Download as pdf or txt
You might also like
- Research Proposal On Prevalence of PneumoniaDocument26 pagesResearch Proposal On Prevalence of Pneumoniasolomon demissew62% (13)
- Case Study Hpi SamplesDocument10 pagesCase Study Hpi SamplesMihai DohotariuNo ratings yet
- Thimerosal Content of US Vaccines 02-04Document3 pagesThimerosal Content of US Vaccines 02-04Diane StierNo ratings yet
- Cervical Cancer Research 1Document9 pagesCervical Cancer Research 1tivaNo ratings yet
- Cervical Cancer MalaysiaDocument12 pagesCervical Cancer MalaysiaAlbina Mary RajooNo ratings yet
- Knowledge and Perception of Female Nursing Students About Human Papilloma Virus (HPV), Cervical Cancer and Attitudes Towards HPV VaccinationDocument18 pagesKnowledge and Perception of Female Nursing Students About Human Papilloma Virus (HPV), Cervical Cancer and Attitudes Towards HPV VaccinationpangaribuansantaNo ratings yet
- Immunization of Cervical CancerDocument14 pagesImmunization of Cervical CancerAasif KohliNo ratings yet
- WA0054mmmDocument4 pagesWA0054mmmA HNo ratings yet
- Mini CaseDocument4 pagesMini CaseSheryl Anne GonzagaNo ratings yet
- Conduct Organized Campaign On Cervical Cancer ScreDocument3 pagesConduct Organized Campaign On Cervical Cancer Scregivelyn olorvidaNo ratings yet
- Felix Mpachika - CHAPTER 1Document8 pagesFelix Mpachika - CHAPTER 1sekani mondwechilengaNo ratings yet
- Intl J Gynecology Obste - 2021 - WilailakDocument5 pagesIntl J Gynecology Obste - 2021 - WilailakKalaivathanan VathananNo ratings yet
- Case Study of Cervical Cancer Stage III (Final)Document82 pagesCase Study of Cervical Cancer Stage III (Final)DRJC94% (33)
- A Synthesis Paper About Breast, Testicular and Cervical Cancer in The PhillipinesDocument3 pagesA Synthesis Paper About Breast, Testicular and Cervical Cancer in The Phillipinesjanna mae patriarcaNo ratings yet
- Cancer CervixDocument7 pagesCancer Cervixkalpana gondipalliNo ratings yet
- Epidemiological Profile of Gynecologic Breast Cancer inDocument3 pagesEpidemiological Profile of Gynecologic Breast Cancer indomi kalondaNo ratings yet
- Cervical CA Proposal Jan152010Document21 pagesCervical CA Proposal Jan152010redblade_88100% (2)
- Cervical Ca R. ProposalDocument7 pagesCervical Ca R. ProposalRobel HaftomNo ratings yet
- Keywords: Human Papillomavirus Vaccine, Efficacy, Safety, Phase III Randomized TrialsDocument10 pagesKeywords: Human Papillomavirus Vaccine, Efficacy, Safety, Phase III Randomized TrialsBassment MixshowNo ratings yet
- Meeting The Challenges of Breast Cancer 290411Document40 pagesMeeting The Challenges of Breast Cancer 290411Presentaciones_FKNo ratings yet
- Neenu BabyDocument24 pagesNeenu BabyNeenu PauloseNo ratings yet
- Chapter 1 of Research Study PDFDocument3 pagesChapter 1 of Research Study PDFAasif KohliNo ratings yet
- Current Status of Knowledge, Attitude and Practice (KAP) and Screening For Cervical Cancer in Countries at Different Levels of DevelopmentDocument7 pagesCurrent Status of Knowledge, Attitude and Practice (KAP) and Screening For Cervical Cancer in Countries at Different Levels of DevelopmentHuzaifa SaeedNo ratings yet
- Cervical Cancer Main WorkDocument41 pagesCervical Cancer Main WorkocmainNo ratings yet
- Cervical CancerDocument75 pagesCervical CancerJetty Elizabeth JoseNo ratings yet
- E Lert OT LarmedDocument48 pagesE Lert OT LarmedJetty Elizabeth JoseNo ratings yet
