Download as pdf or txt
You might also like
- Endocrine Anesthesia MCQsDocument18 pagesEndocrine Anesthesia MCQsMuhammad Aasim Maan100% (2)
- Anaesthesia Equipment: Anaesthetics OSCE (Compiled by C Lee Kin) 1Document98 pagesAnaesthesia Equipment: Anaesthetics OSCE (Compiled by C Lee Kin) 1Shen BNo ratings yet
- Primitive Man and His Food - Arnold DeVriesDocument97 pagesPrimitive Man and His Food - Arnold DeVriessamui11No ratings yet
- Anesthesiology Resident Manual of Procedures: A Step-by-Step GuideFrom EverandAnesthesiology Resident Manual of Procedures: A Step-by-Step GuideNo ratings yet
- 05 IV Induction Agents PDFDocument0 pages05 IV Induction Agents PDFjuniorebinda100% (1)
- Anesthesiology Case PresDocument25 pagesAnesthesiology Case PresKirstin100% (1)
- Obs Gynae Full Summary NotesDocument41 pagesObs Gynae Full Summary NotesJana Aldour100% (1)
- Aipgmee 2008 Merit ListDocument53 pagesAipgmee 2008 Merit ListPraveen RadhakrishnanNo ratings yet
- Yoga Therapy For KneesDocument3 pagesYoga Therapy For Kneesgnostication100% (2)
- History Taking in OrthopaedicsDocument23 pagesHistory Taking in OrthopaedicsPrachi Gupta100% (1)
- Pre Eclampsia Eclampsia Guideline For The Management of SevereDocument15 pagesPre Eclampsia Eclampsia Guideline For The Management of SevereMelanie JuntakNo ratings yet
- Epidural AnaesthesiaDocument13 pagesEpidural AnaesthesiajuniorebindaNo ratings yet
- Anaesthesia Notes For PGDocument11 pagesAnaesthesia Notes For PGskycall28No ratings yet
- Anaesthesia For Casarean DeliveryDocument109 pagesAnaesthesia For Casarean DeliveryMohammed Shahnawaz HussainNo ratings yet
- Management of Pregnancy Related BleedingDocument75 pagesManagement of Pregnancy Related BleedingChuah Wei Hong100% (1)
- 21 Obstetric Anaesthesia PDFDocument0 pages21 Obstetric Anaesthesia PDFjuniorebindaNo ratings yet
- Management of Cardiac Disease in PregnancyDocument7 pagesManagement of Cardiac Disease in PregnancyMegavarnen Gobinathan100% (1)
- Textbook of Anaesthesia For Postgraduates PDFDocument1,218 pagesTextbook of Anaesthesia For Postgraduates PDFMohammad HayajnehNo ratings yet
- Anesthetic AgentsDocument7 pagesAnesthetic AgentsJan DacioNo ratings yet
- ANESTHESIA in OBSTETRICSDocument159 pagesANESTHESIA in OBSTETRICSemma rose lutellaNo ratings yet
- Ectopic PregnancyDocument5 pagesEctopic PregnancyFaith FuentevillaNo ratings yet
- Anesthesia One Liner PDFDocument13 pagesAnesthesia One Liner PDFMinaz PatelNo ratings yet
- STAGES of AnesthesiaDocument4 pagesSTAGES of AnesthesiaMabz Posadas BisnarNo ratings yet
- ERAS Guidelines PDFDocument8 pagesERAS Guidelines PDFWadezigNo ratings yet
- 12.intraoperative Fluid ManagmentDocument54 pages12.intraoperative Fluid ManagmentyeabsraNo ratings yet
- Epidural AnesthesiaDocument5 pagesEpidural AnesthesiaImran MukhlessNo ratings yet
- Obstetric AnesthesiaDocument35 pagesObstetric AnesthesiaMuhammad Zulkifli100% (1)
- Cme Fluid and Electrolytes 2902016Document37 pagesCme Fluid and Electrolytes 2902016Mohd Faie Ramli0% (1)
- Vasodilators 1233318450814478 3Document29 pagesVasodilators 1233318450814478 3Nehal AmjadNo ratings yet
- CH 46 Complications of AnaesthesiaDocument29 pagesCH 46 Complications of AnaesthesiaChristian LeepoNo ratings yet
- Obestetrics Gynecology PDFDocument192 pagesObestetrics Gynecology PDFdrazam5314No ratings yet
- Conduct of AnaesthesiaDocument30 pagesConduct of AnaesthesiaAnirban PalNo ratings yet
- Anesthetic Challenges and Successful Management of Uncorrected Tetralogy of Fallot (Tof) in PregnancyDocument3 pagesAnesthetic Challenges and Successful Management of Uncorrected Tetralogy of Fallot (Tof) in PregnancyIJAR JOURNALNo ratings yet
- PPH by Dr. Rajabu Nyangara MtillyDocument38 pagesPPH by Dr. Rajabu Nyangara MtillynyangaraNo ratings yet
