GP, Yuan JQ, Mathias J, Thomas GR, Matthews
W. A role for leptin and its cognate receptor in hematopoiesis. Curr
Biol (CB) 1996;6(9):117080.
[44] Pamuk GE, Demir M, Harmandar F, Yesil Y, Turgut B, Vural O.
Leptin and resistin levels in serum of patients with hematologic
malignancies: correlation with clinical characteristics. Exp Oncol
2006;28(3):2414.
[45] Dalamaga M, Crotty BH, Fargnoli J, et al. B-cell chronic lymphocytic leukemia risk in association with serum leptin and adiponectin
levels: a case-control study in Greece. Cancer Causes Control (CCC)
2010;21(9):14519.
[46] Avalos BR. Molecular analysis of the granulocyte colony-stimulating
factor receptor. Blood 1996;88(3):76177.
[47] Demetri GD, Griffin JD. Granulocyte colony-stimulating factor and
its receptor. Blood 1991;78(11):2791808.
[48] Bennett CL, Djulbegovic B, Norris LB, Armitage JO. Colonystimulating factors for febrile neutropenia during cancer therapy. N
Engl J Med 2013;368(12):11319.
L.M. Aguirre Palma et al. / Critical Reviews in Oncology/Hematology 93 (2015) 225236
[49] Martino M, Fedele R, Massara E, Recchia AG, Irrera G, Morabito F.
Long-term safety of granulocyte colony-stimulating factor in normal
donors: is it all clear? Expert Opin Biol Ther 2012;12(5):60921.
[50] Calandra G, Bridger G, Fricker S. CXCR4 in clinical hematology.
In: Bruserud O, editor. The chemokine system in experimental and
clinical hematology. Current topics in microbiology and immunology.
Berlin Heidelberg: Springer; 2010. p. 17391.
[51] Gruber M, Fleiss K, Porpaczy E, et al. Prolonged progressionfree survival in patients with chronic lymphocytic leukemia
receiving granulocyte colony-stimulating factor during treatment
with fludarabine, cyclophosphamide, and rituximab. Ann Hematol
2011;90(10):11316.
[52] Bartholin L, Guindon S, Martel S, Corbo L, Rimokh R. Identification
of NF-kappaB responsive elements in follistatin related gene (FLRG)
promoter. Gene 2007;393(12):15362.
[53] Maguer-Satta V, Bartholin L, Jeanpierre S, et al. During
hematopoiesis, expression of FLRG, a novel activin A ligand, is
regulated by TGF-. Exp Hematol 2001;29(3):3018.
[54] De Kretser DM, OHehir RE, Hardy CL, Hedger MP. The roles of
activin A and its binding protein, follistatin, in inflammation and tissue
repair. Mol Cell Endocrinol 2012;359(12):1016.
[55] Phillips DJ. Regulation of activins access to the cell: why is Mother
Nature such a control freak? BioEssays 2000;22(8):68996.
[56] Bartholin L, Maguer-Satta V, Hayette S, et al. Transcription activation
of FLRG and follistatin by activin A, through Smad proteins, participates in a negative feedback loop to modulate activin A function.
Oncogene 2002;21(14):222735.
[57] Hayette S, Gadoux M, Martel S, et al. FLRG (follistatin-related gene),
a new target of chromosomal rearrangement in malignant blood disorders. Oncogene 1998;16(22):294954.
[58] Zipori D, Barda-Saad M. Role of activin A in negative regulation
of normal and tumor B lymphocytes. J Leukoc Biol 2001;69(6):
86773.
[59] Maguer-Satta V, Rimokh R. FLRG, member of the follistatin
family, a new player in hematopoiesis. Mol Cell Endocrinol
2004;225(12):10918.
[60] Kawaguchi M, Sugaya M, Suga H, et al. Serum levels of angiopoietin2, but not angiopoietin-1, are elevated in patients with erythrodermic
cutaneous T-cell lymphoma. Acta Derm Venereol 2013.
[61] Yu X, Seegar TCM, Dalton AC, et al. Structural basis for
angiopoietin-1mediated signaling initiation. Proc Natl Acad Sci
USA 2013;110(18):720510.