- E Lert OT LarmedDocument58 pagesE Lert OT LarmedJetty Elizabeth JoseNo ratings yet
- E Lert OT LarmedDocument46 pagesE Lert OT LarmedJetty Elizabeth JoseNo ratings yet
- E Lert OT LarmedDocument47 pagesE Lert OT LarmedJetty Elizabeth JoseNo ratings yet
- E Lert OT LarmedDocument54 pagesE Lert OT LarmedJetty Elizabeth JoseNo ratings yet
- International Journal of Scientific Research: OncologyDocument3 pagesInternational Journal of Scientific Research: OncologyDr SrigopalNo ratings yet
- Asia Oceania GuidelinesDocument25 pagesAsia Oceania GuidelinesKaily TrầnNo ratings yet
- A Review On Cervical Cancer VaccinationDocument3 pagesA Review On Cervical Cancer VaccinationKIU PUBLICATION AND EXTENSIONNo ratings yet
- Pamj 22 26Document8 pagesPamj 22 26Yosie Yulanda PutraNo ratings yet
- Trends and Determinants of Maternal Mortality in Mizan-Tepi University Teaching and Bonga General Hospital From 2011 - 2015: A Case Control StudyDocument8 pagesTrends and Determinants of Maternal Mortality in Mizan-Tepi University Teaching and Bonga General Hospital From 2011 - 2015: A Case Control StudyTegenne LegesseNo ratings yet
- Cervical Cancer FACTSHEET April 2011Document3 pagesCervical Cancer FACTSHEET April 2011Daomisyel LiaoNo ratings yet
- Current Global Status & Impact of Human Papillomavirus Vaccination: Implications For IndiaDocument12 pagesCurrent Global Status & Impact of Human Papillomavirus Vaccination: Implications For IndiaPrasanna BabuNo ratings yet
- Epidemiological Study On Breast Cancer Associated Risk Factors and Screening Practices Among Women in Mbaise Imo State, NigeriaDocument8 pagesEpidemiological Study On Breast Cancer Associated Risk Factors and Screening Practices Among Women in Mbaise Imo State, NigeriaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Practice Bulletin: Endometrial CancerDocument21 pagesPractice Bulletin: Endometrial CancerDivika ShilvanaNo ratings yet
- 1 s2.0 S2352578919300554 MainDocument8 pages1 s2.0 S2352578919300554 Mainkarenelijah147No ratings yet
- FIGO CANCER REPORT 2021 - Cancer of The Cervix Uteri 2021 Update 2021Document17 pagesFIGO CANCER REPORT 2021 - Cancer of The Cervix Uteri 2021 Update 2021amrodriguez9No ratings yet
- Ca ServixDocument30 pagesCa ServixDanang MustofaNo ratings yet
- CANCER Preventing Cervical CancerDocument4 pagesCANCER Preventing Cervical CancerLeonardo Rodríguez BottacciNo ratings yet
- Manuskrip PI169418064519870645Document19 pagesManuskrip PI169418064519870645Bibup GhaziyahNo ratings yet
- Genotypes and Associated Risk Levels of Human Papilloma Virus Among Female Patients Attending Rabuor Sub County Hospital, KisumuDocument13 pagesGenotypes and Associated Risk Levels of Human Papilloma Virus Among Female Patients Attending Rabuor Sub County Hospital, KisumuMJBAS JournalNo ratings yet
- Tatalaksana Dan Pencegahan - Hal 29-38 - Cancer of The Cervix Uteri 2021 UpdateDocument17 pagesTatalaksana Dan Pencegahan - Hal 29-38 - Cancer of The Cervix Uteri 2021 UpdateAl-Amirah ZainabNo ratings yet
- Only One in Five Indonesian Women Are Aware of Cervical Cancer ScreeningDocument3 pagesOnly One in Five Indonesian Women Are Aware of Cervical Cancer Screeningedi_wsNo ratings yet
- Update of Breast Cancer Profile in IndonesiaDocument7 pagesUpdate of Breast Cancer Profile in IndonesiaYona TarunaNo ratings yet