- Local Anesthetics Used For Spinal Anesthesia: Abdirahman Dahir Wais (BSN, Anesthetist)Document39 pagesLocal Anesthetics Used For Spinal Anesthesia: Abdirahman Dahir Wais (BSN, Anesthetist)Abdi MohamedNo ratings yet
- Antepartum HemorrhageDocument12 pagesAntepartum HemorrhageMohammed AbdNo ratings yet
- Obstetrics AnesthesiaDocument55 pagesObstetrics AnesthesiaJohn Paulo Catacutan100% (2)
- How To Read A CTGDocument11 pagesHow To Read A CTGiwennieNo ratings yet
- Hypertensive Disorders in Pregnancy (Williams 22 Edition)Document88 pagesHypertensive Disorders in Pregnancy (Williams 22 Edition)bagir_dm1067% (3)
- Obstructed Labor AND ITS CAUSE, CORD PROLAPS AND PRESENTATIONDocument59 pagesObstructed Labor AND ITS CAUSE, CORD PROLAPS AND PRESENTATIONmaezu100% (2)
- Management of PPHDocument24 pagesManagement of PPHMutabazi SharifNo ratings yet
- Heart Diseases in PregnancyDocument19 pagesHeart Diseases in PregnancyKirubah Sai PatnaikNo ratings yet
- Surgical Treatment of Traumatic PPHDocument23 pagesSurgical Treatment of Traumatic PPHAyushi GuptaNo ratings yet
- Enhanced Recovery After Surgery: Nutrition Issues in Gastroenterology, Series #151Document15 pagesEnhanced Recovery After Surgery: Nutrition Issues in Gastroenterology, Series #151Hendry DimasNo ratings yet
- Obstetric EmergenciesDocument15 pagesObstetric EmergenciesAndi SaputraNo ratings yet
- Anesthetic Considerations For Ambulatory Anesthesia: Advantages of Ambulatory SurgeryDocument4 pagesAnesthetic Considerations For Ambulatory Anesthesia: Advantages of Ambulatory SurgeryIsabel CastilloNo ratings yet
- Anesthetic Consideration in Hypertensive PatientDocument11 pagesAnesthetic Consideration in Hypertensive PatientYosiAsmaraNo ratings yet
- Pregnancy With Cardiac DiseaseDocument16 pagesPregnancy With Cardiac DiseasemiaputeriNo ratings yet
- Revision Long Case Obs GynaeDocument10 pagesRevision Long Case Obs GynaeHo Yong WaiNo ratings yet
- Anesthesia For Cesarean SectionDocument60 pagesAnesthesia For Cesarean Sectionmaheralrwimi100% (1)
- ObGyn Concise Notes NEET-PGDocument57 pagesObGyn Concise Notes NEET-PGMohamed TayyabNo ratings yet
- Tetanus Treatment & Management - Approach Considerations, Initial Supportive Therapy and Wound Care, Pharmacologic TherapyDocument11 pagesTetanus Treatment & Management - Approach Considerations, Initial Supportive Therapy and Wound Care, Pharmacologic TherapyFuad Adi PrasetyoNo ratings yet
- OB1 Lec - AnalgesiaDocument3 pagesOB1 Lec - Analgesiaapi-3700579No ratings yet
- Anaesthesia For Thyroid Surgery....Document46 pagesAnaesthesia For Thyroid Surgery....Parvathy R NairNo ratings yet
- Dr. P.Narasimha Reddy, MD Da Narayana Medical College, NelloreDocument90 pagesDr. P.Narasimha Reddy, MD Da Narayana Medical College, NelloreJaybee SarmientoNo ratings yet
- Journal ClubDocument26 pagesJournal Clubysindhura23gmailcom100% (1)
- General Anesthesia: Presented By: Shalakha Bhardwaj BDS Final Year (2007-2011)Document85 pagesGeneral Anesthesia: Presented By: Shalakha Bhardwaj BDS Final Year (2007-2011)KrishnaBihariShuklaNo ratings yet
- Hepatic EncephalopathyDocument3 pagesHepatic EncephalopathySuhas KandeNo ratings yet
- Er DrugsDocument4 pagesEr Drugsanne_18No ratings yet
- Anemia and AnesthesiaDocument11 pagesAnemia and AnesthesialhalamNo ratings yet
- Technique For Awake Fibre Optic IntubationDocument3 pagesTechnique For Awake Fibre Optic Intubationmonir61No ratings yet
- A Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Essentials for Practice of Medicine in the Frontline: From Tropical Africa; Pleasantly Different Volume 2From EverandEssentials for Practice of Medicine in the Frontline: From Tropical Africa; Pleasantly Different Volume 2Rating: 5 out of 5 stars5/5 (1)