[62] Moss A. The angiopoietin:Tie 2 interaction: a potential target for
future therapies in human vascular disease. Cytokine Growth Factor
Rev 2013;24(6):57992.
[63] Seegar TCM, Eller B, Tzvetkova-Robev D, et al. Tie1Tie2 interactions mediate functional differences between angiopoietin ligands.
Mol Cell 2010;37(5):64355.
[64] Martinelli S, Kanduri M, Maffei R, et al. ANGPT2 promoter methylation is strongly associated with gene expression and prognosis in
chronic lymphocytic leukemia. Epigenetics 2013;8(7).
[65] Maffei R, Martinelli S, Castelli I, et al. Increased angiogenesis induced
by chronic lymphocytic leukemia B cells is mediated by leukemiaderived Ang2 and VEGF. Leuk Res 2010;34(3):31221.
[66] Maffei R, Martinelli S, Santachiara R, et al. Angiopoietin-2 plasma
dosage predicts time to first treatment and overall survival in chronic
lymphocytic leukemia. Blood 2010;116(4):58492.
[67] Kay NE, Bone ND, Tschumper RC, et al. B-CLL cells are capable of
synthesis and secretion of both pro- and anti-angiogenic molecules.
Leukemia 2002;16(5):9119.
[68] Musolino C, Alonci A, Bellomo G, et al. Levels of soluble angiogenin in chronic myeloid malignancies: clinical implications. Eur J
Haematol 2004;72(6):4169.
[69] Thiyagarajan N, Acharya KR. Crystal structure of human angiogenin
with an engineered loop exhibits conformational flexibility at the
functional regions of the molecule. FEBS Open Biol 2012;3:6570.
235
[70] Gao X, Xu Z. Mechanisms of action of angiogenin. Acta Biochim
Biophys Sin 2008;40(7):61924.
[71] Molica S, Vitelli G, Levato D, et al. Serum angiogenin is not elevated in patients with early B-cell chronic lymphocytic leukemia
but is prognostic factor for disease progression. Eur J Haematol
2004;73(1):3642.
[72] Pavlov N, Badet J. Langiognine: implication dans langiogense et
le dveloppement tumoral. Bull Cancer (Paris) 2001;88(8):72532.
[73] Gao X, Hu H, Zhu J, Xu Z. Identification and characterization
of follistatin as a novel angiogenin-binding protein. FEBS Lett
2007;581(28):550510.
[74] Cohen S, Shoshana O, Zelman-Toister E, et al. The cytokine midkine
and its receptor RPTP? Regulate B cell survival in a pathway induced
by CD74. J Immunol (Baltimore, MD: 1950) 2012;188(1):25969.
[75] Kadomatsu K, Hagihara M, Akhter S, Fan QW, Muramatsu H, Muramatsu T. Midkine induces the transformation of NIH3T3 cells. Br J
Cancer 1997;75(3):3549.
[76] Shachar I, Cohen S, Marom A, Becker-Herman S. Regulation of CLL
survival by hypoxia-inducible factor and its target genes. FEBS Lett
2012;586(18):290610.
[77] Hidaka H, Yagasaki H, Takahashi Y, et al. Increased midkine gene
expression in childhood B-precursor acute lymphoblastic leukemia.
Leuk Res 2007;31(8):104551.
[78] Ohuchida T, Okamoto K, Akahane K, et al. Midkine protects hepatocellular carcinoma cells against TRAIL-mediated apoptosis through
down-regulation of caspase-3 activity. Cancer 2004;100(11):24306.
[79] Besse S, Comte R, Frchault S, Courty J, Jol de L, Delb J.
Pleiotrophin promotes capillary-like sprouting from senescent aortic
rings. Cytokine 2013;62(1):447.
[80] Mikelis C, Sfaelou E, Koutsioumpa M, Kieffer N, Papadimitriou E.
Integrin 3 is a pleiotrophin receptor required for pleiotrophininduced endothelial cell migration through receptor protein tyrosine
phosphatase /. FASEB J 2009;23(5):145969.