- Knowledge, Attitude and Uptake of Cervical Cancer Screening Among HIV Positive Women Visiting Kampala International University Teaching HospitalDocument10 pagesKnowledge, Attitude and Uptake of Cervical Cancer Screening Among HIV Positive Women Visiting Kampala International University Teaching HospitalKIU PUBLICATION AND EXTENSIONNo ratings yet
- FIGO 2018 - Cervical CADocument15 pagesFIGO 2018 - Cervical CAJP RecioNo ratings yet
- Malaria in Pregnancy - A Community-Based Study On The Knowledge, Perception, andDocument15 pagesMalaria in Pregnancy - A Community-Based Study On The Knowledge, Perception, andsemabiaabenaNo ratings yet
- Assignment No 1 bt502 SeminarDocument15 pagesAssignment No 1 bt502 SeminarMashal WakeelaNo ratings yet
- Figo 2018Document15 pagesFigo 2018EJ CMNo ratings yet
- Prospects and Potential For Expanding Women's Oncofertility Options - Gabriella TranDocument18 pagesProspects and Potential For Expanding Women's Oncofertility Options - Gabriella TrannurjNo ratings yet
- Iva Screening2Document9 pagesIva Screening2ponekNo ratings yet
- Tesfaw, Alebachew, Tiruneh - 2020 - Why Women With Breast Cancer Presented Late To Health Care Facility in North-West Ethiopia A QualitaDocument15 pagesTesfaw, Alebachew, Tiruneh - 2020 - Why Women With Breast Cancer Presented Late To Health Care Facility in North-West Ethiopia A QualitaABDUL MUHAIMINNo ratings yet
- Health Belief Model On The Determinants of Human Papilloma Virus Vaccination in Women of Reproductive Age in Surakarta, Central JavaDocument11 pagesHealth Belief Model On The Determinants of Human Papilloma Virus Vaccination in Women of Reproductive Age in Surakarta, Central Javaadilla kusumaNo ratings yet
- Breast Cancer Awareness Among Pregnant Women at Hoima Regional Referral Hospital, Western UgandaDocument12 pagesBreast Cancer Awareness Among Pregnant Women at Hoima Regional Referral Hospital, Western UgandaKIU PUBLICATION AND EXTENSIONNo ratings yet
- New Microsoft Office Word DocumentDocument11 pagesNew Microsoft Office Word DocumentMihaela AndreiNo ratings yet
- Rajiv Gandhi University of Health Sciences, Karnataka, Bangalore Annexure - Ii Name of The Candidate and Address (In Block Letters)Document18 pagesRajiv Gandhi University of Health Sciences, Karnataka, Bangalore Annexure - Ii Name of The Candidate and Address (In Block Letters)subiNo ratings yet
- Sexuallytransmittedhuman Papillomavirus: Update in Epidemiology, Prevention, and ManagementDocument22 pagesSexuallytransmittedhuman Papillomavirus: Update in Epidemiology, Prevention, and Managementerikglu2796No ratings yet
- Breast Cancer in Nigeria: Diagnosis, Management and ChallengesFrom EverandBreast Cancer in Nigeria: Diagnosis, Management and ChallengesNo ratings yet
- Kanker ServiksDocument308 pagesKanker ServiksponekNo ratings yet
- Sadiq KhanDocument5 pagesSadiq KhanponekNo ratings yet
- Checklist Dmpa EnglishDocument3 pagesChecklist Dmpa EnglishponekNo ratings yet
- Scientific Schedule: Alarm Course Day 1Document11 pagesScientific Schedule: Alarm Course Day 1ponekNo ratings yet
- Preclinical Condition MagementDocument27 pagesPreclinical Condition MagementponekNo ratings yet
- Analisis Pengendalian Alkes Farmasi Di Rs Pangkal PinangDocument12 pagesAnalisis Pengendalian Alkes Farmasi Di Rs Pangkal PinangponekNo ratings yet
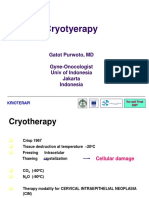
- CRYOTERAPI See&Treat GatotDocument20 pagesCRYOTERAPI See&Treat GatotponekNo ratings yet