- Prevention Identification and Management of PE EclampsiaDocument15 pagesPrevention Identification and Management of PE EclampsiaRuva Oscass JimmyNo ratings yet
- Kerala Medico Legal CodeDocument161 pagesKerala Medico Legal CodePraveen RadhakrishnanNo ratings yet
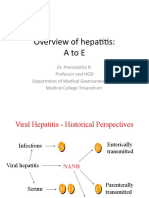
- Overview of Hepatitis: AtoeDocument40 pagesOverview of Hepatitis: AtoePraveen RadhakrishnanNo ratings yet
- Keralapg Medical 2013 Merit ListDocument89 pagesKeralapg Medical 2013 Merit ListPraveen RadhakrishnanNo ratings yet
- Kerala PG Medical Senority List 2013Document37 pagesKerala PG Medical Senority List 2013Praveen RadhakrishnanNo ratings yet
- Simple MastectomyDocument3 pagesSimple MastectomyCindy DayocNo ratings yet
- Essentials of Abnormal Psychology 8th Edition Durand Test BankDocument43 pagesEssentials of Abnormal Psychology 8th Edition Durand Test Bankvenerealembolism93fNo ratings yet
- Int Endodontic J - 2018 - Kim - Regenerative Endodontics A Comprehensive ReviewDocument22 pagesInt Endodontic J - 2018 - Kim - Regenerative Endodontics A Comprehensive ReviewCyber MagicNo ratings yet
- Anxiety, Stress, & Coping: An International Journal: Click For UpdatesDocument34 pagesAnxiety, Stress, & Coping: An International Journal: Click For Updateskarine schmidtNo ratings yet
- Aha Guidelines For StemiDocument94 pagesAha Guidelines For StemiBeny Rilianto100% (1)
- Wound Cleansing: Benefits of Hypochlorous AcidDocument5 pagesWound Cleansing: Benefits of Hypochlorous Acidlps DiamondNo ratings yet
- Causes and Treatment of DepressionDocument12 pagesCauses and Treatment of DepressionGEETA MOHANNo ratings yet
- Revalida Review NotesDocument14 pagesRevalida Review NotesBryan Lloyd RayatNo ratings yet
- Jurnal CA RektiDocument8 pagesJurnal CA RektiIvan HoNo ratings yet
- Pharmacotherapy of Anxiety Disorders: Current and Emerging Treatment OptionsDocument21 pagesPharmacotherapy of Anxiety Disorders: Current and Emerging Treatment OptionsGabriel Vargas CuadrosNo ratings yet
- Pembahasan Kuis 7 Ppu - Bahasa Inggris: B.Inggris Persiapan Utbk 2021Document8 pagesPembahasan Kuis 7 Ppu - Bahasa Inggris: B.Inggris Persiapan Utbk 202154 Hilmi Nur PersadaNo ratings yet
- Kapal KapalDocument2 pagesKapal KapalVishal PatelNo ratings yet
- ResumeDocument2 pagesResumeapi-291740538No ratings yet
- First Aid Safety Meeting TopicsDocument79 pagesFirst Aid Safety Meeting TopicsSrikanth BammhideNo ratings yet
- HTT 10 ManualDocument9 pagesHTT 10 ManualJack StrongNo ratings yet
- DrChi PART 1 October3Document325 pagesDrChi PART 1 October3jayjonbeach100% (1)
- Nursing Philosophy FinalDocument7 pagesNursing Philosophy Finalapi-429837528100% (1)
- The Burke Lateropulsion Scale and Addressing Pusher Syndrome Post-Cva 1Document12 pagesThe Burke Lateropulsion Scale and Addressing Pusher Syndrome Post-Cva 1api-621048040No ratings yet
- FOLLOW UP FORM Pharmacy StudentsDocument2 pagesFOLLOW UP FORM Pharmacy Studentsbala muruganNo ratings yet
- Dura Mastic DatasheetDocument4 pagesDura Mastic DatasheetBhisamS SallehNo ratings yet
- Aqua TabsDocument3 pagesAqua TabsShakti ShonaNo ratings yet
- Robotic UrologyDocument279 pagesRobotic UrologyZICONo ratings yet
- ECG in Emergency Medicine (2006)Document234 pagesECG in Emergency Medicine (2006)EcoGert100% (1)
- DR Khaled Final Exam MCQ 2012 - 2013Document89 pagesDR Khaled Final Exam MCQ 2012 - 2013ﻣﻠﻚ عيسى100% (2)
- Resume EportfolioDocument1 pageResume Eportfolioapi-253211220No ratings yet
- 3D Treatment Planning in Head & NeckDocument29 pages3D Treatment Planning in Head & NeckErick Natividad Zevallos0% (1)
- Pulmonary TuberculosisDocument17 pagesPulmonary TuberculosisRobert Dominic GonzalesNo ratings yet