Download as pdf or txt
You might also like
- Generic Name: Classification: IndicationDocument2 pagesGeneric Name: Classification: IndicationKristine YoungNo ratings yet
- Proper Use of Medicines: Lesson 10Document3 pagesProper Use of Medicines: Lesson 10Johnpaul LarozaNo ratings yet
- ClindamycinDocument5 pagesClindamycinDarwyn Paul DagumanNo ratings yet
- Crusted (Norwegian) Scabies Following Systemic and Topical Corticosteroid TherapyDocument4 pagesCrusted (Norwegian) Scabies Following Systemic and Topical Corticosteroid TherapysfiahyusnitaNo ratings yet
- Correspondence: Peritonitis Due To Multiresistant Rhizobium RadiobacterDocument5 pagesCorrespondence: Peritonitis Due To Multiresistant Rhizobium RadiobacterFrontiersNo ratings yet
- Toxic Epidermal Necrolysis A Case ReportDocument3 pagesToxic Epidermal Necrolysis A Case ReportResearch ParkNo ratings yet
- ASIA Syndrome Following Breast Implant Placement: Case CommunicationsDocument3 pagesASIA Syndrome Following Breast Implant Placement: Case Communicationssilvana31No ratings yet
- RF - Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis: A Treatment UpdateDocument2 pagesRF - Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis: A Treatment Updatedoc.kentoNo ratings yet
- Biologics - SynopsisDocument12 pagesBiologics - SynopsisWei Sheng ChongNo ratings yet
- Jurnal P.acnesDocument4 pagesJurnal P.acnesFazlicha SyaradilaNo ratings yet
- Case Vitiligo 1Document2 pagesCase Vitiligo 1Nguyễn Lê BằngNo ratings yet
- ScrofulodermDocument4 pagesScrofulodermIzmi AzizahNo ratings yet
- Rapid Response To Acitretin Combined With Cryotherapy For Extensive and Recalcitrant Verruca Vulgaris On The ScalpDocument4 pagesRapid Response To Acitretin Combined With Cryotherapy For Extensive and Recalcitrant Verruca Vulgaris On The ScalpNada Utami PrahastiwiNo ratings yet
- Treatment of Toxic Epidermal Necrolysis With Intravenous ImmunoglobulinDocument5 pagesTreatment of Toxic Epidermal Necrolysis With Intravenous ImmunoglobulinUbaidillah HafidzNo ratings yet
- Acute Necrotizing Sinusitis Caused by Staphylococcus Lugdunensis 2011Document3 pagesAcute Necrotizing Sinusitis Caused by Staphylococcus Lugdunensis 2011J Sebastian PeinadoNo ratings yet
- JA A D: M CAD ErmatolDocument2 pagesJA A D: M CAD ErmatolCristian QuitoNo ratings yet
- Medicine: An Unusual Extranodal Natural Killer/t-Cell Lymphoma Presenting As Chronic LaryngitisDocument4 pagesMedicine: An Unusual Extranodal Natural Killer/t-Cell Lymphoma Presenting As Chronic Laryngitisnurul atika havizNo ratings yet
- Dermatochalasis CN Chua Et AlDocument4 pagesDermatochalasis CN Chua Et AlEndrianus Jaya PutraNo ratings yet
- A Case Report On Steroid Induced Acneiform EruptionsDocument3 pagesA Case Report On Steroid Induced Acneiform EruptionsVidini Kusuma AjiNo ratings yet
- Wang 2019Document7 pagesWang 2019PippoNo ratings yet
- Nekrolisis Epidermal Toksik Ec KotrimoksasolDocument6 pagesNekrolisis Epidermal Toksik Ec KotrimoksasolIrgi PutraNo ratings yet
- Falzon 2010Document3 pagesFalzon 2010dhanoushk.jr2023No ratings yet
- Dechlorane Plus and Related Compounds in Peregrine Falcon (Falco Peregrinus) Eggs From Canada and SpainDocument6 pagesDechlorane Plus and Related Compounds in Peregrine Falcon (Falco Peregrinus) Eggs From Canada and SpainlacosNo ratings yet
