Download as pdf or txt
You might also like
- Grand Osce ReviewerDocument16 pagesGrand Osce ReviewerBA Ong100% (1)
- Clinical Practice Guidelines For The Obstetrician - GynecologistDocument79 pagesClinical Practice Guidelines For The Obstetrician - GynecologistAngela Caguitla67% (3)
- Classification and Diagnosis of Endometrial HyperplasiaDocument7 pagesClassification and Diagnosis of Endometrial HyperplasiaaksinuNo ratings yet
- qt5j15k0nf NosplashDocument2 pagesqt5j15k0nf NosplashsinayaphetNo ratings yet
- Parkhurst 2013Document17 pagesParkhurst 2013barkat cikomNo ratings yet
- Effective Screening14Document9 pagesEffective Screening14ponekNo ratings yet
- Best Practice & Research Clinical Obstetrics and GynaecologyDocument12 pagesBest Practice & Research Clinical Obstetrics and GynaecologyAndhika MaulinaNo ratings yet
- The Effect of Medical Experience On The Economic Evaluation of Health Policies. A Discrete Choice ExperimentDocument13 pagesThe Effect of Medical Experience On The Economic Evaluation of Health Policies. A Discrete Choice ExperimentGuillermo Sanchez VanegasNo ratings yet
- Literature Review On Cervical Cancer ScreeningDocument4 pagesLiterature Review On Cervical Cancer Screeningbqvlqjugf100% (1)
- 1 Health Econ Rodriguez 2013Document7 pages1 Health Econ Rodriguez 2013EgociNo ratings yet
- Accounting For Future Costs in Medical Cost-Effectiveness AnalysisDocument32 pagesAccounting For Future Costs in Medical Cost-Effectiveness AnalysisYossRlingNo ratings yet
- Prevention and Health Education How Recent Advances in TheDocument4 pagesPrevention and Health Education How Recent Advances in TheNataLya MendilaNo ratings yet
- Future ImplicationsDocument2 pagesFuture ImplicationsConsuelo MolinaNo ratings yet
- Art:10 1186/bcr1744Document23 pagesArt:10 1186/bcr1744Preda LoredanaNo ratings yet
- Prevention of Gastric CancerDocument2 pagesPrevention of Gastric CancerAndhika Bintang MahardhikaNo ratings yet
- Proposal First Draft 07.02.2019.edited - EditedDocument12 pagesProposal First Draft 07.02.2019.edited - EditedHammoda Abu-odahNo ratings yet
- Breast Cancer Policy in Latin America Account of ADocument12 pagesBreast Cancer Policy in Latin America Account of Aandrea sanabria pedrazaNo ratings yet
- Ovarian Cancer DissertationDocument5 pagesOvarian Cancer DissertationHelpWritingPaperYonkers100% (1)
- Breast CancerDocument25 pagesBreast CancerEthio PNo ratings yet
- HS 4810 DF Unit 2Document5 pagesHS 4810 DF Unit 2Mathias NjoyaNo ratings yet
- Breast Cancer ReflectionDocument4 pagesBreast Cancer ReflectionCAJES NOLINo ratings yet
- iDSI Reference CaseDocument8 pagesiDSI Reference CaseZurNo ratings yet
- Dissertation Funding Public HealthDocument5 pagesDissertation Funding Public HealthWriteMyPaperCanadaUK100% (1)
- Jurnal Cbe 1Document21 pagesJurnal Cbe 1Dewi SurayaNo ratings yet
- Proposal First Draft 03.02.2019Document35 pagesProposal First Draft 03.02.2019Hammoda Abu-odah100% (1)
- Breast CancerDocument23 pagesBreast CancerCiocan AlexandraNo ratings yet
- MIT CV Booklet 11 4 2010Document67 pagesMIT CV Booklet 11 4 2010XesemeNo ratings yet
- Systematic Review of Peer-Reviewed Literature On Global Condom Promotion ProgramsDocument21 pagesSystematic Review of Peer-Reviewed Literature On Global Condom Promotion ProgramsAbhishek DalalNo ratings yet
- A Systematic Review of Patient Education Strategies For Oncology Patients in Low-And Middle-Income CountriesDocument10 pagesA Systematic Review of Patient Education Strategies For Oncology Patients in Low-And Middle-Income CountriesAhana MukherjeeNo ratings yet
- Breast and Gynecological Cancers - An Integrated Approach For Screening and Early Diagnosis in Developing Countries (PDFDrive)Document365 pagesBreast and Gynecological Cancers - An Integrated Approach For Screening and Early Diagnosis in Developing Countries (PDFDrive)Bharti Pant Gahtori100% (1)
- Dissertation Clinical TrialsDocument5 pagesDissertation Clinical TrialsCanSomeoneWriteMyPaperForMeSingapore100% (1)
