Download as docx, pdf, or txt
You might also like
- Nephrotic Syndrome PathophysiologyDocument1 pageNephrotic Syndrome PathophysiologyKrisianne Mae Lorenzo FranciscoNo ratings yet
- ACS PathophysiologyDocument2 pagesACS PathophysiologyFerliza OblenaNo ratings yet
- Cardiology II WorkbookDocument70 pagesCardiology II WorkbookPharmacist Dina100% (1)
- Pahtophysiology of EsrdDocument5 pagesPahtophysiology of EsrdCarl JardelezaNo ratings yet
- Pathophysiology of NephrosclerosisDocument2 pagesPathophysiology of NephrosclerosisJessica Damasen Caballero0% (1)
- Cancer Schematic DiagramDocument1 pageCancer Schematic DiagramCyrus De Asis100% (4)
- Pathophysiology of DMDocument4 pagesPathophysiology of DMNicole Louise N. VillanuevaNo ratings yet
- Hypertension PathophysiologyDocument1 pageHypertension PathophysiologyZaida Eunice EstabayaNo ratings yet
- Urinary Tract Infection Anatomy and PhysiologyDocument12 pagesUrinary Tract Infection Anatomy and PhysiologyPaul Anthony Centeno PimentelNo ratings yet
- Cancer Pathophysiology To Be EditedDocument5 pagesCancer Pathophysiology To Be EditedEyySiEffVeeNo ratings yet
- Professional Review Guidance Notes - 2 PDFDocument9 pagesProfessional Review Guidance Notes - 2 PDFalanmoore123100% (1)
- Pathophy - Nephrotic SyndromeedDocument1 pagePathophy - Nephrotic Syndromeedianecunar100% (1)
- Pathophysiology of HyperthyroidismDocument4 pagesPathophysiology of HyperthyroidismKitty YuffieNo ratings yet
- "Acute Coronary Syndrome Non ST Elevation Myocardial Infarction, Hypertensive Cardiovascular Disease, Diabetes Mellitus Type 2, and Community Acquired Pneumonia" Client Centered PathophysiologyDocument3 pages"Acute Coronary Syndrome Non ST Elevation Myocardial Infarction, Hypertensive Cardiovascular Disease, Diabetes Mellitus Type 2, and Community Acquired Pneumonia" Client Centered PathophysiologyCarl Elexer Cuyugan Ano50% (2)
- HCVDDocument5 pagesHCVDkhrizaleehNo ratings yet
- Pa Tho Physiology Sle, CompDocument5 pagesPa Tho Physiology Sle, CompHassan Bj MarabongNo ratings yet
- Schistosomiasis (From Anatomy To Pathophysiology)Document10 pagesSchistosomiasis (From Anatomy To Pathophysiology)Tiger Knee100% (1)
- Hypertensive NephrosclerosisDocument14 pagesHypertensive Nephrosclerosisreysanne100% (2)
- DB13 - Pathophysiology of AtherosclerosisDocument2 pagesDB13 - Pathophysiology of Atherosclerosisi_vhie03No ratings yet
- Pathophysiology CKDDocument2 pagesPathophysiology CKDSugar Capule - ManuelNo ratings yet
- Schematic Diagram Pathophysiology (Book-Based) COPD and TuberculosisDocument1 pageSchematic Diagram Pathophysiology (Book-Based) COPD and Tuberculosispragna novaNo ratings yet
- Lupus Case ReportDocument1 pageLupus Case ReportMendy HararyNo ratings yet
- PathophysiologyDocument4 pagesPathophysiologyAngelou Joefred Congreso100% (1)
- Bachelor of Nursing Science With HonoursDocument17 pagesBachelor of Nursing Science With HonoursMaryam HasanahNo ratings yet
- CASE STUDY PheumoniaDocument5 pagesCASE STUDY PheumoniaEdelweiss Marie CayetanoNo ratings yet
- Potts Disease Case AnalysisDocument5 pagesPotts Disease Case AnalysisAdrian MallarNo ratings yet
- Pathophysiology of Type II Diabetes MellitusDocument1 pagePathophysiology of Type II Diabetes MellitusMarion Mendez100% (1)
- Acute Glomerulonephritis: Gordon Sara Sonnya Ayutthaya Novita Sari DewiDocument12 pagesAcute Glomerulonephritis: Gordon Sara Sonnya Ayutthaya Novita Sari DewiSara Sonnya Ayutthaya NapitupuluNo ratings yet
- Pathophysiology of Diabetic Ketoacidosis and Hyperglycemic Hyperosmolar Nonketotic Syndrome EtiologyDocument2 pagesPathophysiology of Diabetic Ketoacidosis and Hyperglycemic Hyperosmolar Nonketotic Syndrome EtiologyJaylord VerazonNo ratings yet
- Pathophysio Chronic GlomerulonephritisDocument1 pagePathophysio Chronic GlomerulonephritisRan Ma100% (1)
- PathophysiologyDocument1 pagePathophysiologynitlihpNo ratings yet