- Correspondence: Idiopathic Recurrent Subconjunctival HemorrhageDocument2 pagesCorrespondence: Idiopathic Recurrent Subconjunctival HemorrhageSatrya DitaNo ratings yet
- Imprimir 2Document3 pagesImprimir 2Gino VitteriNo ratings yet
- CVS MMP SGSDocument7 pagesCVS MMP SGSNUR RADHIAH MOHD SAZLINo ratings yet
- Penetrating Keratoplasty in Active Acanthamoeba KeratitisDocument5 pagesPenetrating Keratoplasty in Active Acanthamoeba Keratitisdrvishalkulkarni2007No ratings yet
- BCR 2019 233131Document5 pagesBCR 2019 233131jhordyafsNo ratings yet
- Pi Is 2213260022001862Document11 pagesPi Is 2213260022001862Zainab MohamedNo ratings yet
- Cutaneous Polyarteritis Nodosa in A Child FollowinDocument2 pagesCutaneous Polyarteritis Nodosa in A Child FollowinandresrogersNo ratings yet
- Infectious Diseases IIDocument57 pagesInfectious Diseases IIAhmad MakhloufNo ratings yet
- Of Vaginal Candidosis With Econazole Nitrate and Nystatin: TreatmentDocument4 pagesOf Vaginal Candidosis With Econazole Nitrate and Nystatin: TreatmentMuthanna Lo'ayNo ratings yet
- A Comparison of Local and in The of Herpetic Disciform KeratitisDocument4 pagesA Comparison of Local and in The of Herpetic Disciform KeratitisAndi Raodah ImranNo ratings yet
- Scrofuloderma: Images in DermatologyDocument1 pageScrofuloderma: Images in DermatologyAkira MasumiNo ratings yet
- Lichenoid Drug Reaction To Antituberculosis Drugs Treated Through With Topical Steroids and PhototherapyDocument3 pagesLichenoid Drug Reaction To Antituberculosis Drugs Treated Through With Topical Steroids and PhototherapyChristabella Natalia WijayaNo ratings yet
- complete wart treatment, two cases of warts treated with isotretinoin, recalcitrant genital warts case reports, Dr Rahul kumar sharma skin specialist ajmer , Dermatologist ajmer, cases of warts, condylomataDocument3 pagescomplete wart treatment, two cases of warts treated with isotretinoin, recalcitrant genital warts case reports, Dr Rahul kumar sharma skin specialist ajmer , Dermatologist ajmer, cases of warts, condylomataRahul SharmaNo ratings yet
- Hon 2005Document2 pagesHon 2005Andana TrisaviNo ratings yet
- Case Report: Saudi Journal of Kidney Diseases and TransplantationDocument4 pagesCase Report: Saudi Journal of Kidney Diseases and TransplantationWilber Roberto Ticona MamaniNo ratings yet
- Case Study (Serencio's Group) FINALDocument4 pagesCase Study (Serencio's Group) FINALMarjorie EragNo ratings yet
- 4.1 Pemphigus: Case 38 Pemphigus Vulgaris (Involving The Skin and Oral Mucosa) BDocument16 pages4.1 Pemphigus: Case 38 Pemphigus Vulgaris (Involving The Skin and Oral Mucosa) BIrma NovitasariNo ratings yet
- Acute Transverse Myelitis After COVID-19 VaccinationDocument7 pagesAcute Transverse Myelitis After COVID-19 VaccinationMing-Jen TsaiNo ratings yet
- Fimmu 13 1022093Document14 pagesFimmu 13 1022093Wojciech WawrętyNo ratings yet
- DRES SindromeDocument6 pagesDRES SindromeleslyjanetNo ratings yet
- 6689-23393-1-PB LaDocument5 pages6689-23393-1-PB Laasnia rahmawatiNo ratings yet
- BCR 2019 233946Document2 pagesBCR 2019 233946Paola AlcocerNo ratings yet
- Lupus SeverDocument3 pagesLupus SeverdeliaNo ratings yet
