Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5820)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Best of Five MCQs For The Rheumatology SCEDocument225 pagesBest of Five MCQs For The Rheumatology SCElittle lulu100% (2)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Ultherapy Patient BrochureDocument2 pagesUltherapy Patient BrochureSusantiNo ratings yet
- The Lifestyle of A VegetarianDocument2 pagesThe Lifestyle of A VegetarianCarlos DNo ratings yet
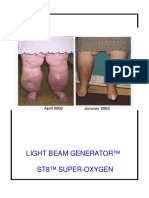
- Wow Light Beam Generator St8 Super-OxygenDocument44 pagesWow Light Beam Generator St8 Super-OxygenMilan Valachovic100% (1)
- Early Warning SignsDocument1 pageEarly Warning SignsRosarioBengocheaSecoNo ratings yet
- Maintenance Guide PDFDocument2 pagesMaintenance Guide PDFRosarioBengocheaSecoNo ratings yet
- ConnectednessDocument13 pagesConnectednessRosarioBengocheaSeco100% (1)
- ConnectednessDocument13 pagesConnectednessRosarioBengocheaSeco100% (1)
- Vaskin 2009Document3 pagesVaskin 2009RosarioBengocheaSecoNo ratings yet
- Activities For Assessing and Developing ReadinessDocument17 pagesActivities For Assessing and Developing ReadinessRosarioBengocheaSecoNo ratings yet
- Psychiatry Research: Philip Brittain, Dominic H. Ffytche, Allison Mckendrick, Simon SurguladzeDocument6 pagesPsychiatry Research: Philip Brittain, Dominic H. Ffytche, Allison Mckendrick, Simon SurguladzeRosarioBengocheaSecoNo ratings yet
- Bell 2010Document8 pagesBell 2010RosarioBengocheaSecoNo ratings yet
- Ziv 2011Document2 pagesZiv 2011RosarioBengocheaSecoNo ratings yet
- Social Perception and Social Skill in SchizophreniaDocument12 pagesSocial Perception and Social Skill in SchizophreniaRosarioBengocheaSecoNo ratings yet
- Couture 2006Document20 pagesCouture 2006RosarioBengocheaSecoNo ratings yet
- Roberts 2009Document7 pagesRoberts 2009RosarioBengocheaSecoNo ratings yet
- Social Cognition in Schizophrenia, Part 2: 12-Month Stability and Prediction of Functional Outcome in First-Episode PatientsDocument8 pagesSocial Cognition in Schizophrenia, Part 2: 12-Month Stability and Prediction of Functional Outcome in First-Episode PatientsRosarioBengocheaSecoNo ratings yet
- Antenatal AssessmentDocument53 pagesAntenatal AssessmentAaron Wallace100% (1)
- Tacrolimus Ointment Is Used To Treat The Symptoms of EczemaDocument2 pagesTacrolimus Ointment Is Used To Treat The Symptoms of EczemaSharan SahotaNo ratings yet
- Child Abuse and Neglect PDF 75545669305285Document24 pagesChild Abuse and Neglect PDF 75545669305285JOSÉ DAVID SALCEDO CASTRONo ratings yet
- STAFFING-POWER ReivisedPOINTDocument103 pagesSTAFFING-POWER ReivisedPOINTEkoy TheRealNo ratings yet
- Main PPT For Fitness Grade & 10Document25 pagesMain PPT For Fitness Grade & 10Vinod Baitha (Vinod Sir)No ratings yet
- Defining NursingDocument28 pagesDefining NursingSao Tome100% (1)
- Dating Violence ThesisDocument4 pagesDating Violence Thesisafjrqokne100% (2)
- IAAP Body of KnowledgeDocument108 pagesIAAP Body of Knowledge9c296h7my6No ratings yet
- Childhood Obesity - Prevention & InterventionDocument51 pagesChildhood Obesity - Prevention & InterventionDea Mustika Hapsari100% (1)
- Fall Risk AssessmentDocument14 pagesFall Risk AssessmentLa navida Mv100% (1)
- Module # 3 Physiological Changes in Aging Affecting Various SystemsDocument30 pagesModule # 3 Physiological Changes in Aging Affecting Various SystemsJann ericka JaoNo ratings yet
- Announcement PKBDocument8 pagesAnnouncement PKBlo tek huiNo ratings yet
- CWU Psy 3Document8 pagesCWU Psy 3Codillia CheongNo ratings yet
- Global Issues Data Response Questions AdviceDocument9 pagesGlobal Issues Data Response Questions Adviceapi-261914272No ratings yet
- Alpha 1 AT DefficiencyDocument22 pagesAlpha 1 AT DefficiencySensing NonsenseNo ratings yet
- Ped001 - Lesson 1Document12 pagesPed001 - Lesson 1JERE-ANN MANAMBAYNo ratings yet
- Multilingual GPsDocument26 pagesMultilingual GPsMax RamirezNo ratings yet
- CBC Bread and Pastry Production SfistDocument84 pagesCBC Bread and Pastry Production SfistNel Mar100% (7)
- ch04 - States of Conciousness - Quiz 1Document4 pagesch04 - States of Conciousness - Quiz 1api-351675451No ratings yet
- Types of Cerebral PalsyDocument6 pagesTypes of Cerebral PalsySahil SahniNo ratings yet
- Chest X-Ray Findings and Temporal Lung Changes in Patients With COVID-19 PneumoniaDocument9 pagesChest X-Ray Findings and Temporal Lung Changes in Patients With COVID-19 PneumoniaRaniNo ratings yet
- Using Gratitude To Promote Positive Change A Series of Meta Analyses Investigating The Effectiveness of Gratitude InterventionsDocument17 pagesUsing Gratitude To Promote Positive Change A Series of Meta Analyses Investigating The Effectiveness of Gratitude InterventionsArina CismaruNo ratings yet
- Biology Investigatory Project: Drug and Alcohol AbuseDocument19 pagesBiology Investigatory Project: Drug and Alcohol AbuseChomu Dj100% (1)
- Diabetes NCPDocument6 pagesDiabetes NCPMonique Sacherow BacherNo ratings yet
- Pancreatitis Cronica Dog-CatDocument14 pagesPancreatitis Cronica Dog-CatSamantha Orozco PinedaNo ratings yet
- OtodexDocument2 pagesOtodexadelin ransunNo ratings yet