Download as pdf or txt
You might also like
- How To Measure Frailty in Your PatientsDocument1 pageHow To Measure Frailty in Your PatientsZahra'a Al-AhmedNo ratings yet
- Abdominal Examination: OSCE ChecklistDocument2 pagesAbdominal Examination: OSCE ChecklistWafa Abdalla100% (2)
- Molecules 22 00058Document41 pagesMolecules 22 00058Jordan MillerNo ratings yet
- Aprox Intersectorial EtdDocument7 pagesAprox Intersectorial EtdLuis AlfonsoNo ratings yet
- Neglected Infectious Disease in The Perspective of GlobalDocument18 pagesNeglected Infectious Disease in The Perspective of GlobalHany Aboelhamd AbdelgafarNo ratings yet
- Aids 2013Document404 pagesAids 2013kovaron80No ratings yet
- Review Article: Chagas' Disease: Pregnancy and Congenital TransmissionDocument11 pagesReview Article: Chagas' Disease: Pregnancy and Congenital Transmissiondiaa skamNo ratings yet
- Contemporary PRJCT-WPS OfficeDocument13 pagesContemporary PRJCT-WPS Officecram eugnapenNo ratings yet
- Aids 2012Document388 pagesAids 2012Xadvier Rivera JimenezNo ratings yet
- Pertemuan 15 - Epidemiologi Penyakit New Emerging DiseaseDocument79 pagesPertemuan 15 - Epidemiologi Penyakit New Emerging DiseasePutti AnnisaNo ratings yet
- At The End of The Lesson, The Students Will:: Overview of Public Health Nursing in The Philippines Learning OutcomesDocument18 pagesAt The End of The Lesson, The Students Will:: Overview of Public Health Nursing in The Philippines Learning OutcomesPABLO, JACKSON P.100% (1)
- Textbook of AIDS Pathology, Edward C. Klatt, MD (May 2, 2011)Document382 pagesTextbook of AIDS Pathology, Edward C. Klatt, MD (May 2, 2011)Marc Imhotep Cray, M.D.No ratings yet
- Disease 4Document20 pagesDisease 4KIGHERANo ratings yet
- Epidemiology Public Health Measures For The Control of DiseaseDocument3 pagesEpidemiology Public Health Measures For The Control of Disease339 Humera ShaikhNo ratings yet
- Preventing Pandemics Aug 2021Document44 pagesPreventing Pandemics Aug 2021Victor CorreaNo ratings yet
- Othman 2014Document44 pagesOthman 2014Jessica QuevedoNo ratings yet
- Final Honors Bio PaperDocument10 pagesFinal Honors Bio Paperapi-247377745No ratings yet
- CHN 1 FullDocument88 pagesCHN 1 FullKristine Joy CamusNo ratings yet
- Health RisksDocument21 pagesHealth RisksOxfamNo ratings yet
- Health RisksDocument21 pagesHealth RisksOxfamNo ratings yet
- Health RisksDocument21 pagesHealth RisksOxfamNo ratings yet
- Health RisksDocument21 pagesHealth RisksOxfamNo ratings yet
- Health RisksDocument21 pagesHealth RisksOxfamNo ratings yet
- Health RisksDocument21 pagesHealth RisksOxfamNo ratings yet
- Health RisksDocument21 pagesHealth RisksOxfamNo ratings yet
- Health RisksDocument21 pagesHealth RisksOxfamNo ratings yet
- Health RisksDocument21 pagesHealth RisksOxfamNo ratings yet
- Health RisksDocument21 pagesHealth RisksOxfamNo ratings yet
- Health RisksDocument21 pagesHealth RisksOxfamNo ratings yet
- Health RisksDocument21 pagesHealth RisksOxfamNo ratings yet
- Health RisksDocument21 pagesHealth RisksOxfamNo ratings yet
- Health RisksDocument21 pagesHealth RisksOxfamNo ratings yet
- Health RisksDocument21 pagesHealth RisksOxfamNo ratings yet
- Health RisksDocument21 pagesHealth RisksOxfamNo ratings yet
- Health RisksDocument21 pagesHealth RisksOxfamNo ratings yet
- Health RisksDocument21 pagesHealth RisksOxfamNo ratings yet
- Health RisksDocument21 pagesHealth RisksOxfamNo ratings yet
- Health RisksDocument21 pagesHealth RisksOxfamNo ratings yet
- Health RisksDocument21 pagesHealth RisksOxfamNo ratings yet
- Health RisksDocument21 pagesHealth RisksOxfamNo ratings yet
- Health RisksDocument21 pagesHealth RisksOxfamNo ratings yet
- Health RisksDocument21 pagesHealth RisksOxfamNo ratings yet
- Health RisksDocument21 pagesHealth RisksOxfamNo ratings yet
- Health RisksDocument21 pagesHealth RisksOxfamNo ratings yet
- Health RisksDocument21 pagesHealth RisksOxfamNo ratings yet
- Health RisksDocument21 pagesHealth RisksOxfamNo ratings yet
- Health RisksDocument21 pagesHealth RisksOxfamNo ratings yet
- Health RisksDocument21 pagesHealth RisksOxfamNo ratings yet
- Health RisksDocument21 pagesHealth RisksOxfamNo ratings yet
- Health RisksDocument21 pagesHealth RisksOxfamNo ratings yet
- Health RisksDocument21 pagesHealth RisksOxfamNo ratings yet
- Health RisksDocument21 pagesHealth RisksOxfamNo ratings yet
- Health RisksDocument21 pagesHealth RisksOxfamNo ratings yet