- CHN & CD Pre-Board TestDocument6 pagesCHN & CD Pre-Board TestAndrea Broccoli100% (1)
- Health Check Consent FormDocument4 pagesHealth Check Consent Formaxenic04No ratings yet
- Health For All-ImpDocument54 pagesHealth For All-ImpSathish KumarNo ratings yet
- Polio Eradication: Pulse Polio Programme: A.Prabhakaran M.SC (N), Tutor, VMACON, SalemDocument13 pagesPolio Eradication: Pulse Polio Programme: A.Prabhakaran M.SC (N), Tutor, VMACON, SalemPrabhakaran Aranganathan100% (3)
- Indian Immunization Programme: A Literature Review 2012Document44 pagesIndian Immunization Programme: A Literature Review 2012Raajan K SharmaNo ratings yet
- Nanotechnology and VaccinesDocument24 pagesNanotechnology and VaccinespranchishNo ratings yet
- Multifibren UDocument6 pagesMultifibren UMari Fere100% (1)
- Diphtheria HandoutsDocument8 pagesDiphtheria HandoutsRachelle Mae DimayugaNo ratings yet
- Landasan Teori Tetanus GeneralisataDocument22 pagesLandasan Teori Tetanus GeneralisataadityaNo ratings yet
- Fake Vaccines in June 2016Document1 pageFake Vaccines in June 2016Herlinda SoefiyantiNo ratings yet
- Most Common MedsDocument13 pagesMost Common MedsMaria Zenaida BonoanNo ratings yet
- Science & Health Writing (English, Sample) Dengue Kills TitleDocument2 pagesScience & Health Writing (English, Sample) Dengue Kills TitleValyn Encarnacion100% (1)
- Whooping Cough Letter Shahala Middle SchoolDocument2 pagesWhooping Cough Letter Shahala Middle SchoolKGW NewsNo ratings yet
- "Expanded Program On Immunization": Angeles University FoundationDocument12 pages"Expanded Program On Immunization": Angeles University FoundationJaillah Reigne CuraNo ratings yet
- Sample CDC Whistleblower Letter For RepublicansDocument3 pagesSample CDC Whistleblower Letter For RepublicansmarathonjonNo ratings yet
- Rabies Prevention and ControlDocument9 pagesRabies Prevention and ControlJames RiedNo ratings yet
- Baby Vaccination ProgramDocument1 pageBaby Vaccination Programplainspeak100% (1)
- Battisti Exercices PediatrieDocument197 pagesBattisti Exercices Pediatrieahkrab100% (1)
- Barangay Mantuyong Bherts (Inventory of 1 Dose For Covid-19 Vaccination)Document1 pageBarangay Mantuyong Bherts (Inventory of 1 Dose For Covid-19 Vaccination)Barangay CentroNo ratings yet
- Quiz Hand SlidesDocument10 pagesQuiz Hand SlidesSushant SaxenaNo ratings yet
- Chappuis, Neonatal Immunity and Immunisation in Early Age. Lesons From Veterinary MedicineDocument5 pagesChappuis, Neonatal Immunity and Immunisation in Early Age. Lesons From Veterinary MedicineNath BixoNo ratings yet
- Acs Ca3 BookDocument69 pagesAcs Ca3 BookchrisNo ratings yet
- Strachan Hygiene HypotheseDocument9 pagesStrachan Hygiene HypotheseRikko HudyonoNo ratings yet
- Pamphlet Jan 8 PDFDocument2 pagesPamphlet Jan 8 PDFRouetchen AshleeNo ratings yet
- Fever in Infants and Children: Health NotesDocument3 pagesFever in Infants and Children: Health NotesHanso LataNo ratings yet
- Hubungan Antara Faktor Gender Dan Usia Terhadap Efektivitas Vaksinasi Hepatitis B Pada Mahasiswa Jurusan Keperawatan Di Poltekkes SurakartaDocument4 pagesHubungan Antara Faktor Gender Dan Usia Terhadap Efektivitas Vaksinasi Hepatitis B Pada Mahasiswa Jurusan Keperawatan Di Poltekkes SurakartaadindadpyanaNo ratings yet
- Moving Target Vaccines Thimerosol and AutismDocument25 pagesMoving Target Vaccines Thimerosol and AutismcirclestretchNo ratings yet