[81] Kong Y, Bai P, Nan K, Sun H, Chen N, Qi X. Pleiotrophin is a potential
colorectal cancer prognostic factor that promotes VEGF expression
and induces angiogenesis in colorectal cancer. Int J Colorectal Dis
2012;27(3):28798.
[82] Du C, Wang L, Li Y, et al. Elevated expression of pleiotrophin in
lymphocytic leukemia CD19+ B cells. APMIS 2014;122(10):90513.
[83] Lu Y, Zheng L, Zhang W, et al. Growth factor progranulin contributes
to cervical cancer cell proliferation and transformation in vivo and in
vitro. Gynecol Oncol 2014;134(2):36471.
[84] DeMorrow S. Progranulin: a novel regulator of gastrointestinal cancer
progression. Transl Gastrointest Cancer 2013;2(3):14551.
[85] Tang W, Lu Y, Tian Q-Y, et al. The growth factor progranulin binds to
tnf receptors and is therapeutic against inflammatory arthritis in mice.
Science 2011;332(6028):47884.
[86] Maas C, Tromp JM, van Laar J, et al. CLL cells are resistant to smac
mimetics because of an inability to form a ripoptosome complex. Cell
Death Dis 2013;4(8):e782.
[87] Gbel M, Eisele L, Mllmann M, et al. Progranulin is a novel independent predictor of disease progression and overall survival in chronic
lymphocytic leukemia. PLoS One 2013;8(8):e72107.
[88] Toft DJ, Rosenberg SB, Bergers G, Volpert O, Linzer DIH.
Reactivation of proliferin gene expression is associated with increased
angiogenesis in a cell culture model of fibrosarcoma tumor progression. Proc Natl Acad Sci USA 2001;98(23):130559.
[89] El-Shewy HM, Luttrell LM. Insulin-like growth factor-2/mannose-6
phosphate receptors. In: Gerald Litwack, editor. Vitamins & Hormones. Insulin and IGFs, vol. 80. Oxford, UK: Academic Press; 2009.
p. 66797 (Chapter 24).
[90] Vignon F, Rochefort H. Interactions of pro-cathepsin D and IGF-II
on the mannose-6-phosphate/IGF-II receptor. Breast Cancer Res Treat
1992;22(1):4757.
[91] Yang X, Qiao D, Meyer K, Pier T, Keles S, Friedl A. Angiogenesis induced by signal transducer and activator of transcription 5A
236
[92]
[93]
[94]
[95]
[96]
[97]
[98]
[99]
[100]
[101]
[102]
[103]
[104]
[105]
[106]
[107]
[108]
[109]
[110]
[111]
[112]
L.M. Aguirre Palma et al. / Critical Reviews in Oncology/Hematology 93 (2015) 225236
(STAT5A) is dependent on autocrine activity of proliferin. J Biol
Chem 2012;287(9):6490502.
Hanayama R, Tanaka M, Miwa K, Nagata S. Expression of developmental endothelial locus-1 in a subset of macrophages for engulfment
of apoptotic cells. J Immunol 2004;172(6):387682.
Kim K-J, Cho C-S, Kim W-U. Role of placenta growth factor in cancer
and inflammation. Exp Mol Med 2012;44(1):109.
Reinart N, Nguyen P-H, Boucas J, et al. Delayed development of
chronic lymphocytic leukemia in the absence of macrophage migration inhibitory factor. Blood 2013;121(5):81221.
Maffei R, Bulgarelli J, Fiorcari S, et al. The monocytic population in chronic lymphocytic leukemia shows altered composition and
deregulation of genes involved in phagocytosis and inflammation.
Haematologica 2013;98(7):111523.
Nielsen DL, Sengelv L. Inhibition of placenta growth factor with
TB-403: a novel antiangiogenic cancer therapy. Exp Opin Biol Ther
2012;12(6):795804.
Zins K, Thomas A, Lucas T, Sioud M, Aharinejad S, Abraham D.
Inhibition of stromal PLGF suppresses the growth of prostate cancer
xenografts. Int J Mol Sci 2013;14(9):1795871.
Munnink THO, Tamas KR, Hooge MNL, et al. Placental growth factor
(PlGF)specific uptake in tumor microenvironment of 89Zr-labeled
PlGF antibody RO5323441. J Nucl Med 2013;54(6):92935.