- Literature Review Sample On Breast CancerDocument6 pagesLiterature Review Sample On Breast Canceraflslcqrg100% (1)
- NVSM 1613Document7 pagesNVSM 1613kay_mike_83No ratings yet
- Caesarean SectiDocument1 pageCaesarean SectipurityobotNo ratings yet
- Cross Roads in Quality 2008Hlth AffairsDocument11 pagesCross Roads in Quality 2008Hlth AffairsVaida BankauskaiteNo ratings yet
- Cancer Screening in the Developing World: Case Studies and Strategies from the FieldFrom EverandCancer Screening in the Developing World: Case Studies and Strategies from the FieldMadelon L. FinkelNo ratings yet
- ADocument6 pagesANeharika MahajanNo ratings yet
- The Science of Clinical Practice - Disease Diagnosis or Patient Prognosis - Croft Et Al 2015Document8 pagesThe Science of Clinical Practice - Disease Diagnosis or Patient Prognosis - Croft Et Al 2015Bipul RajbhandariNo ratings yet
- Trong bối cảnh phát triển nhanh chóng của các ngành công nghiệp khác nhauDocument9 pagesTrong bối cảnh phát triển nhanh chóng của các ngành công nghiệp khác nhauLinh ĐồngNo ratings yet
- Econometric Evaluation of Health PoliciesDocument41 pagesEconometric Evaluation of Health PoliciescreativejoburgNo ratings yet
- Cancer Screening - Health Impact, Prevalence, Correlates and InterventionsDocument38 pagesCancer Screening - Health Impact, Prevalence, Correlates and InterventionsMary OvbieboNo ratings yet
- Mr. Hariom Rajput Mr. Ramsingh Ji Gmail-ID International Association of Oncology (IAO) Government of IndiaDocument6 pagesMr. Hariom Rajput Mr. Ramsingh Ji Gmail-ID International Association of Oncology (IAO) Government of IndiaHariom RajputNo ratings yet
- 10 1200@jco 2001 19 4 980Document12 pages10 1200@jco 2001 19 4 980Ade Ria Septa UtamiNo ratings yet
- Literature Review of Adverse EventsDocument5 pagesLiterature Review of Adverse Eventsafmabzmoniomdc100% (1)
- A Comparative Analysis of ClassificationDocument12 pagesA Comparative Analysis of ClassificationSharmi BhatNo ratings yet
- PROGRESS1Document11 pagesPROGRESS1Sergio TerrasaNo ratings yet
- Commentary: Improving The Medical Decision-Making Process by John E. WennbergDocument8 pagesCommentary: Improving The Medical Decision-Making Process by John E. WennbergGee ThaNo ratings yet
- CP Driving High Reliability and High ValueDocument12 pagesCP Driving High Reliability and High ValueAkhmad IrawanNo ratings yet
- Primary Care Impact On Health Outcomes A Literature ReviewDocument6 pagesPrimary Care Impact On Health Outcomes A Literature Reviewm1dyhuh1jud2No ratings yet
- Medical Tribune March 2012 MY2Document46 pagesMedical Tribune March 2012 MY2Bernard Ho Kar EngNo ratings yet
- 02 01 Methodologies Realizing Potential Hia 2005Document8 pages02 01 Methodologies Realizing Potential Hia 2005Lidwina Margaretha LakaNo ratings yet
- Jurnal HBMDocument10 pagesJurnal HBMSeindz OstenNo ratings yet
- Dani Rodrik and Mark R. RosenzweigDocument1 pageDani Rodrik and Mark R. RosenzweigEd ZNo ratings yet
- 2019 Sheng BrCa Survivorship Care Beyond TherapyDocument7 pages2019 Sheng BrCa Survivorship Care Beyond TherapyAngélica Fernández PérezNo ratings yet
- Thesis On Health Care FinancingDocument5 pagesThesis On Health Care Financingchristinawestcharleston100% (2)
- Breast Cancer ScreeningDocument13 pagesBreast Cancer ScreeningAinsley PNo ratings yet
- Progress 1Document11 pagesProgress 1dianis0506No ratings yet
- Dissertation Randomised Controlled TrialDocument4 pagesDissertation Randomised Controlled TrialBuyAPaperOnlineUK100% (1)
- An Integrated Machine Learning Scheme For PredictingDocument17 pagesAn Integrated Machine Learning Scheme For PredictingMuzungu Hirwa SylvainNo ratings yet
- Cancer Registries in Four Provinces in Turkey: A Case Study: Research Open AccessDocument8 pagesCancer Registries in Four Provinces in Turkey: A Case Study: Research Open Accessjs14camaraNo ratings yet
- JDS 712Document9 pagesJDS 712aaditya01No ratings yet
- 2014 Article 446Document19 pages2014 Article 446Nimas Ayu Lestari NNo ratings yet
- Kanker ServiksDocument308 pagesKanker ServiksponekNo ratings yet
