Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5822)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Drift of A Body Floating On WavesDocument11 pagesThe Drift of A Body Floating On WavesvictorNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Saudi Aramco Engineering Standards-Electrical-CommissioningDocument61 pagesSaudi Aramco Engineering Standards-Electrical-Commissioningsyedsalmanali9193% (15)
- Primary ImpressionDocument18 pagesPrimary ImpressionJewana J. Ghazal67% (3)
- 3A Crystal StructureDocument70 pages3A Crystal StructureIvy TovilloNo ratings yet
- Capping Cusps With Amalgam (Last Edi)Document12 pagesCapping Cusps With Amalgam (Last Edi)Jewana J. GhazalNo ratings yet
- Periodontal Examination and Clinical Indices: Why Do We Do Examination?Document13 pagesPeriodontal Examination and Clinical Indices: Why Do We Do Examination?Jewana J. GhazalNo ratings yet
- Primary ImpressionDocument17 pagesPrimary ImpressionJewana J. GhazalNo ratings yet
- Lecture 9 & 10 - Cements (Slides)Document52 pagesLecture 9 & 10 - Cements (Slides)JustDen09No ratings yet
- Lenze ESMD 230VDocument23 pagesLenze ESMD 230VNenad MarticNo ratings yet
- Experiment 3Document5 pagesExperiment 3Viky KumarNo ratings yet
- Microbiology PosterDocument1 pageMicrobiology PosterAgnieszkaNo ratings yet
- Introduction To Excel For DATA ANALYSTS Day-01Document8 pagesIntroduction To Excel For DATA ANALYSTS Day-01ErrY Florencia100% (1)
- ChemEngineering 04 00063 v2Document22 pagesChemEngineering 04 00063 v2Akademski TrudoviNo ratings yet
- Mounting Instruction Series 70+70D+70M - 9420022100Document8 pagesMounting Instruction Series 70+70D+70M - 9420022100Bob ToddNo ratings yet
- Black Smithy ShopDocument3 pagesBlack Smithy ShopAmarjeet Singh (Assistant Professor- Mechanical Engineer)No ratings yet
- Assignment#3: DR - Azhar UL HaqDocument9 pagesAssignment#3: DR - Azhar UL HaqmuzammalNo ratings yet
- Design of Missile Control System Using Model Predictive ControlDocument7 pagesDesign of Missile Control System Using Model Predictive ControlNorah M KiggunduNo ratings yet
- Gen Chem Revision 2013 PDFDocument2 pagesGen Chem Revision 2013 PDFPSCNo ratings yet
- Distress ID ManualDocument30 pagesDistress ID Manualramdasse100% (2)
- Introduction To The Program FULLPROF Refinement ofDocument15 pagesIntroduction To The Program FULLPROF Refinement ofehagar60No ratings yet
- Power RICH SystemBrochureRev3Document4 pagesPower RICH SystemBrochureRev3Jeremy HensleyNo ratings yet
- Ce 1304 Environmental EngineeringDocument44 pagesCe 1304 Environmental EngineeringprashmceNo ratings yet
- CHAPTER 4: Antenna Array and SynthesisDocument15 pagesCHAPTER 4: Antenna Array and SynthesisTibebu Xibe TeNo ratings yet
- Whole PDFDocument191 pagesWhole PDFMYNAMENo ratings yet
- Baby Booties Pattern Uni - Boots by Vineraeyerpatterns: Skill Level - AdvansedDocument11 pagesBaby Booties Pattern Uni - Boots by Vineraeyerpatterns: Skill Level - AdvansedMariana Anchepe100% (2)
- Earthing MaterialsDocument2 pagesEarthing MaterialsMohammed MustafaNo ratings yet
- Grade 2 Tos 3RD Quarter CompleteDocument15 pagesGrade 2 Tos 3RD Quarter CompleteLyka TamarayNo ratings yet
- Real-Time Construction Project ProgressDocument217 pagesReal-Time Construction Project Progressbala pandiyanNo ratings yet
- Item ConversionDocument52 pagesItem Conversionredro0% (1)
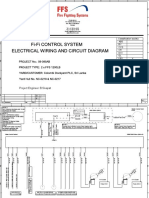
- Electrical Wiring and Circuit Diagram Fi-Fi Control SystemDocument16 pagesElectrical Wiring and Circuit Diagram Fi-Fi Control SystemDamithaNo ratings yet
- ACL 395 Resistivity Meter: Operation ManualDocument13 pagesACL 395 Resistivity Meter: Operation Manualrhap_0925060No ratings yet
- Solution of Transportation Problem With South-EastDocument12 pagesSolution of Transportation Problem With South-EastS AdilakshmiNo ratings yet
- Ship Resistance OP ShahDocument85 pagesShip Resistance OP ShahlakshmiNo ratings yet
- Simple Annuity 1Document13 pagesSimple Annuity 1Kelvin BarceLon0% (1)
- The Design of High-Performance Analog Circuits On Digital CMOS Chips - Vittoz - PaperDocument155 pagesThe Design of High-Performance Analog Circuits On Digital CMOS Chips - Vittoz - Papercira529No ratings yet