Ho H-KV, Jang JJ, Kaji S, et al. Developmental endothelial locus-1
(Del-1), a novel angiogenic protein its role in ischemia. Circulation
2004;109(10):13149.
Aoka Y, Johnson FL, Penta K, et al. The embryonic angiogenic factor Del1 accelerates tumor growth by enhancing vascular formation.
Microvasc Res 2002;64(1):14861.
Ciucurel EC, Sefton MV. Del-1 overexpression in endothelial cells
increases vascular density in tissue-engineered implants containing
endothelial cells and adipose-derived mesenchymal stromal cells.
Tissue Eng, A 2013;20(7-8):123552.
Kay NE, Shanafelt TD, Strege AK, Lee YK, Bone ND, Raza A. Bone
biopsy derived marrow stromal elements rescue chronic lymphocytic
leukemia B-cells from spontaneous and drug induced cell death and
facilitates an angiogenic switch. Leuk Res 2007;31(7):899906.
Cinamon G, Shinder V, Alon R. Shear forces promote lymphocyte
migration across vascular endothelium bearing apical chemokines.
Nat Immunol 2001;2(6):51522.
Eikesdal HP, Kalluri R. Drug resistance associated with antiangiogenesis therapy. Semin Cancer Biol 2009;19(5):3107.
Haugsten EM, Wiedlocha A, Olsnes S, Wesche J. Roles of fibroblast growth factor receptors in carcinogenesis. Mol Cancer Res
2010;8(11):143952.
Bouloumi A, Drexler HCA, Lafontan M, Busse R. Leptin, the product of Ob gene, promotes angiogenesis. Circ Res
1998;83(10):105966.
Malli F, Papaioannou AI, Gourgoulianis KI, Daniil Z. The role of leptin in the respiratory system: an overview. Respir Res 2010;11(1):152.
Krneta J, Kroll J, Alves F, et al. Dissociation of angiogenesis and
tumorigenesis in follistatin- and activin-expressing tumors. Cancer
Res 2006;66(11):568695.
Davis S, Aldrich TH, Jones PF, et al. Isolation of angiopoietin-1, a
ligand for the TIE2 receptor, by secretion-trap expression cloning.
Cell 1996;87(7):11619.
Dumont DJ, Gradwohl G, Fong GH, et al. Dominant-negative and
targeted null mutations in the endothelial receptor tyrosine kinase,
tek, reveal a critical role in vasculogenesis of the embryo. Genes Dev
1994;8(16):1897909.
Jones N, Chen SH, Sturk C, et al. A unique autophosphorylation site on
Tie2/Tek mediates Dok-R phosphotyrosine binding domain binding
and function. Mol Cell Biol 2003;23(8):265868.
Tadros A, Hughes DP, Dunmore BJ, Brindle NPJ. ABIN-2 protects
endothelial cells from death and has a role in the antiapoptotic effect
of angiopoietin-1. Blood 2003;102(13):44079.
[113] Dai L-C. Midkine translocated to nucleoli and involved in carcinogenesis. World J Gastroenterol (WJG) 2009;15(4):4126.
[114] You Z, Dong Y, Kong X, Beckett LA, Gandour-Edwards R, Melamed
J. Midkine is a NF-?B-inducible gene that supports prostate cancer
cell survival. BMC Med Genomics 2008;1:6.
[115] Koutsioumpa M, Drosou G, Mikelis C, et al. Pleiotrophin expression
and role in physiological angiogenesis in vivo: potential involvement
of nucleolin. Vasc Cell 2012;4:4.
[116] Polykratis A, Katsoris P, Courty J, Papadimitriou E. Characterization
of heparin affin regulatory peptide signaling in human endothelial
cells. J Biol Chem 2005;280(23):2245461.
[117] He Z, Bateman A. Progranulin (granulin-epithelin precursor, PCcell-derived growth factor, acrogranin) mediates tissue repair and
tumorigenesis. J Mol Med 2003;81(10):60012.