- Checklist Dmpa EnglishDocument3 pagesChecklist Dmpa EnglishponekNo ratings yet
- Sadiq KhanDocument5 pagesSadiq KhanponekNo ratings yet
- Scientific Schedule: Alarm Course Day 1Document11 pagesScientific Schedule: Alarm Course Day 1ponekNo ratings yet
- Preclinical Condition MagementDocument27 pagesPreclinical Condition MagementponekNo ratings yet
- Analisis Pengendalian Alkes Farmasi Di Rs Pangkal PinangDocument12 pagesAnalisis Pengendalian Alkes Farmasi Di Rs Pangkal PinangponekNo ratings yet
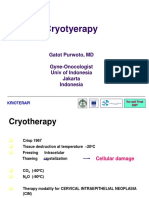
- CRYOTERAPI See&Treat GatotDocument20 pagesCRYOTERAPI See&Treat GatotponekNo ratings yet
- Cervical CancerDocument36 pagesCervical CancerSatish ShresthaNo ratings yet
- Benefits and Contributions Schedule 2021Document72 pagesBenefits and Contributions Schedule 2021MarcoNo ratings yet
- Endometrial HyperplasiaDocument11 pagesEndometrial HyperplasiarinieeeNo ratings yet
- Influencing Elements Impacting The Participation in Cervical Cancer Screening Among Women of Childbearing Age at Jinja Regional Referral Hospital, Eastern UgandaDocument12 pagesInfluencing Elements Impacting The Participation in Cervical Cancer Screening Among Women of Childbearing Age at Jinja Regional Referral Hospital, Eastern UgandaKIU PUBLICATION AND EXTENSIONNo ratings yet
- Luma - Health Insurance Quotation - May Kabyar Oo (3 Options)Document3 pagesLuma - Health Insurance Quotation - May Kabyar Oo (3 Options)Kabyar MayNo ratings yet
- Atlas Cancer CervicalDocument458 pagesAtlas Cancer CervicalihsansabridrNo ratings yet
- Thesis Cervical CancerDocument6 pagesThesis Cervical Cancerheduurief100% (2)
- DNA VirusesDocument154 pagesDNA VirusesRod Pasion0% (1)
- Cervical CancerDocument23 pagesCervical CancerShinal ChandNo ratings yet
- Colposcopy, Cervical Screening, and HPV, An Issue of Obstetrics and Gynecology Clinics (The Clinics - Internal Medicine)Document155 pagesColposcopy, Cervical Screening, and HPV, An Issue of Obstetrics and Gynecology Clinics (The Clinics - Internal Medicine)Annca RoXanna100% (1)
- Aids - Idsa 2013Document34 pagesAids - Idsa 2013sandykumalaNo ratings yet
- Candida Albicans Infection of Cervix and Comparison of Pap Smear and Culture in DiagnosisDocument4 pagesCandida Albicans Infection of Cervix and Comparison of Pap Smear and Culture in DiagnosisMARIANA CRISTINA DA SILVEIRA LESSANo ratings yet
- Combined Orals APGODocument52 pagesCombined Orals APGOEmilee Tu0% (1)
- OSCE Checklist Cervical Screening SmearDocument2 pagesOSCE Checklist Cervical Screening SmearDemuel Dee L. BertoNo ratings yet
- Pap Smear ChecklistDocument2 pagesPap Smear ChecklistAnonymous HzjO3S100% (1)
- A Case Report of Ayurveda Management of Cervical Cell Dysplasia (Cin 1)Document4 pagesA Case Report of Ayurveda Management of Cervical Cell Dysplasia (Cin 1)IJAR JOURNALNo ratings yet
- Section 11 - Selected Topics in General and Internal MedicineDocument65 pagesSection 11 - Selected Topics in General and Internal MedicineMike GNo ratings yet
- 22 - Atypical Squamous Cells in Liquid-Based CervicalDocument6 pages22 - Atypical Squamous Cells in Liquid-Based CervicalRenan RodriguesNo ratings yet
- TOPICS in Health Care ConceptDocument41 pagesTOPICS in Health Care ConcepthageguroNo ratings yet
- ATLAS ThinPrep TPPTMorphologyLectureDocument116 pagesATLAS ThinPrep TPPTMorphologyLectureCristina CostaNo ratings yet
- Basic Information About Gynecologic CancersDocument26 pagesBasic Information About Gynecologic CancersynaNo ratings yet
- Cervical CancerDocument27 pagesCervical CancerHanif RezaNo ratings yet
- Pap Smear - Overview, Indications, PreparationDocument11 pagesPap Smear - Overview, Indications, PreparationBayu Surya DanaNo ratings yet
- Cervical CancerDocument52 pagesCervical CancerCiiezz BunciiezzNo ratings yet
- Research Project SampleDocument109 pagesResearch Project SampleVincent eneNo ratings yet
- Reproductive Arranged (MedicalBooksVN - Com)Document63 pagesReproductive Arranged (MedicalBooksVN - Com)Rabooh AyashiNo ratings yet