- Daptomycin 5Document2 pagesDaptomycin 5SachithNo ratings yet
- Disseminated Tuberculous Myositis in A Child With Acut 2009 Pediatrics NeoDocument4 pagesDisseminated Tuberculous Myositis in A Child With Acut 2009 Pediatrics NeoFrankenstein MelancholyNo ratings yet
- AACE Clinical Case Reports: Kyrstin L. Lane, MD, Ari Weinreb, MD, Kira Chow, MD, Jane Weinreb, MDDocument2 pagesAACE Clinical Case Reports: Kyrstin L. Lane, MD, Ari Weinreb, MD, Kira Chow, MD, Jane Weinreb, MDShuaib AhmedNo ratings yet
- Nejmcpc 2115847Document10 pagesNejmcpc 2115847j8hcyh8j2jNo ratings yet
- Alsberg 1 s2.0 S2451993621002279 MainDocument5 pagesAlsberg 1 s2.0 S2451993621002279 MainDoug PulaNo ratings yet
- Tosca 1996Document7 pagesTosca 1996HEARTJUGGLERNo ratings yet
- JA A D: M CAD ErmatolDocument2 pagesJA A D: M CAD ErmatolSuzana SoozyNo ratings yet
- Larotrectinib FIBROSARCOMA INFANTILDocument5 pagesLarotrectinib FIBROSARCOMA INFANTILJOHN LOPERANo ratings yet
- Infectious DiseasesDocument41 pagesInfectious DiseasesPharmacotherapy100% (2)
- Meningitis TBC Lancet PDFDocument11 pagesMeningitis TBC Lancet PDFGustavo MartinezNo ratings yet
- Antibiotic Induced Black Hairy TongueDocument11 pagesAntibiotic Induced Black Hairy TongueYuganya SriNo ratings yet
- E. Coli CellulitisDocument7 pagesE. Coli CellulitisBelajar KedokteranNo ratings yet
- A Long-Term Followup of 30 Neuropsychiatric-Tuberculosis Patients With The "Open-Negative" Syndrome of Indefinitely Prolonged ChemotherapyDocument7 pagesA Long-Term Followup of 30 Neuropsychiatric-Tuberculosis Patients With The "Open-Negative" Syndrome of Indefinitely Prolonged ChemotherapyRiot Riot AdjaNo ratings yet
- Case Report Benign Mucosal Membrane Pemphigoid As A Differential Diagnosis of Necrotizing Periodontal DiseaseDocument4 pagesCase Report Benign Mucosal Membrane Pemphigoid As A Differential Diagnosis of Necrotizing Periodontal DiseaseYeni PuspitasariNo ratings yet
- Debreceni2006 PDFDocument5 pagesDebreceni2006 PDFAnderson CarvalhoNo ratings yet
- LEAFLETLEWDocument1 pageLEAFLETLEWLewishoppusNo ratings yet
- Anggi Lewis R.P Aruan 1161050113Document1 pageAnggi Lewis R.P Aruan 1161050113LewishoppusNo ratings yet
- Ophtalmology Record Corneal Ulcer: Anggi Lewis R P Aruan 1161050113Document7 pagesOphtalmology Record Corneal Ulcer: Anggi Lewis R P Aruan 1161050113LewishoppusNo ratings yet
- Ophtalmology Record Corneal Ulcer: Anggi Lewis R P Aruan 1161050113Document7 pagesOphtalmology Record Corneal Ulcer: Anggi Lewis R P Aruan 1161050113LewishoppusNo ratings yet
- 1 - Internal Medicine UKIDocument128 pages1 - Internal Medicine UKILewishoppusNo ratings yet
- Case Report: Subcorneal Pustular Dermatosis An Immnohisto-Pathological PerspectiveDocument4 pagesCase Report: Subcorneal Pustular Dermatosis An Immnohisto-Pathological PerspectiveLewishoppusNo ratings yet
- Pi Is 0190962214011566Document2 pagesPi Is 0190962214011566LewishoppusNo ratings yet
- Stop Bull YubDocument1 pageStop Bull YubLewishoppusNo ratings yet
- Timeline Gizi PKMDocument13 pagesTimeline Gizi PKMLewishoppusNo ratings yet
- Lamhot PurbaDocument7 pagesLamhot PurbaLewishoppusNo ratings yet
- ROSADocument9 pagesROSAREZA ARY FACHRURROZINo ratings yet