[118] Serrero G. Autocrine growth factor revisited: PC-cell-derived growth
factor (progranulin), a critical player in breast cancer tumorigenesis.
Biochem Biophys Res Commun 2003;308(3):40913.
[119] Brockman JL, Schroeder MD, Schuler LA. PRL activates the
cyclin D1 promoter via the Jak2/stat pathway. Mol Endocrinol
2002;16(4):77484.
[120] Yang X, Zhang Y, Yang Y, et al. Vascular endothelial growth factordependent spatiotemporal dual roles of placental growth factor in
modulation of angiogenesis and tumor growth. Proc Natl Acad Sci
USA 2013;110(34):139327.
[121] Fischer C, Jonckx B, Mazzone M, et al. Anti-PlGF inhibits growth
of VEGF(R)inhibitor-resistant tumors without affecting healthy
vessels. Cell 2007;131(3):46375.
[122] Penta K, Varner JA, Liaw L, Hidai C, Schatzman R, Quertermous
T. Del1 induces integrin signaling and angiogenesis by ligation of
V3. J Biol Chem 1999;274(16):111019.
Biography
Karl-Anton Kreuzer studied medicine at the University
of Bonn and the Technical University of Munich, as well as in
Pittsburgh, PA, USA, and Zurich, Switzerland. He furthered
his scientific training at the Wistar Institute in Philadelphia,
PA, USA and the Weizmann Institute of Science in Rehovot,
Israel. Under the supervision of Prof. Dr. Dieter Huhn he
underwent his residency at the Rudolf Virchow University
Clinic of Charit, Berlin. Since 2004 he focuses in haematology, oncology, internal medicine research, and diagnostics at
the Department of Internal Medicine I at University Clinic of
Cologne. In addition, Prof. Kreuzer is one of the directors of
the Interdisciplinary Oncology Project of Acute Leukaemia
and Myelodysplastic Syndromes of the Centre for Integral
Oncology of Cologne-Bonn (CIO). Currently he directs the
Laboratory of Molecular Haematology and Oncology at the
Clinic of the University of Cologne, a laboratory focused on
haematological diagnostics comprising cytogenetics, molecular genetics, flow cytometry, morphology, and a research
facility focusing on understanding angiogenesis and cellular
stress in chronic lymphocytic leukaemia (CLL). As member of several internationally renowned medical societies,
Prof. Kreuzer serves as consultant to international research
institutions and is author and co-author of multiple publications in the fields of haematology, oncology, and internal
medicine.
You might also like
- Applied Energy: Selvakumar Thiruvenkadam, Shamsul Izhar, Hiroyuki Yoshida, Michael K. Danquah, Razif HarunDocument14 pagesApplied Energy: Selvakumar Thiruvenkadam, Shamsul Izhar, Hiroyuki Yoshida, Michael K. Danquah, Razif HarunAgustine Christela MelvianaNo ratings yet
- City of Weed Love's Travel Stop Draft EIR IDocument8 pagesCity of Weed Love's Travel Stop Draft EIR Iapi-437859414No ratings yet
- An Evaluation of Fishing Activities at Kasenyi Fish Landing Site Along The Northern Shores of L.victoria (2000-2004)Document46 pagesAn Evaluation of Fishing Activities at Kasenyi Fish Landing Site Along The Northern Shores of L.victoria (2000-2004)Denis Tumusiime100% (4)
- Similar But Not The Same Differential Diagnosis of HLH and SepsisDocument12 pagesSimilar But Not The Same Differential Diagnosis of HLH and SepsisJuan JoséNo ratings yet
- Rizzieri 2016Document13 pagesRizzieri 2016alinamatei1000000No ratings yet
- Report On The Status of Major Health Risk Factors For Noncommunicable Diseases: WHO African Region, 2015Document88 pagesReport On The Status of Major Health Risk Factors For Noncommunicable Diseases: WHO African Region, 2015GhislainNo ratings yet
