
Chapter 13
Chapter 13
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5824)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Eakin PDFDocument21 pagesEakin PDFAlec McIntoshNo ratings yet
- Thom's Directory of Dublin 1880Document9 pagesThom's Directory of Dublin 1880Geordie Winkle100% (1)
- Should College Athletes Be Paid - FinalDocument7 pagesShould College Athletes Be Paid - Finalapi-509669602No ratings yet
- How We Gain Weight 2018Document18 pagesHow We Gain Weight 2018Alec McIntoshNo ratings yet
- Q2 Compiled Drug ListDocument30 pagesQ2 Compiled Drug ListAlec McIntoshNo ratings yet
- Chapter 12 - Muscle PhysiologyDocument21 pagesChapter 12 - Muscle PhysiologyAlec McIntoshNo ratings yet
- Chapter 8Document12 pagesChapter 8Alec McIntoshNo ratings yet
- Stemcells WidespreadDocument6 pagesStemcells WidespreadAlec McIntoshNo ratings yet
- Catalogo TiendadelhypeDocument6 pagesCatalogo TiendadelhypeCharlyNo ratings yet
- Ruston ProctorDocument14 pagesRuston Proctorpaniczoran100% (1)
- 2023 Winners Edge Individual Time Trial ResultsDocument2 pages2023 Winners Edge Individual Time Trial ResultsBernewsAdminNo ratings yet
- Mock Test Grammar G4Document6 pagesMock Test Grammar G4ratchanee soontreNo ratings yet
- HadesDocument2 pagesHadesapi-313153896No ratings yet
- Group Members Habiba Jameel Raffia Tariq Amina Zahoor ZunairaDocument27 pagesGroup Members Habiba Jameel Raffia Tariq Amina Zahoor ZunairaMuiz SaddozaiNo ratings yet
- Fitt ChartsDocument3 pagesFitt Chartsapi-630179008No ratings yet
- 67168966-G3-Armorers-Manual Part 1Document15 pages67168966-G3-Armorers-Manual Part 1Wilmer Howard BenderNo ratings yet
- Ankit Rathi: Divide 16 Bit Number by 8 Bit NumberDocument20 pagesAnkit Rathi: Divide 16 Bit Number by 8 Bit NumberHamid ArizNo ratings yet
- 07c Injured Job DescriptionDocument1 page07c Injured Job DescriptionMohammed MinhajNo ratings yet
- 11.11 Brand Mega OffersDocument5 pages11.11 Brand Mega OffersBARNEY RAY REAMONNo ratings yet
- s33x UpgradeDocument15 pagess33x UpgradeAlexandre Borges BorgesNo ratings yet
- WODSDocument11 pagesWODSMaria DâmasoNo ratings yet
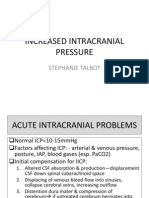
- Increased Intracranial PressureDocument13 pagesIncreased Intracranial PressureStephanie Talbot100% (1)
- UID KH tiềm năngDocument12 pagesUID KH tiềm năngtran duyNo ratings yet
- Training RoutineDocument2 pagesTraining RoutineAakash AhujaNo ratings yet
- YEC BrochureDocument12 pagesYEC BrochureRobCollinsNo ratings yet
- TMPDocument2 pagesTMPkakaroto produccionesNo ratings yet
- The Fourth World: Maroon 5 (Formerly Kara's Flowers) Is An AmericanDocument8 pagesThe Fourth World: Maroon 5 (Formerly Kara's Flowers) Is An AmericanJahnavi SinghNo ratings yet
- The Mars Volta - Cicatriz ESPDocument29 pagesThe Mars Volta - Cicatriz ESPMarco LopesNo ratings yet
- 北興國中111學年度第2學期第3次段考1年級英文題目Document6 pages北興國中111學年度第2學期第3次段考1年級英文題目esther715151No ratings yet
- RushmoreDataExport11-05-2015 12 - 24 - 56Document440 pagesRushmoreDataExport11-05-2015 12 - 24 - 56Anonymous QhsWnAA6No ratings yet
- Homework For Softball PlayersDocument8 pagesHomework For Softball Playersnyvem0domuj3100% (1)
- Parking Brake AssyDocument5 pagesParking Brake AssycipraduNo ratings yet
- Humiliation - Hannah 1Document2 pagesHumiliation - Hannah 1api-751170106No ratings yet
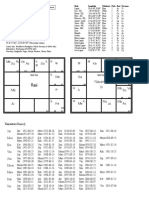
- As Ve Sa Su Me Ra Ke: NavamsaDocument1 pageAs Ve Sa Su Me Ra Ke: NavamsaAstroAnudeepNo ratings yet
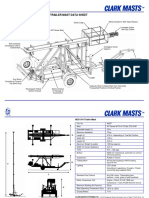
- Model 802/15-6 Standard Duty Trailer Mast Data SheetDocument2 pagesModel 802/15-6 Standard Duty Trailer Mast Data SheetBilly ChrisNo ratings yet