- Health RisksDocument21 pagesHealth RisksOxfamNo ratings yet
- Health RisksDocument21 pagesHealth RisksOxfamNo ratings yet
- Health RisksDocument21 pagesHealth RisksOxfamNo ratings yet
- Health RisksDocument21 pagesHealth RisksOxfamNo ratings yet
- Health RisksDocument21 pagesHealth RisksOxfamNo ratings yet
- Health RisksDocument21 pagesHealth RisksOxfamNo ratings yet
- Health RisksDocument21 pagesHealth RisksOxfamNo ratings yet
- Health RisksDocument21 pagesHealth RisksOxfamNo ratings yet
- Pcos 170123144542Document86 pagesPcos 170123144542Dewi Puspita Apsari100% (2)
- PKM Toga LandDocument3 pagesPKM Toga LandDewi Puspita ApsariNo ratings yet
- Scanned by CamscannerDocument3 pagesScanned by CamscannerDewi Puspita ApsariNo ratings yet
- Isbn6641-4 EG 19-01Document4 pagesIsbn6641-4 EG 19-01Dewi Puspita ApsariNo ratings yet
- HDFC Life Critical Illness Plus Rider BrochureDocument8 pagesHDFC Life Critical Illness Plus Rider Brochurepinky_y2kNo ratings yet
- Drug StudyDocument6 pagesDrug StudyAko Si Vern ÖNo ratings yet
- (Impetigo) : Erbil Polythecnic University Soran Technical Insititute Nuraing Department First StageDocument14 pages(Impetigo) : Erbil Polythecnic University Soran Technical Insititute Nuraing Department First StageKubra ĖdrisNo ratings yet
- Medication Sheet 2021-2022Document3 pagesMedication Sheet 2021-2022Attekah MohammedNo ratings yet
- Complications of PuerperiumDocument45 pagesComplications of PuerperiumsubashikNo ratings yet
- Appendix 4 - Example Birth HistoryDocument2 pagesAppendix 4 - Example Birth HistorySriMathi Kasi Malini ArmugamNo ratings yet
- Bacterial PathogensDocument16 pagesBacterial Pathogensdevita oktaviani salsabilla kiranaNo ratings yet
- 03 Muscle and Neuromuscular Junction Disorders PDFDocument325 pages03 Muscle and Neuromuscular Junction Disorders PDFOTTO JESUS VEGA VEGA100% (2)
- Lifestyle Modification: Asterlyn T. Coniendo Bsn-IvDocument4 pagesLifestyle Modification: Asterlyn T. Coniendo Bsn-IvAsterlyn ConiendoNo ratings yet
- 1.who Shall Be Considered As Having Community-Acquired Pneumonia?Document6 pages1.who Shall Be Considered As Having Community-Acquired Pneumonia?Kristine Jade OdtujanNo ratings yet
- Brochure Ultrasonograph y of The Live Ru 42 eDocument132 pagesBrochure Ultrasonograph y of The Live Ru 42 ealiceinwinterNo ratings yet
- Written Assignment Unit 3Document5 pagesWritten Assignment Unit 3Benses AlvaradoNo ratings yet
- Feline Nonregenerative Anemia Pathophysiology and ErilologiesDocument7 pagesFeline Nonregenerative Anemia Pathophysiology and ErilologiesTORRES GUTIERREZ JOYNY RAQUEL catedraticoNo ratings yet
- Chapter 53: Nursing Management: Sexually Transmitted DiseasesDocument4 pagesChapter 53: Nursing Management: Sexually Transmitted Diseasesjefroc100% (1)
- Chronic Pancreatitis 1Document21 pagesChronic Pancreatitis 1Bala DhanaNo ratings yet
- Blood Transfusion Purpose: 9. Check Blood For Presence of BubblesDocument2 pagesBlood Transfusion Purpose: 9. Check Blood For Presence of BubblesMabes100% (1)
- Noncirrhotic Portal Hypertension: ReviewDocument6 pagesNoncirrhotic Portal Hypertension: ReviewIsrael BlancoNo ratings yet
- Dysentery ShigellaDocument10 pagesDysentery ShigellaPaulNo ratings yet
- Concept Map Safe Quality Ebp CareDocument2 pagesConcept Map Safe Quality Ebp Careapi-307852462No ratings yet
- Guidelines For Gamma Irradiation of Blood Components: A ZSBT NDocument8 pagesGuidelines For Gamma Irradiation of Blood Components: A ZSBT NDiego Martin RabasedasNo ratings yet
- Nipah Virus PDFDocument2 pagesNipah Virus PDFRakesh SahuNo ratings yet
- Endotracheal Tube SuctioningDocument5 pagesEndotracheal Tube SuctioningArlene DalisayNo ratings yet
- Health: Ielts Thematic VocabDocument3 pagesHealth: Ielts Thematic VocabNguyễn Bông Phương ThảoNo ratings yet
- Case Presentation OralcavityDocument33 pagesCase Presentation Oralcavityapi-250609678No ratings yet
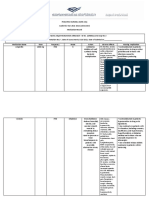
- Assessment Nursing Diagnosis Patient Outcomes Interventions Rationale Evaluation of OutcomesDocument2 pagesAssessment Nursing Diagnosis Patient Outcomes Interventions Rationale Evaluation of OutcomeslitaNo ratings yet
- Surgical Complication of Typhoid FeverDocument10 pagesSurgical Complication of Typhoid FeverHelsa Eldatarina JNo ratings yet
- First Aid PPT - DR GhaziDocument22 pagesFirst Aid PPT - DR GhaziMands_KLP100% (1)
- 5 Myths About STDsDocument8 pages5 Myths About STDsThanh Bình ĐinhNo ratings yet