- Rezistenta Antimicrobiana in EuropaDocument208 pagesRezistenta Antimicrobiana in EuropairiscelNo ratings yet
- Structure and Biological Activities of The Polysaccharides From The Leaves, Roots and Fruits of Panax Ginseng C.A. Meyer: An OverviewDocument10 pagesStructure and Biological Activities of The Polysaccharides From The Leaves, Roots and Fruits of Panax Ginseng C.A. Meyer: An OverviewAlfredo de la CruzNo ratings yet
- Antimicrobial Resistance: A Global Report On SurveillanceDocument256 pagesAntimicrobial Resistance: A Global Report On SurveillanceJonathanKealing100% (3)
- Anaerobic Digestion of Solid Organic Substrates in Batch Mode An Overview Relating To Methane Yields and Experimental Procedures 2012 Renewable and Sustainable Energy ReviewsDocument17 pagesAnaerobic Digestion of Solid Organic Substrates in Batch Mode An Overview Relating To Methane Yields and Experimental Procedures 2012 Renewable and Sustainable Energy ReviewsLinnaZuluagaNo ratings yet
- Rehabilitation of Muscle Dysfunction in HemophiliaDocument14 pagesRehabilitation of Muscle Dysfunction in HemophiliadavidcorzoNo ratings yet
- International Journal of Pediatric OtorhinolaryngologyDocument10 pagesInternational Journal of Pediatric Otorhinolaryngologysangar_girl5133No ratings yet
- Protein Aggregation and Inhibition in Bio PharmaceuticsDocument30 pagesProtein Aggregation and Inhibition in Bio PharmaceuticsFatima Herranz Trillo100% (2)
- Hepatitis B C SurveillanceDocument64 pagesHepatitis B C SurveillanceAli AlisonNo ratings yet
- Dissertation No RestrictionDocument135 pagesDissertation No RestrictioniramshaguftaNo ratings yet
- 2 - Production, Recovery and Applications of Xanthan GumDocument12 pages2 - Production, Recovery and Applications of Xanthan GumJuan Daniel Guaqueta100% (1)
- Hepatitis B C Surveillance Europe 2012 July 2014Document64 pagesHepatitis B C Surveillance Europe 2012 July 2014mihaela bogdanNo ratings yet
- BiofarDocument14 pagesBiofarAl Pharux Ox-CygenNo ratings yet
- EIA Final ReportDocument62 pagesEIA Final ReportAquaquam Tube100% (1)
- 10 1016@j Critrevonc 2016 06 003 PDFDocument14 pages10 1016@j Critrevonc 2016 06 003 PDFlengers poworNo ratings yet
- Review in Electrospinning 2Document25 pagesReview in Electrospinning 2Muaathe IbrahimNo ratings yet
- PUP Student HandbookDocument29 pagesPUP Student HandbookMichael PagaduanNo ratings yet
- Process Simulation Model For A Staged, Fluidized-Bed Oil-Shale Retort With Lift-Pipe CombustorDocument31 pagesProcess Simulation Model For A Staged, Fluidized-Bed Oil-Shale Retort With Lift-Pipe CombustorAljay Neeson ImperialNo ratings yet
- Diving O&g411Document52 pagesDiving O&g411phsemNo ratings yet
- PDF Daftar Isi Dan Pembatas Dokumen Csmsdocx - CompressDocument70 pagesPDF Daftar Isi Dan Pembatas Dokumen Csmsdocx - Compresshsse.patriagroupNo ratings yet
- Encapsulation of Probiotic Living Cells From Laboratory Scale To Industrial - Burgarin, 2011Document17 pagesEncapsulation of Probiotic Living Cells From Laboratory Scale To Industrial - Burgarin, 2011rock2312No ratings yet
- Guia Esvs Manejo Evc 2015Document60 pagesGuia Esvs Manejo Evc 2015Steeven Ruilova Valle100% (1)
- Total Life Academ ScienceDocument4 pagesTotal Life Academ ScienceRolly RollyNo ratings yet
- Atherosclerosis: Review QDocument9 pagesAtherosclerosis: Review QAsri RachmawatiNo ratings yet