- UNIT2 Health and FitnessDocument6 pagesUNIT2 Health and FitnessY DươngNo ratings yet










































































Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5824)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Eakin PDFDocument21 pagesEakin PDFAlec McIntoshNo ratings yet
- Thom's Directory of Dublin 1880Document9 pagesThom's Directory of Dublin 1880Geordie Winkle100% (1)
- Should College Athletes Be Paid - FinalDocument7 pagesShould College Athletes Be Paid - Finalapi-509669602No ratings yet
- How We Gain Weight 2018Document18 pagesHow We Gain Weight 2018Alec McIntoshNo ratings yet
- Q2 Compiled Drug ListDocument30 pagesQ2 Compiled Drug ListAlec McIntoshNo ratings yet
- Chapter 12 - Muscle PhysiologyDocument21 pagesChapter 12 - Muscle PhysiologyAlec McIntoshNo ratings yet
- Chapter 8Document12 pagesChapter 8Alec McIntoshNo ratings yet
- Stemcells WidespreadDocument6 pagesStemcells WidespreadAlec McIntoshNo ratings yet
- Catalogo TiendadelhypeDocument6 pagesCatalogo TiendadelhypeCharlyNo ratings yet
- Ruston ProctorDocument14 pagesRuston Proctorpaniczoran100% (1)
- 2023 Winners Edge Individual Time Trial ResultsDocument2 pages2023 Winners Edge Individual Time Trial ResultsBernewsAdminNo ratings yet
- Mock Test Grammar G4Document6 pagesMock Test Grammar G4ratchanee soontreNo ratings yet
- HadesDocument2 pagesHadesapi-313153896No ratings yet
- Group Members Habiba Jameel Raffia Tariq Amina Zahoor ZunairaDocument27 pagesGroup Members Habiba Jameel Raffia Tariq Amina Zahoor ZunairaMuiz SaddozaiNo ratings yet
- Fitt ChartsDocument3 pagesFitt Chartsapi-630179008No ratings yet
- 67168966-G3-Armorers-Manual Part 1Document15 pages67168966-G3-Armorers-Manual Part 1Wilmer Howard BenderNo ratings yet
- Ankit Rathi: Divide 16 Bit Number by 8 Bit NumberDocument20 pagesAnkit Rathi: Divide 16 Bit Number by 8 Bit NumberHamid ArizNo ratings yet
- 07c Injured Job DescriptionDocument1 page07c Injured Job DescriptionMohammed MinhajNo ratings yet
- 11.11 Brand Mega OffersDocument5 pages11.11 Brand Mega OffersBARNEY RAY REAMONNo ratings yet
- s33x UpgradeDocument15 pagess33x UpgradeAlexandre Borges BorgesNo ratings yet
- WODSDocument11 pagesWODSMaria DâmasoNo ratings yet
- Increased Intracranial PressureDocument13 pagesIncreased Intracranial PressureStephanie Talbot100% (1)
- UID KH tiềm năngDocument12 pagesUID KH tiềm năngtran duyNo ratings yet
- Training RoutineDocument2 pagesTraining RoutineAakash AhujaNo ratings yet
- YEC BrochureDocument12 pagesYEC BrochureRobCollinsNo ratings yet
- TMPDocument2 pagesTMPkakaroto produccionesNo ratings yet
- The Fourth World: Maroon 5 (Formerly Kara's Flowers) Is An AmericanDocument8 pagesThe Fourth World: Maroon 5 (Formerly Kara's Flowers) Is An AmericanJahnavi SinghNo ratings yet
- The Mars Volta - Cicatriz ESPDocument29 pagesThe Mars Volta - Cicatriz ESPMarco LopesNo ratings yet
- 北興國中111學年度第2學期第3次段考1年級英文題目Document6 pages北興國中111學年度第2學期第3次段考1年級英文題目esther715151No ratings yet
- RushmoreDataExport11-05-2015 12 - 24 - 56Document440 pagesRushmoreDataExport11-05-2015 12 - 24 - 56Anonymous QhsWnAA6No ratings yet
- Homework For Softball PlayersDocument8 pagesHomework For Softball Playersnyvem0domuj3100% (1)
- Parking Brake AssyDocument5 pagesParking Brake AssycipraduNo ratings yet
- Humiliation - Hannah 1Document2 pagesHumiliation - Hannah 1api-751170106No ratings yet
- As Ve Sa Su Me Ra Ke: NavamsaDocument1 pageAs Ve Sa Su Me Ra Ke: NavamsaAstroAnudeepNo ratings yet
- Model 802/15-6 Standard Duty Trailer Mast Data SheetDocument2 pagesModel 802/15-6 Standard Duty Trailer Mast Data SheetBilly ChrisNo ratings yet
- UNIT2 Health and FitnessDocument6 pagesUNIT2 Health and FitnessY DươngNo ratings yet