- Pathophysiology CVD InfarctDocument1 pagePathophysiology CVD InfarctElisa KerrNo ratings yet
- Esophagea L Cancer: By: Krizzia S. Bunagan-Legasi, RNDocument20 pagesEsophagea L Cancer: By: Krizzia S. Bunagan-Legasi, RNAnn SalvatierraNo ratings yet
- CHOLANGITISDocument1 pageCHOLANGITISKirk Torregosa PañaresNo ratings yet
- Bladder CancerDocument1 pageBladder CancerCarmina AguilarNo ratings yet
- Diabetes PathoDocument2 pagesDiabetes Pathodrewcel100% (1)
- Hypertensive Cardiovascular Disease Also Known As Hypertensive Heart Disease Occurs Due To The Complication of Hypertension or High Blood PressureDocument3 pagesHypertensive Cardiovascular Disease Also Known As Hypertensive Heart Disease Occurs Due To The Complication of Hypertension or High Blood Pressurejoanneceline16No ratings yet
- Ineffective Tissue Perfusion PDFDocument4 pagesIneffective Tissue Perfusion PDFgcodouganNo ratings yet
- Chronic Kidney Disease: A. Pathophysiology A. Schematic DiagramDocument3 pagesChronic Kidney Disease: A. Pathophysiology A. Schematic DiagramDaniel GeduquioNo ratings yet
- Pathophysiology CAP and HTNDocument5 pagesPathophysiology CAP and HTNLeonaPunzalanNo ratings yet
- Cva Concept MapDocument1 pageCva Concept MapAnn Justine OrbetaNo ratings yet
- CVA PathophysiologyDocument3 pagesCVA Pathophysiologyshmily_0810No ratings yet
- Diabetes PathophysiologyDocument2 pagesDiabetes PathophysiologyRyan MulanoNo ratings yet
- Diabetes Mellitus: Hyperglycemia (304 MG/DL, 13.2 MG/DL)Document3 pagesDiabetes Mellitus: Hyperglycemia (304 MG/DL, 13.2 MG/DL)John Henry ValenciaNo ratings yet
- Anatomy and Physiology-AppendicitisDocument3 pagesAnatomy and Physiology-AppendicitisMaria Socorro Sismundo DavidNo ratings yet
- NCP CvaDocument4 pagesNCP CvaMariquita BuenafeNo ratings yet
- NCP 2 CabalunaDocument7 pagesNCP 2 CabalunaIrene Grace BalcuevaNo ratings yet
- Nephrosclerosis PathophysiologyDocument14 pagesNephrosclerosis PathophysiologyAllene Paderanga0% (1)
- Anatomy and Physiology For Bacterial MeningitisDocument4 pagesAnatomy and Physiology For Bacterial MeningitisynecesityNo ratings yet
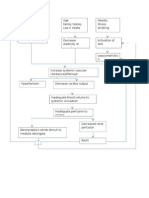
- Age Greater Than 60 Y/o Hereditary Precipitating Factors: Hypertension Increase Protein and Fat IntakeDocument3 pagesAge Greater Than 60 Y/o Hereditary Precipitating Factors: Hypertension Increase Protein and Fat Intakenursing concept mapsNo ratings yet
- Pathophysiology of Inflammatory ResponseDocument1 pagePathophysiology of Inflammatory ResponseDeo FactuarNo ratings yet
- Schematic Diagram: Signs and Symptoms: Headache, Unconsciousness, Nausea and Vomiting, Visual DisturbancesDocument3 pagesSchematic Diagram: Signs and Symptoms: Headache, Unconsciousness, Nausea and Vomiting, Visual DisturbancesJosett RomanoNo ratings yet
- CeVD, MI, HCVD & Atrial Fibrillation PathophysiologyDocument3 pagesCeVD, MI, HCVD & Atrial Fibrillation PathophysiologyJjessmar Bolivar FamaNo ratings yet
- Cancer Pathophysiology FinalDocument3 pagesCancer Pathophysiology FinalAngelique Ramos Pascua100% (1)
- Patof DMDocument1 pagePatof DMxerwaneNo ratings yet
- AldazideDocument2 pagesAldazideianecunarNo ratings yet
- Liver Case StudyDocument6 pagesLiver Case StudyGhulam MustafaNo ratings yet
- Cystic Mass PathophysiologyDocument1 pageCystic Mass PathophysiologyMa Cheryll DueñasNo ratings yet
- The Ride of Your Life: What I Learned about God, Love, and Adventure by Teaching My Son to Ride a BikeFrom EverandThe Ride of Your Life: What I Learned about God, Love, and Adventure by Teaching My Son to Ride a BikeRating: 4.5 out of 5 stars4.5/5 (2)
- Syok Kardiogenik Dr. Rani Maliawan, SP JPDocument59 pagesSyok Kardiogenik Dr. Rani Maliawan, SP JPLuh Leni AriniNo ratings yet
- DR Anuj Raj BijukchheDocument95 pagesDR Anuj Raj BijukchheMUHAMMAD JAWAD HASSANNo ratings yet
- Refreshing Shock: Pembimbing: Dr. Fauzi Abdillah Susman, SP - An, MSC Disusun Oleh: Achmad Reza SyamsuladeDocument14 pagesRefreshing Shock: Pembimbing: Dr. Fauzi Abdillah Susman, SP - An, MSC Disusun Oleh: Achmad Reza SyamsuladeSam.No ratings yet