- Tuberculosis Infection: Gamma Interferon Release Assays For Detection of MycobacteriumDocument18 pagesTuberculosis Infection: Gamma Interferon Release Assays For Detection of MycobacteriumLinda MaylianaNo ratings yet
- A Brief History of Tuberculosis Control: in KenyaDocument32 pagesA Brief History of Tuberculosis Control: in KenyaNiharikaNo ratings yet
- Environmental and Social Consideration TanayDocument246 pagesEnvironmental and Social Consideration Tanayfranz ramosNo ratings yet
- Litio en Cauchari PDFDocument387 pagesLitio en Cauchari PDFJoni Guanca100% (1)
- Raj Mohan Raja Muthiah 08Document245 pagesRaj Mohan Raja Muthiah 08Agustin BernacchiaNo ratings yet
- The Biology Of: Trifolium Repens L. (White Clover)Document41 pagesThe Biology Of: Trifolium Repens L. (White Clover)ROBERTO MIRANDA CALDASNo ratings yet
- Mip As BiosensorDocument15 pagesMip As Biosensorhareesh13hNo ratings yet
- Texaco Gasification Process PDFDocument90 pagesTexaco Gasification Process PDFBun YaminNo ratings yet
- Critical Reviews in Oncology/Hematology: Sandro Barni, Fausto Petrelli, Mary CabidduDocument10 pagesCritical Reviews in Oncology/Hematology: Sandro Barni, Fausto Petrelli, Mary Cabiddubenny christantoNo ratings yet
- On Dance TronDocument10 pagesOn Dance TronBenny Chris TantoNo ratings yet
- Renewable and Sustainable Energy Reviews: Pablo Del Rı O, Mercedes BurguilloDocument12 pagesRenewable and Sustainable Energy Reviews: Pablo Del Rı O, Mercedes BurguilloJanus Van AsNo ratings yet
- Seino Van Breugel-A Grammar of Atong PDFDocument753 pagesSeino Van Breugel-A Grammar of Atong PDFDylan StillwoodNo ratings yet
- Melikoglu-Shale Gas-Analysis of Its Role in The Global Energy MarketDocument9 pagesMelikoglu-Shale Gas-Analysis of Its Role in The Global Energy MarketCarlos GomezNo ratings yet
- Journal P 2Document16 pagesJournal P 2nurahmi widyani ratriNo ratings yet
- Biobutanol Production ChallengesDocument17 pagesBiobutanol Production ChallengesSussan VillamizarNo ratings yet
- GK HyperloopDocument29 pagesGK HyperloopAjitNo ratings yet
- DNAL Livro PDFDocument369 pagesDNAL Livro PDFAnonymous hhLREXRhLNo ratings yet
- tmpF69A TMPDocument21 pagestmpF69A TMPFrontiersNo ratings yet
- Effectiveness of Homeopathy For Clinical Conditions - Evaluation of The Evidence PDFDocument301 pagesEffectiveness of Homeopathy For Clinical Conditions - Evaluation of The Evidence PDFYaniv AlgrablyNo ratings yet
- Golder ReportDocument91 pagesGolder ReportMark Joseph AbelleraNo ratings yet
- Barreras en El Crebro en DesarrolloDocument19 pagesBarreras en El Crebro en DesarrolloAlvarez Flores GilmerNo ratings yet
- BIA MarsyangdiDocument139 pagesBIA Marsyangdivijay guptaNo ratings yet
- The International Journal of Biochemistry & Cell BiologyDocument15 pagesThe International Journal of Biochemistry & Cell BiologyNathalia PietraniNo ratings yet
- Epidemiology Methods and Uses Complete Master FileDocument55 pagesEpidemiology Methods and Uses Complete Master Filefrsh4u.comNo ratings yet
- 4Document13 pages4Juan Carlos Hernandez CriadoNo ratings yet
- Pollution Prevention: Methodology, Technologies and PracticesFrom EverandPollution Prevention: Methodology, Technologies and PracticesNo ratings yet
- Re-Cording Lives: Governing Asylum in Switzerland and the Need to ResolveFrom EverandRe-Cording Lives: Governing Asylum in Switzerland and the Need to ResolveNo ratings yet
- Cardiothoracic Care for Children and Young People: A Multidisciplinary ApproachFrom EverandCardiothoracic Care for Children and Young People: A Multidisciplinary ApproachKerry CookNo ratings yet