- Birth Control Effectiveness Wall Chart Front and Back 8-03-2015Document2 pagesBirth Control Effectiveness Wall Chart Front and Back 8-03-2015api-286375746100% (1)
- Antirheumatic and Antigout DrugsDocument66 pagesAntirheumatic and Antigout DrugsBadri KarkiNo ratings yet
- Adcetris Drug StudyDocument7 pagesAdcetris Drug StudyHUSAIN, HAIZIAH-YASMINNo ratings yet
- Ascorbic Acid: Generic Name Brand Name ManufacturerDocument6 pagesAscorbic Acid: Generic Name Brand Name ManufacturerJant Joyce U. UlepNo ratings yet
- Drug Study RivastigmineDocument6 pagesDrug Study RivastigmineRaijenne VersolaNo ratings yet
- Pharma Parenteral Dosage CalculationDocument3 pagesPharma Parenteral Dosage CalculationMaxinne RoseñoNo ratings yet
- IUB 401 Ch1 IntroADocument56 pagesIUB 401 Ch1 IntroAMahmud IslamNo ratings yet
- CefalexinDocument1 pageCefalexinIvan Matthew SuperioNo ratings yet
- Moderna Files For Authorization of Its COVID 19 Vaccine in Young Children Six Months To Under Six Years of Age 2022Document4 pagesModerna Files For Authorization of Its COVID 19 Vaccine in Young Children Six Months To Under Six Years of Age 2022Aristegui NoticiasNo ratings yet
- Chapter 43: Antiulcer Drugs Mccuistion: Pharmacology: A Patient-Centered Nursing Process Approach, 10Th EditionDocument95 pagesChapter 43: Antiulcer Drugs Mccuistion: Pharmacology: A Patient-Centered Nursing Process Approach, 10Th Editionmichael patterson100% (1)
- MLP by StateDocument12 pagesMLP by StateFlor OMNo ratings yet
- Drug Profile: Lahore Pharmacy CollegeDocument18 pagesDrug Profile: Lahore Pharmacy CollegeShivangi SharmaNo ratings yet
- Name of The Medicinal Product: Short-Term TreatmentDocument10 pagesName of The Medicinal Product: Short-Term TreatmentasdwasdNo ratings yet
- CEFUROXIMEDocument3 pagesCEFUROXIMEGwyn RosalesNo ratings yet
- Endocrine Drug ChartDocument1 pageEndocrine Drug ChartJessicaNo ratings yet
- 1.2 Patient Care Coordinator DepartmentDocument16 pages1.2 Patient Care Coordinator DepartmentIurii IuriiNo ratings yet
- Sympatheticnervous System (SNS) Parasympathetic Nervous System (PNS)Document2 pagesSympatheticnervous System (SNS) Parasympathetic Nervous System (PNS)Jhevilin RMNo ratings yet
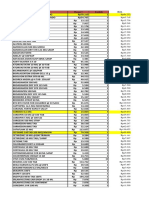
- Stock 05 Mei 23 PDFDocument51 pagesStock 05 Mei 23 PDFRomandaniNo ratings yet
- PHARMACOLOGYDocument42 pagesPHARMACOLOGYrbishestaNo ratings yet
- Controlled Drug Prescribing OSCE GuideDocument3 pagesControlled Drug Prescribing OSCE GuideAdil IslamNo ratings yet
- Farmasetika II - AnalgetikDocument15 pagesFarmasetika II - AnalgetikNur FitriNo ratings yet
- Dialysis DrugsDocument51 pagesDialysis Drugslimkokhui100% (2)
- Ticagrelor - Changing Paradigm in ACS ManagementDocument42 pagesTicagrelor - Changing Paradigm in ACS ManagementBudi WirawanNo ratings yet
- Drug CalculationDocument14 pagesDrug CalculationAbegail FloresNo ratings yet
- Statement From Marathon Pharmaceuticals On EmflazaDocument4 pagesStatement From Marathon Pharmaceuticals On EmflazaNed PagliaruloNo ratings yet
- Do Not CrushOral Dosage Forms That Should Not Be Crushed 2015Document15 pagesDo Not CrushOral Dosage Forms That Should Not Be Crushed 2015hunainahmed13No ratings yet
- Lap Ranap 2020Document193 pagesLap Ranap 2020Putu Alen RenaldoNo ratings yet