- 2ND Quarterly Meeting For BbiDocument4 pages2ND Quarterly Meeting For BbiRuth PerezNo ratings yet
- Mary Janet C. Gorriceta Blk. 21 Zone 3 Bo - Obrero Iloilo City Mobile #: 09302029037 E-Mail AddressDocument8 pagesMary Janet C. Gorriceta Blk. 21 Zone 3 Bo - Obrero Iloilo City Mobile #: 09302029037 E-Mail AddressDick Morgan FerrerNo ratings yet
- CHN 113 LecDocument5 pagesCHN 113 LecGEOMHAI CATBAGANNo ratings yet
- Clinical Evaluation of Trikatu Kumari As Hypolipidemic DrugDocument7 pagesClinical Evaluation of Trikatu Kumari As Hypolipidemic Drugvietthang70No ratings yet
- Chapter 6Document68 pagesChapter 6Restie TeanoNo ratings yet
- Test Bank For Comprehensive Medical Assisting Administrative and Clinical Competencies 6th Edition Wilburta Billie Q Lindh Carol D Tamparo Barbara M Dahl Julie Morris Cindy CorreaDocument13 pagesTest Bank For Comprehensive Medical Assisting Administrative and Clinical Competencies 6th Edition Wilburta Billie Q Lindh Carol D Tamparo Barbara M Dahl Julie Morris Cindy Correadonnamcbride10021996wqk100% (26)
- Top 5 Best Ayurvedic Medicine Shop in Dubai 2021 HG Reviews & CompareDocument1 pageTop 5 Best Ayurvedic Medicine Shop in Dubai 2021 HG Reviews & CompareChaitanya RaisinghaniNo ratings yet
- Ebn StrokeDocument10 pagesEbn StrokeChristian Jake PaomeyNo ratings yet
- Aphasia HandoutDocument24 pagesAphasia HandoutArielena DuranNo ratings yet
- Mobileframe Healthcare Application Suite: Configurable Mobile ApplicationsDocument4 pagesMobileframe Healthcare Application Suite: Configurable Mobile ApplicationsSteveEpsteinNo ratings yet
- Guardian - Dental PPO Plan Summary 2022Document4 pagesGuardian - Dental PPO Plan Summary 2022Jessi ChallagullaNo ratings yet
- Body of Evidence: The History of Forensic MedicineDocument4 pagesBody of Evidence: The History of Forensic MedicineRisty Tuballas AdarayanNo ratings yet
- Patch TestingDocument1 pagePatch Testing26 ThufailNo ratings yet
- Daftar PustakaDocument2 pagesDaftar PustakaDasep PadilahNo ratings yet
- Form 2D Health Plan Implementation Pregnancy Prenatal CareDocument2 pagesForm 2D Health Plan Implementation Pregnancy Prenatal CareLora CarpioNo ratings yet
- Curriculum Vitae Muhammad Zakria Zakar, PHD: CV - Professor M. ZakarDocument13 pagesCurriculum Vitae Muhammad Zakria Zakar, PHD: CV - Professor M. ZakarMirza Khurram BaigNo ratings yet
- Dental Clinic - ResearchDocument10 pagesDental Clinic - ResearchAmorphus ViNo ratings yet
- Dr. Rath S Cellular Health ProgramsDocument21 pagesDr. Rath S Cellular Health ProgramsSilambarasu Karuppiah100% (1)
- Hygienic Requirements of Food and Drink EstablishmentsDocument25 pagesHygienic Requirements of Food and Drink Establishmentssneh7335No ratings yet
- Drug Study: Republic of The Philippines City of Makati University of Makati College of Allied Health StudiesDocument35 pagesDrug Study: Republic of The Philippines City of Makati University of Makati College of Allied Health StudiesKrystel PeñosoNo ratings yet
- Manuel - Lab Post TaskDocument1 pageManuel - Lab Post TaskShawn ManuelNo ratings yet
- Metacognitive Reading Report # 1: General InstructionsDocument2 pagesMetacognitive Reading Report # 1: General InstructionsSeth Jarl G. AgustinNo ratings yet
- Accepted Manuscript: Epilepsy ResearchDocument14 pagesAccepted Manuscript: Epilepsy ResearchSyedNo ratings yet
- NCPDocument4 pagesNCPJanella Kyle ParejaNo ratings yet
- Per Bech: The Bech, Hamilton and Zung Scales For Mood DisordersDocument85 pagesPer Bech: The Bech, Hamilton and Zung Scales For Mood DisordersKmoespinoNo ratings yet
- Quality Standards For Urban Primary Health CentreDocument284 pagesQuality Standards For Urban Primary Health CentreGajendra TodakarNo ratings yet
- Chemical Leukoderma To Hair DyeDocument2 pagesChemical Leukoderma To Hair DyeCHONG WEI SHENGNo ratings yet